My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
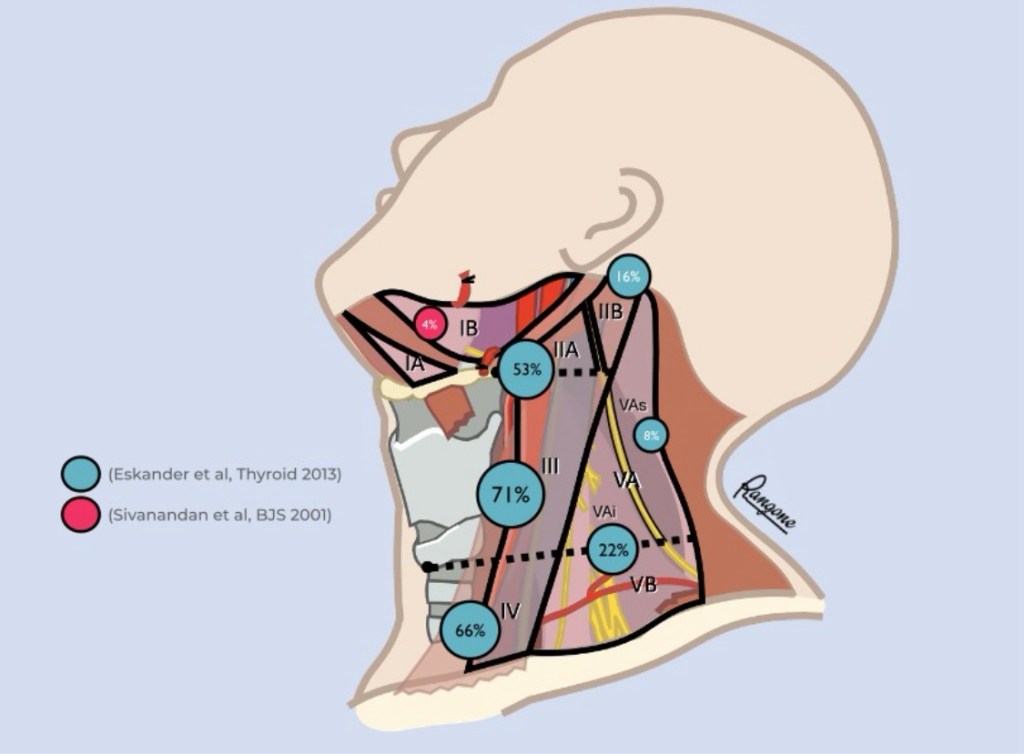
What lymph node levels does a lateral [comprehensive / therapeutic] neck dissection for differentiated thyroid cancer (DTC) include?
Although the rate of clinical nodal involvement in the lateral compartment was initially described by Japanese (Noguchi et al. 1970) and Germans (Gimm et al. 1998):
Sivanandan et al (2001) were the first to systematize it by levels
In 2013, the Canadian group of Jeremy L. Freeman (Eskander et al. Thyroid) conducted a systematic review that included the meta-analysis of 18 publications (including his 2012 retrospective work with 185 patients; Merdad et al. Head Neck) agglutinating 1298 lateral neck dissections for DTC:
Although heterogeneity was a constant in all comparisons by levels (I2: 31% to 87%), it is the best evidence to date that justifies the use of selective emptying IIa-Vb in this cohort of patients with this pathology:
Level III is the most frequently compromised
The majority (73%) of patients have more than one level involved:
Level III and IV:
46%
Level II, III and IV:
26%
Level III, IV and V:
11%
Level II, III, IV and V:
13% (Merdad et al. 2012)
Levels I and sublevel Va (cranial to the distal spinal nerve pathway):
Are rarely involved, usually in patients with high disease volume and multilevel invasion
Emptying of sublevel IIb (retrospinal recess):
Is usually indicated when clinical, radiological or macroscopic involvement is evident intraoperatively
The macroscopic involvement evident in the intraoperative sublevel IIa usually determines the addition of sublevel IIb to the neck dissection
“Skip metastases” within the lateral compartment are uncommon and occur in around 9% of patients:
Level II with level III and IV
Level V with level III and IV
(Merdad et al. 2012)
Selective lymphadenectomy IIa to Vb currently dissects levels IIa, III, IV, Vb and the “infraspinal” portion of the VA [VAi] in order to avoid the functional sequelae of cranial nerve XI dissection
Key Sonographic Features Suggestive of Malignancy:
Based on contemporary radiology references:
Hypoechoic echotexture
Posterior acoustic shadowing
Irregular or spiculated margins
Angular or microlobulated margins
Taller-than-wide orientation:
Non-parallel to skin
Thick echogenic halo:
Suggests desmoplastic reaction
Ductal extension or branching pattern
Intra-lesional calcifications
Increased stiffness on elastography:
High shear-wave values
Low apparent diffusion doefficient (ADC) values on diffusion-weighted imaging (DWI)
These align with standard teaching but are now reinforced by quantitative imaging advances such as elastography and DWI
Caveats — Not Exclusively Malignant:
Well-defined smooth borders and posterior acoustic enhancement can appear in both benign and malignant lesions:
Interpretation must rely on the whole feature set
Layering or “teacup” micro-calcifications on mammography typically lean benign, despite ultrasound appearance; correlation remains essential
Integrated Imaging Approach:
A sonographic mass that appears benign on mammography should be evaluated primarily based on B-mode ultrasound features rather than mammographic impression
Use of color Doppler improves specificity for malignancy in non-mass-like lesions without reducing sensitivity
Quantitative Imaging Enhancements:
Diffusion-weighted imaging (DWI):
Apparent Diffusion Coefficient (ADC) values provide quantitative assessment:
Malignant lesions typically show mean ADC ≈ 1.03 ×10⁻³ mm²/s, benign ≈1.5 ×10⁻³ mm²/s; ADC <1.0 ×10⁻³ mm²/s strongly favors malignancy
Recent meta-analysis confirms ADC’s usefulness for distinguishing lesions, though exact thresholds vary:
Most protocols now use ≥ 1.5T MRI with b-values around 800 s/mm²
Shear-wave elastography (SWE):
Mean values for malignancies often exceed 133 to 153 kPa (e.g., ~167 kPa), aiding differentiation
Full References:
Malherbe K. Breast Ultrasound. StatPearls, updated 2024 – Highlights classic sonographic features: hypoechoic texture, shadowing, margins, etc Verywell Health, “Breast Cancer Ultrasound: How It Works and What Results Mean.” (2022) – Discusses overlap of benign/malignant features and interpretive context.
