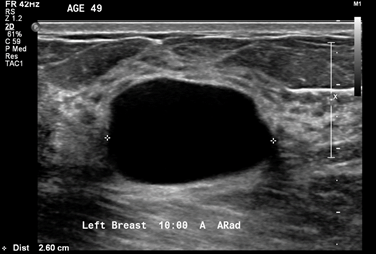
- The patient has a BIRADS 2 simple cyst
- To be regarded as a simple cyst, a breast nodule must meet three criteria:
- The margins must be circumscribed:
- i.e., a margin “that is well defined or sharp, with an abrupt transition between the lesion and surrounding tissue”
- It must be anechoic:
- i.e., “without internal echoes”
- It must show posterior acoustical enhancement:
- i.e., “a column that is more echogenic deep to the mass”
- The margins must be circumscribed:
- Simple cysts:
- Are almost never associated with cancer in the absence of other abnormalities seen on mammogram or ultrasound
- There are numerous reflectors in breast tissue, and all of the sound waves that are reflected do not make it back to the transducer:
- Many of them bounce back and forth (reverberate) between reflectors in the tissue, and with each reverberation, part of the echoes return to the transducer, are recorded, and part undergo another excursion between the reflectors
- Most of these echoes are obscured by all of the other echoes in the tissue, but when an otherwise anechoic window (a cyst) is present:
- The reverberation echoes can be seen in the anterior part of the cyst:
- In the image shown, a hyperechoic band can be seen within or just above the anterior wall of the cyst, especially on the left side of the image:
- The acoustic mismatches between this band and the less echogenic tissue superficial to it and the anechoic fluid deep to it, cause echoes that reverberate, creating the artifact in the near field of the cyst
- In the image shown, a hyperechoic band can be seen within or just above the anterior wall of the cyst, especially on the left side of the image:
- The reverberation echoes can be seen in the anterior part of the cyst:
- References
- D’Orsi CJ, Sickles EA, Mendelson EB, Morris EA. ACR BI-RADS® Atlas: Breast Imaging Reporting and Data System, 5th ed. Reston, VA: American College of Radiology; 2013.
- Kremkau FW. Diagnostic Ultrasound: Principles and Instruments, 7th ed. Elsevier; 2006:274-292. 1Image/Figure 2: Click on space below to upload image. Use highest available resolution and file size .png format: recommended .jpg format: acceptable .gif format: only recommended for text-based images and basic black and white charts Image/Figure 2 Reprint Permission: Obtain required reprint permissions when using copyrighted material Courtesy of the American Society of Breast Surgeons Breast Ultrasound Certification Reviewers.☐ Reprint permission obtained/attached Image/Figure 2 Caption: Include brief, informative caption for image/figure Ultrasound imaging of the palpable lesion.
#Arrangoiz #BreastSurgeon #CancerSurgeon #BreastCancer #CASO #CenterforAdvancedSurgicalOncology