Tarigan VN et al. 2025 systematic review: DWI (ADC) helps distinguish benign vs malignant lesions; ADC measurement challenges remain. Kwon M et al. (2024) – Mean ADC ~0.982 ×10⁻³ mm²/s for cancers; SWE stiffness ~167.7 kPa. Surov A et al. (2019) – Pooled ADC values show malignant lesions average 1.03 ×10⁻³ mm²/s vs benign 1.5 ×10⁻³ mm²/s; benign rarely under 1.0 ×10⁻³ mm²/s.
Stavros AT. Breast Ultrasound, 2004 – Covers foundational ultrasound interpretation concepts. Cardenosa G. Clinical Breast Imaging: The Essentials, 2015 – Classic reference listing the ten ultrasound signs of malignancy.
Tarigan VN et al. (2024) Frontiers in Oncology – Color Doppler specificity enhancement in non-mass lesions.
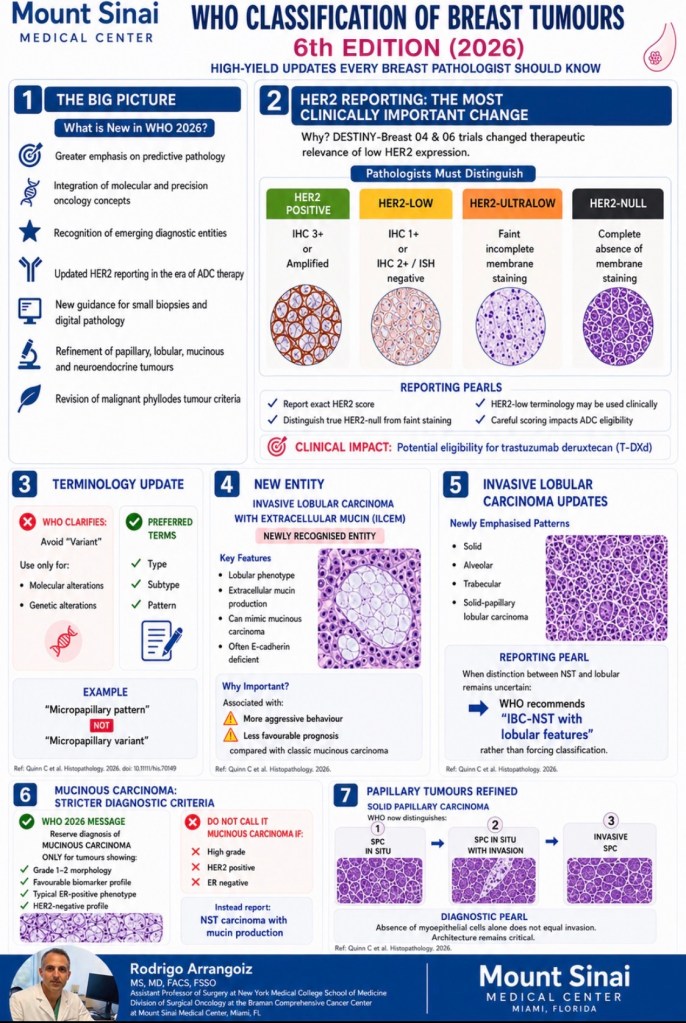
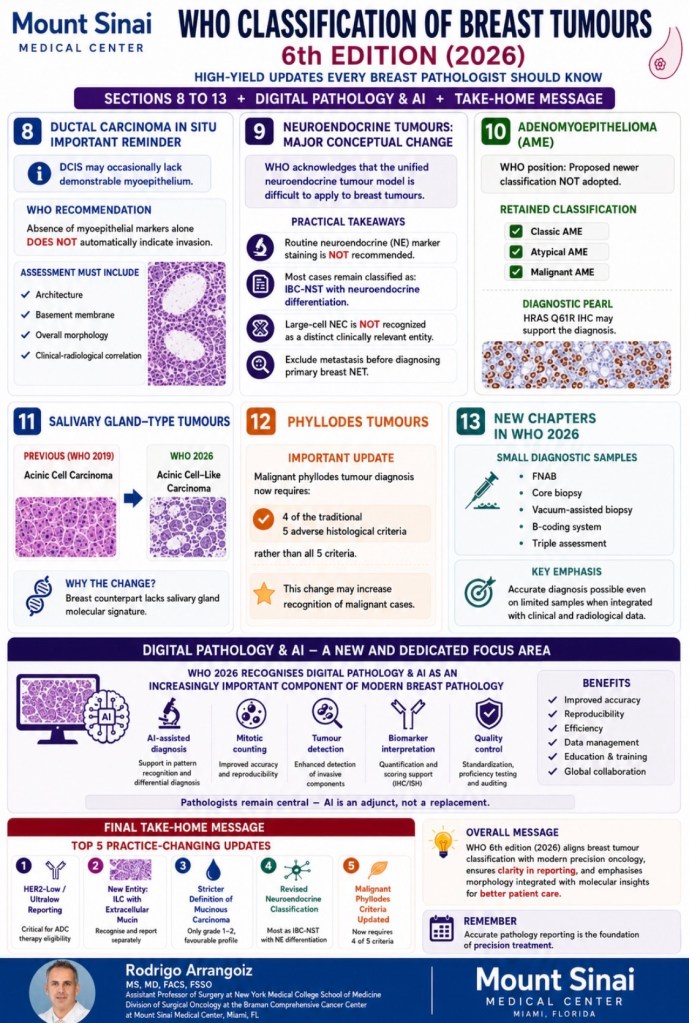
Summary of the major updates in the WHO Classification of Tumors of the Breast, 6th Edition (2026) as they pertain to invasive lobular carcinoma (ILC) and related changes
Key ILC-Specific Changes:
ILC with Extracellular Mucin (ILCEM) — New Diagnostic Entity:
The most significant ILC-related change is the formal recognition of ILC with extracellular mucin (ILCEM) as a distinct diagnostic entity with prognostic implications:
This rare subtype, first described in 2009, is characterized by lobular-phenotype tumor cells (single cells, cords, nests, trabeculae) floating within pools of extracellular mucin
Key features include:
Typically presents as a large mass (> 2 cm) in postmenopausal women:
Often shows high nuclear grade (grade 2 to 3), signet-ring cell morphology, pleomorphic features, solid growth patterns
E-cadherin is absent or aberrant on IHC, with cytoplasmic p120 catenin localization confirming lobular phenotype in both mucinous and non-mucinous components
All reported cases are ER-positive, with a higher rate of HER2 positivity than classic ILC
Molecularly, ILCEM harbors CDH1 alterations in ~ 92% of cases, along with PIK3CA, RUNX1, AKT1, and PTEN mutations:
Cases with recurrences show additional ERBB2, ERBB3, TP53, and FGFR1 alterations
Worse prognosis than classic ILC:
52% recurrence rate and ~ 30% disease-specific mortality in reported series
The WHO 6th Edition (2026) introduces a critical terminological change for ILC:
The term “variant” is now reserved exclusively for molecular / genetic alterations:
While morphological differences in ILC are reclassified as architectural patterns or cytomorphological subtypes rather than “variants”;
This represents a significant conceptual shift from the 5th edition framework
Terminology Update: “Variant” vs. “Pattern/Subtype”:
In the WHO 5th edition, ILC morphological forms were called “variants”
The 6th edition clarifies that “variant” should now refer only to molecular / genetic alterations (e.g., CDH1 mutations, PIK3CA mutations):
While the morphological diversity of ILC is described using terms like “pattern” or “subtype”:
This aligns breast pathology terminology with broader WHO classification principles across organ systems
Architectural Patterns of ILC:
ILC architectural patterns are categorized based on growth pattern and cytomorphology:
Growth pattern-based:
Classic:
The most common pattern, characterized by small, dyscohesive cells with monomorphic nuclei and scant cytoplasm
Arranged in single cells, single files, and targetoid infiltrations around ducts and lobules, with little or no stromal reaction
Two cell types exist within classic ILC:
Type A cells – monomorphic, pleomorphism score 1
Type B cells – larger, vesicular, pleomorphism score 2
Solid:
Sheets of dyscohesive lobular cells growing in solid nests without fibrovascular cores or a fibrous capsule
Associated with higher Ki67 and more aggressive behavior
High-grade solid ILC is grouped with pleomorphic ILC as an aggressive subtype
Alveolar:
Cells arranged in rounded nests of ~ 20 cells resembling alveolar structures; often mixed with other patterns
Tubulolobular:
Features small tubular structures admixed with classic lobular single-file growth
Trabecular:
Trabeculae mainly 2 to 3 cells thick (first described by Martinez and Azzopardi in 1979)
Prognosis appears similar to classic ILC
Solid papillary:
A recently described pattern with circumscribed nodules containing fibrovascular cores, distinct from solid ILC (which lacks fibrovascular cores)
May express neuroendocrine markers (synaptophysin, chromogranin)
Shows higher post-endocrine therapy Ki67 levels
ILC with tubular elements (ILC-TE):
A recently identified pattern defined by noncohesive carcinoma cells mixed with cohesive tubular elements, with complete E-cadherin loss but P-cadherin upregulation (E-cadherin to P-cadherin switch, or EPS) in tubular areas
Accounts for ~ 7.5% of ILC and is associated with less-aggressive features (lower grade, lower Ki67, cT1, cN0)
Cytomorphology-based:
Pleomorphic:
High nuclear grade (pleomorphism score 3), accounting for < 1% of all breast cancers
Associated with worse prognosis than classic ILC and even IBC-NST, with frequent ERBB2 and PIK3CA mutations
Histiocytoid / apocrine:
Cells with abundant eosinophilic or granular cytoplasm resembling histiocytes
New Entity: ILC with Extracellular Mucin (ILCEM):
The 6th edition formally recognizes ILCEM as a distinct diagnostic entity:
Lobular-phenotype cells floating within pools of extracellular mucin, confirmed by absent /aberrant E-cadherin and cytoplasmic p120 catenin
This carries worse prognosis than classic ILC (52% recurrence rate)
Prognostic Stratification by Pattern:
A large cohort study (n = 7,140) identified that pleomorphic ILC and high-grade solid ILC together comprise ~ 14% of ILC cases and constitute an aggressive subtype with worse breast cancer-specific survival and disease-free survival compared to both classic ILC and IBC-NST:
Notably, adjuvant chemotherapy did not improve outcomes in this aggressive subgroup
Classic ILC and its related patterns (alveolar, trabecular, papillary, tubulolobular) had significantly better survival than IBC-NST in the first 10 to 15 years of follow-up
Significant increase in incidence after mammography screening:
10-fold to 17-fold increase from 1970’s to 2004:
1 in 1300 mammograms
Represents 20% to 25% of all screen-detected breast neoplasias diagnosed annually
Based on autopsy data:
The prevalence of undetected DCIS may exceed 20% in women over 40:
Underscoring the concern for overdiagnosis:
Modeling studies estimate up to 65% of DCIS may be overdiagnosed
DCIS by it self:
Is not a risk to life
DCIS may progress to invasion and compromise survival:
If left untreated:
1 in 6 DCIS patients:
Progress to invasive breast cancer (IBC):
70% estimated to remain indolent
At this time we do not have any robust biomarkers:
That can quantify the risk of progression to IBC or
Help us separate indolent disease:
From the potentially dangerous lesions
Risk of overtreament:
The increase incidence of DCIS in mammographically detected cases:
Has not lead to a decrease in the incidence of IBC or reduction of IBC morality
Risk factors for progression / recurrence of DCIS:
The risk factors for IBC recurrence may be different from the risks factors for DCIS recurrence?
Risk of IBC recurrence:
African American race
Premenopausal status
Detection by palpation
Involved margins
High histologic grade
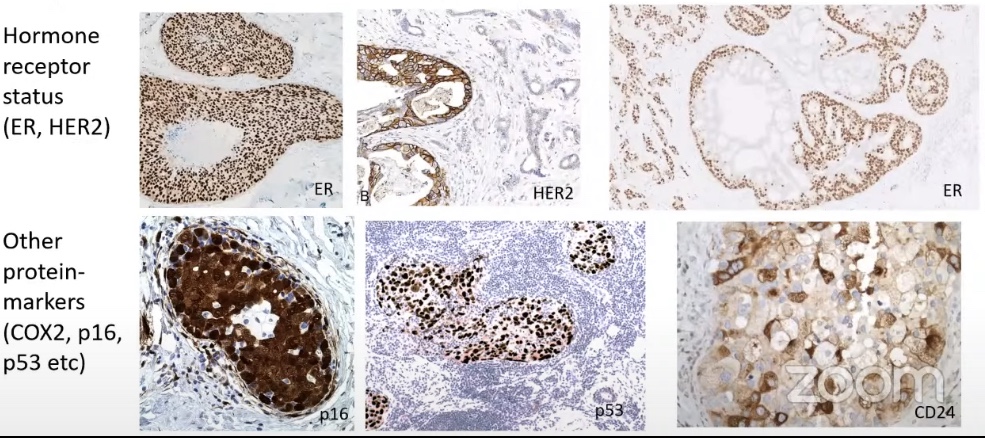
High p16 expression
Risk of IBC or DCIS recurrence:
DCIS size
Histology type
Comedo necrosis
Grade (High)
Young age
Close margins or positive margins
Patients with DCIS that recur with an IBC:
Some patients with DCIS may develop:
Progression of there disease:
30% (1 out of 6)
Some will have a de novo invasive breast cancer
Some might have a missed invasive cancer?
Patient that have a DCIS recurrence:
Might be a true in situ recurrence
De novo DCIS
Residual disease?
Studies are describing observations of events like:
Synchronous IBC
Subsequent ipsilateral or contralateral DCIS or IBC (often a mixture)
We have limited data on DCIS progression with paired molecular profiles
The most consistent biological feature of DCIS:
Heterogeneity:
In clinical presentation
Morphology
Protein expression:
Including receptor status
Gene expression
Genetic alterations
Epigenetic alterations
The heterogeneity is:
Between patients – within the lesion – and within cells in a single duct
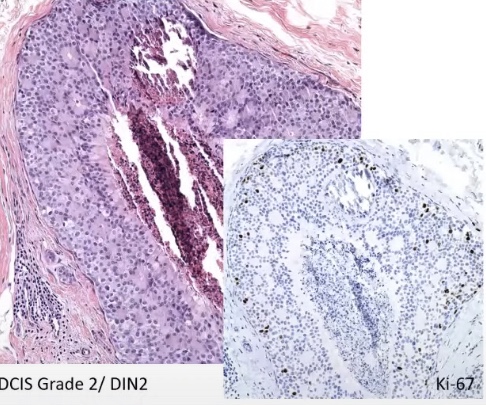
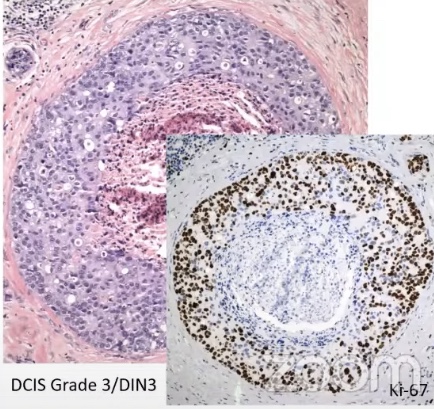
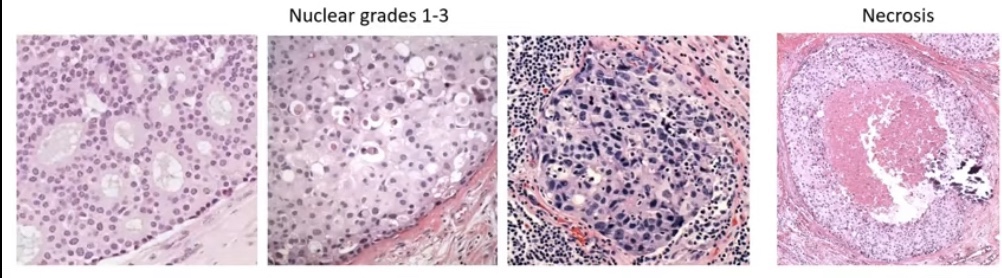
Morphological features that help us predict progression are:
Histologic grading:
Combing the nuclear grade 1 to 3 and necrosis into a three tier system (the good, the bad, and the ugly):
Low / intermediate / high grade
Grade 1 to 3
Van Nuys Group 1 to 3
DIN 1 to 3
We all know that there is regression towards the mean and substantial interobserver variation
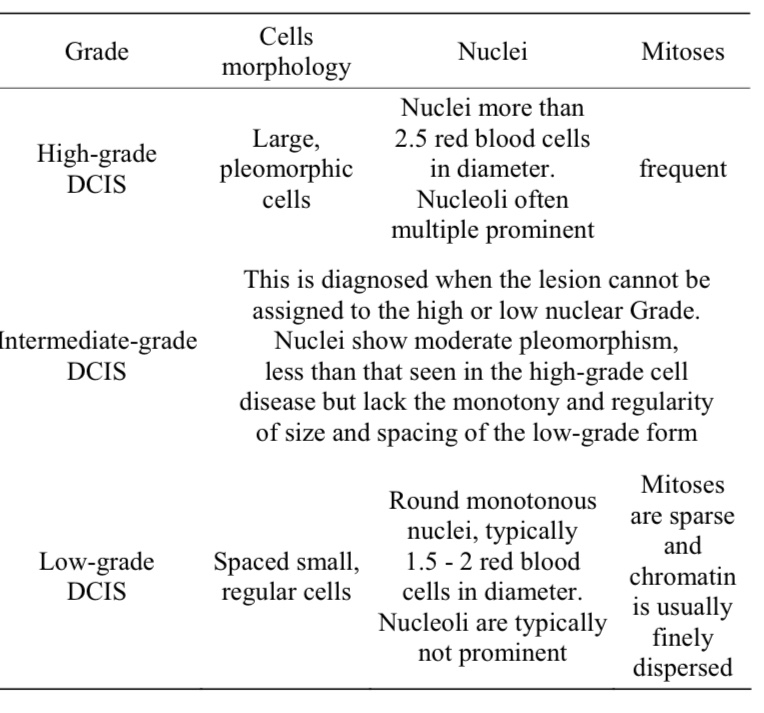
DCIS is classified by two complementary systems:
Nuclear grade (the primary classification):
Low (grade I), intermediate (grade II), and high (grade III):
Based on nuclear size, pleomorphism, chromatin pattern, nucleoli, mitotic activity, and cell polarization
Nuclear grade is the most reproducible and clinically relevant parameter
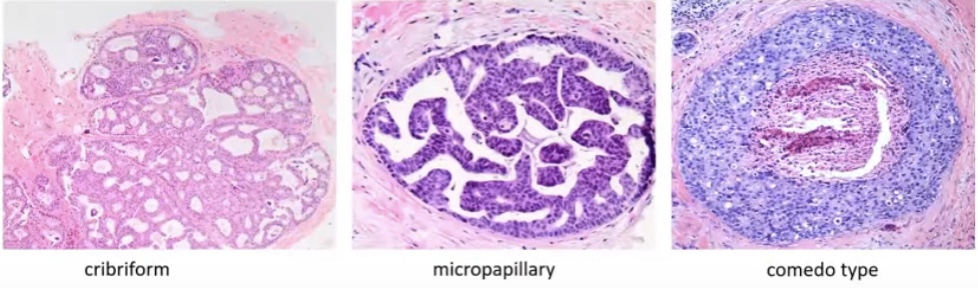
Architectural pattern (secondary / noncore):
Solid, cribriform, micropapillary, papillary, and comedo:
Multiple patterns frequently coexist within a single lesion, limiting reproducibility
Morphologic Features Suggestive of Progression
Unclear prognostic value of the 3-tier system:
We suspect that:
Low to intermediate grade = low risk of progression
High grade system = high risk of progression or shorter time to progression
Maxwell, A.J. Eur.J.Surg.Oncol.,2018, Ryser, MD. J.Natl Cancer Inst., 2019:
Risk of ipsilateral recurrence (DCIS / IBC) at 10 years:
High grade 17.6% (95% CI=12.1-25.2%)
Non high grade 12.2 (95% CI=8.6-17.1%):
Including grade 2
There is overlap in the confidence intervals
Low grade DCIS are the lesions that might have:
Discontinuous growth (multifocal gaps up to 1 cm) and skip lesions that might lead to a:
Greater likelihood of residual disease and recurrence?
DCIS has heterogeneity of grade within the same lesion
Histologic subtype as a prognostic factor:
Subtype:
Cribriform:
Is more often a grade 1 lesion
Comedo type:
Is more often a grade 3 lesion
Usually histology subtype correlates with grade but:
There is often a mixture of growth patterns:
Compromising the use for prognostication
Can we use histology as a prognostic feature?
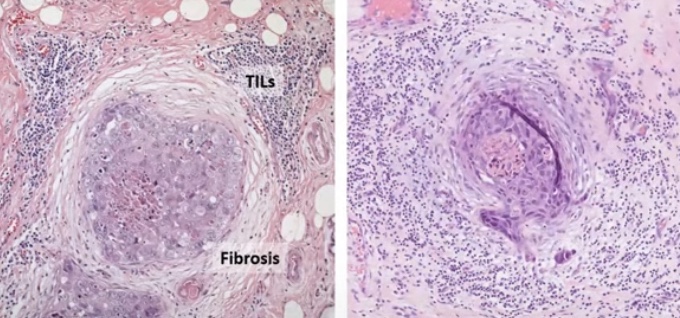
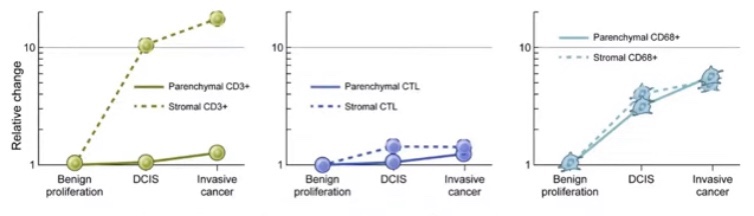
Tumor micro environment:
Could potentially be the most important morphologic feature suggestive of progression especially:
Circumferential periductal fibrosis and associated tumor infiltrating lymphocytes (TIL):
Indicating host reaction to the tumor cells
Tumor micro environment includes:
Myoepithelial cell layer
Tumor infiltrating lymphocytes (TIL)
Adipocytes
Fibroblasts
Matrix
The border around the myoepithelial layer might have prognostic value
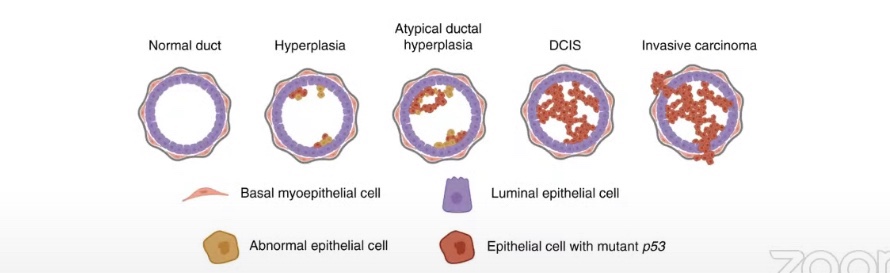
The myoepithelial cell layer acts as a gatekeeper:
Has tumor suppressive functions
The largest gene expression change from normal tissue to DCIS:
Occurs in the myoepithelial cell layer
DCIS is associated myoepithelial cell loss:
That leads the decrease tumor suppressor functions
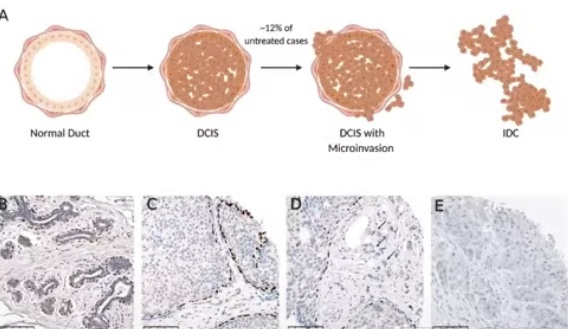
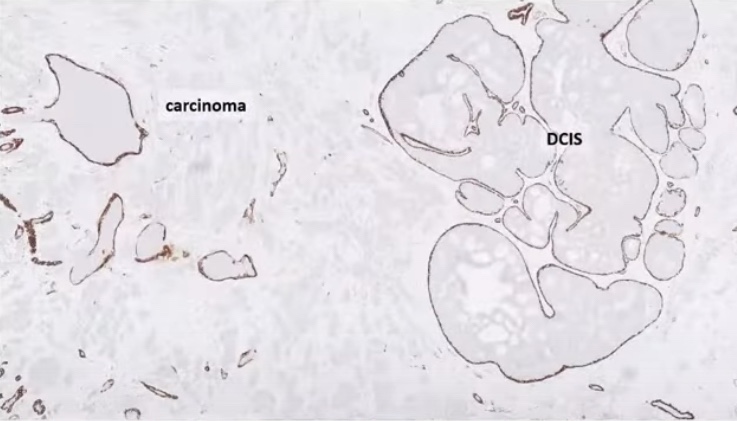
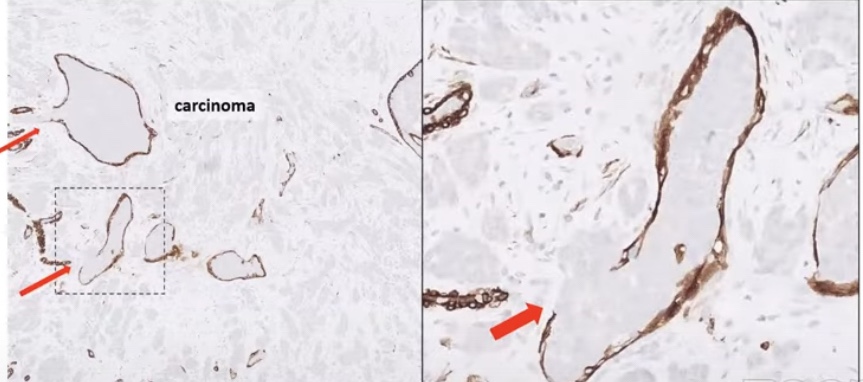
The myoepithelial cell layer is lost in IBC
Myoepithelial cell layer acts as a GATEKEEPER (Tumor Suppressive Functions)
Disruption of the myoepithelial defense:
IBC with DCISBrown color – myoepithelium Arrows point to the disrupted myoepithelial cell layer (micro-invasion)
Conflicting data on prognostic value of TIL:
Some studies have reported no prognostic value of stromal TIL for subsequent recurrences:
Does the spatial location of the immune cells matter?
The TIL in direct contact with the DCIS might be more important that the TIL that are further away
Other studies have shown a correlation between higher levels of TIL and increased risk of subsequent IBC and a shorter (ipsilateral) recurrence-free survival
The eighth edition of the American Joint Committee on Cancer (AJCC) staging system:
Defines microinvasion as:
Invasion of breast cancer cells:
Through the basement membrane at one or more foci:
None of which exceeds a dimension of 1 mm
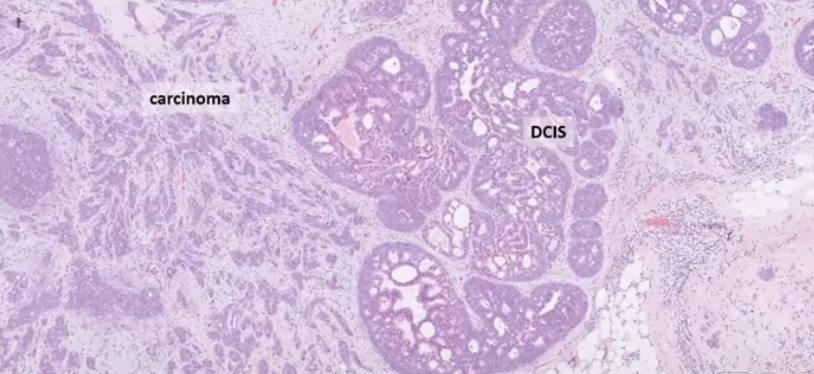
DCIS:
Is a Tis lesion:
Is classified as stage 0 cancer
DCIS with microinvasion is considered:
T1mi:
Upstages DCIS from stage 0 to stage I disease:
The earliest stage of invasive cancer:
In the AJCC staging system
By definition:
DCIS does not have the ability to metastasize to axillary lymph nodes or distant sites:
Whereas DCIS with microinvasion does
Axillary metastasis:
Has been reported in 0% to 20% (0% to 28% in some series) of patients:
With DCIS with microinvasion
The incidence of microinvasion in DCIS:
Varies according to:
The size and extent of the index lesion
Lagios et al. (1989):
Reported a 2% incidence of microinvasion in patients with DCIS:
Measuring ≤ 25 mm in diameter
Compared with a 29% incidence of microinvasion:
In those with lesions ≥ than 26 mm
The incidence of microinvasion is also higher in patients with:
High-grade or comedo-type DCIS with necrosis
In patients with DCIS who present with:
A palpable mass
Nipple discharge
Historically, patients with DCIS with microinvasion:
Have been observed to have a worse prognosis:
Compared with those who have DCIS alone
Mirza et al. (2000):
Reported the long-term results of breast-conserving therapy in patients with:
DCIS
DCIS with micro-invasion (T1mi)
T1 invasive breast cancers
The 20-year disease-specific survival rates in patients with:
DCIS were better:
Than those among patients with DCIS with microinvasion or with T1 invasive tumors
Patients with micro-invasion (T1mi) and those with T1 tumors:
Had similar survival rates
In a retrospective study of 1,248 serially sectioned DCIS tumors, de Mascarel et al. (2002):
Reported a 10.1% incidence of axillary metastases:
In cases of DCIS with microinvasion
Patients with DCIS had a better 10-year distant metastasis-free survival rate:
Than patients with DCIS with microinvasion:
98% and 91%, respectively
The overall survival rate was also better in patients with DCIS compared to DCIS with microinvasion:
96.5% vs. 88.4%
However, the metastasis-free and overall survival rates:
Were worse in patients with invasive ductal carcinoma compared with those with DCIS with microinvasion
These results suggest that DCIS with microinvasion:
Should be characterized as a small invasive tumor with a good outcome:
The therapeutic approach for these patients should be similar to that for patients with invasive cancer
However, more recent studies have pointed toward DCIS with microinvasion having a more similar natural history to pure DCIS than to early-stage invasive disease:
In a review of 393 patients treated at Yale between 1973 and 2004:
There was no statistically significant difference between patients with DCIS and those with DCIS with microinvasion with regard to the presence of axillary metastases (in those who had axillary staging) or the likelihood of recurrence (locoregional and distant) or overall survival (Parikh et al., 2012)
Perioperative Immunotherapy – KEYNOTE-689 Continues to Shape Practice:
The KEYNOTE-689 phase 3 trial:
Which led to the FDA approval of perioperative pembrolizumab (June 2025):
For resectable locally advanced HNSCC with PD-L1 CPS ≥ 1:
Remains a central focus
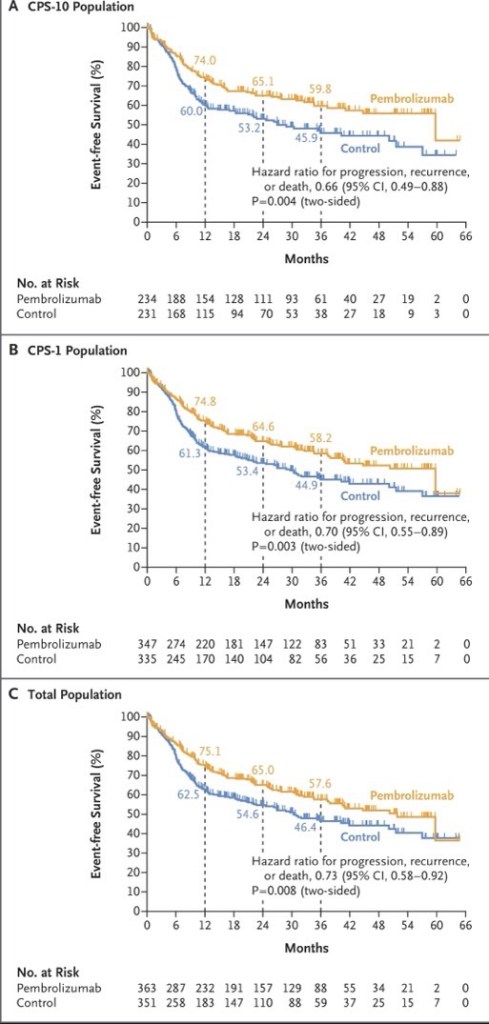
New ASCO 2026 exploratory analyses demonstrate that the EFS benefit of neoadjuvant / adjuvant pembrolizumab:
Persists across surgical outcome subgroups, including:
Patients with and without extranodal extension or positive margins
Notably, fewer patients in the pembrolizumab arm had ENE or positive margins post-surgery:
Suggesting neoadjuvant pembrolizumab contributes to pathologic downstaging
A pooled meta-analysis of three phase 3 trials (KEYNOTE-689, NIVOPOSTOP, and IMvoke010; n=1,786) presented at ASCO 2026:
Confirmed a significant improvement in event-free / disease-free survival with perioperative or adjuvant PD-1 / PD-L1 blockade (pooled HR 0.79, 95% CI 0.68–0.91):
With no meaningful increase in treatment-related deaths
The following figure from the KEYNOTE-689 trial illustrates the event-free survival benefit across PD-L1 subgroups:
Neoadjuvant Bispecific Antibody Combinations: Ivonescimab Leads the Way:
Several ASCO 2026 abstracts highlight the emerging role of bispecific antibodies in the neoadjuvant setting:
All patients with CPS >30 achieved pCR, and 100% laryngeal / pharyngeal preservation was achieved
A randomized phase II trial comparing ivonescimab (PD-1 / VEGF), cadonilimab (PD-1 /CTLA-4), and penpulimab (PD-1 alone), each combined with chemotherapy:
Showed the highest pCR rate with ivonescimab at 60%, compared to 42.1% with cadonilimab and 40% with single-agent PD-1
An 87.5% ORR and a 95.8% larynx preservation rate in resectable LA-HNSCC:
With all p16-positive and CPS ≥ 20 patients responding
Novel Agents in Recurrent / Metastatic HNSCC:
Bispecific antibodies are generating significant excitement in the recurrent / metastatic setting:
Ficerafusp alfa (EGFR × TGF-β) + pembrolizumab:
Two-year follow-up data showed a confirmed ORR of 54% in HPV-negative R/M HNSCC (21% CR), with a median DOR of 21.7 months and median OS of 21.3 months
The phase 2 / 3 FORTIFI-HN01 trial is now actively enrolling
Petosemtamab (EGFR × LGR5) + pembrolizumab:
Updated phase 2 data showed a 60% ORR (including 5 CRs) in first-line PD-L1+ R/M HNSCC, with median DOR of 11 months
Two phase 3 trials (LiGeR-HN1 and LiGeR-HN2) are recruiting
CRB-701 (Nectin-4 ADC):
A phase 1 / 2 study in heavily pretreated R/M HNSCC (85% refractory to immunotherapy and platinum):
Showed a confirmed ORR of 33.3% at both 2.7 and 3.6 mg/kg doses, regardless of HPV status
Becotatug vedotin (EGFR ADC):
A new randomized phase II trial is evaluating neoadjuvant becotatug vedotin alone or combined with immune checkpoint inhibitors in resectable LA-HNSCC
The deep response rate was 87.9%, with 86% of patients receiving de-escalated definitive therapy
At 23 months median follow-up, 2-year PFS was 86% and OS was 100%
Circulating tumor HPV-DNA was significantly associated with recurrence
Evolving First-Line R / M HNSCC Pipeline:
A landscape analysis presented at ASCO 2026 identified 145 active regimens (111 unique assets) in the first-line R / M HNSCC pipeline
Key trends include a shift toward chemotherapy-free combinations alongside PD-1 blockade:
With bispecific antibodies (10.8%), ADCs (10.8%), and cancer vaccines (9.0%) representing the most common novel modalities
Eight key phase 3 trials are underway:
All incorporating PD-1 as a target, with pembrolizumab as the backbone in 7 of 8
Overall, ASCO 2026 highlights a transformative period in head and neck oncology:
With perioperative immunotherapy now established as a new standard, bispecific antibodies and ADCs showing compelling early efficacy, and biomarker-driven strategies (PD-L1 CPS, HPV status, ctHPV-DNA, MRD) increasingly guiding treatment selection
References
Neoadjuvant and Adjuvant Pembrolizumab in Locally Advanced Head and Neck Cancer. Uppaluri R, Haddad RI, Tao Y, et al. The New England Journal of Medicine. 2025;393(1):37-50. doi:10.1056/NEJMoa2415434.
FDA approves neoadjuvant and adjuvant pembrolizumab for resectable locally advanced head and neck squamous cell carcinoma | FDA. Food and Drug Administration. 2025-06-13.
Neoadjuvant and adjuvant pembrolizumab (pembro) plus standard of care (SOC) for resectable locally advanced head and neck squamous cell carcinoma (LA HNSCC): Efficacy by surgical outcomes in the phase 3 KEYNOTE-689 trial.. Adkins D, Haddad R, Tao Y, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):6057. doi:10.1200/JCO.2026.44.16_suppl.6057.
Perioperative or adjuvant PD-1/PD-L1 blockade with curative-intent multimodality therapy for locally advanced head and neck squamous cell carcinoma: A systematic review and meta-analysis of randomized trials.. Daher S, Daher H, Altal H, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):e18074. doi:10.1200/JCO.2026.44.16_suppl.e18074.
Neoadjuvant ivonescimab (AK112, a PD-1/VEGF bispecific antibody) combined with nab-paclitaxel and cisplatin (AP) for resectable locally advanced head and neck squamous cell carcinoma (LA-HNSCC): An exploratory phase II study.. Kunyu Yang, Xiaomeng Zhang and Lu Wen. Journal of Clinical Oncology. 2026;44(Suppl 16):6014. doi:10.1200/JCO.2026.44.16_suppl.6014.
Neoadjuvant immunotherapy in combination with chemotherapy in resectable locally advanced head and neck squamous cell carcinoma: Updated efficacy and safety data from a randomized phase II trial.. Liu L, Chen F, Li Y, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):6091. doi:10.1200/JCO.2026.44.16_suppl.6091.
Neoadjuvant adebrelimab plus chemotherapy in untreated locally advanced head and neck squamous cell carcinoma: Efficacy and biomarker insights from a single-arm phase 2 trial.. Fang R, Lei W, Huang B, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):6106. doi:10.1200/JCO.2026.44.16_suppl.6106.
Ficerafusp Alfa (BCA101) With Pembrolizumab for Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma: Two-Year Results of an Expansion Cohort of a Phase I/Ib Trial. Hanna GJ, Zandberg DP, Wong DJ, et al. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2026;:JCO2502027. doi:10.1200/JCO-25-02027.
A multicenter, randomized, double-blind, phase 2/3 study of ficerafusp alfa (BCA101) or placebo in combination with pembrolizumab for first-line treatment of HPV-negative, PD-L1–positive, recurrent or metastatic (R/M) head and neck squamous cell carcinoma (HNSCC): FORTIFI-HN01.. Ferrarotto R, Kaczmar J, Spigel D, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):TPS6129. doi:10.1200/JCO.2026.44.16_suppl.TPS6129.
Petosemtamab (MCLA-158) with pembrolizumab as first-line (1L) treatment of PD-L1+ recurrent/metastatic (r/m) head and neck squamous cell carcinoma (HNSCC): Phase 2 trial. Herpen C, Daste A, Arrazubi V, et al. Journal of Clinical Oncology. 2025;43(Suppl 16):6024. doi:10.1200/JCO.2025.43.16_suppl.6024.
LiGeR-HN Phase III Trials of Petosemtamab + Pembrolizumab and Petosemtamab Monotherapy in Recurrent or Metastatic HNSCC. Machiels JP, Fayette J, Haddad R, et al. Future Oncology (London, England). 2025;21(16):2007-2016. doi:10.1080/14796694.2025.2511470.
A phase 1/2 study of the next-generation nectin-4–targeting antibody-drug conjugate CRB-701 (SYS6002) in patients with recurrent or metastatic head and neck squamous cell carcinoma.. Mantia C, Hanna G, Loriot Y, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):6062. doi:10.1200/JCO.2026.44.16_suppl.6062.
A randomized, non-comparative, multicenter phase II trial of neoadjuvant becotatug vedotin alone or combined with immune checkpoint inhibitors (penpulimab/ivonescimab) in resectable locally advanced head and neck squamous cell carcinoma.. Wei X, Xiang Z, Zeng Y, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):TPS6135. doi:10.1200/JCO.2026.44.16_suppl.TPS6135.
Neoadjuvant HPV16-specific viral immunotherapy (HB200) plus chemotherapy with response-adapted de-escalation in HPV16+ oropharyngeal squamous cell carcinoma: TARGET-HPV trial.. Rosenberg A, Juloori A, Cursio J, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):6097. doi:10.1200/JCO.2026.44.16_suppl.6097.
Emerging trends in research strategies in the first-line recurrent or metastatic head and neck cancer (R/M SCCHN) landscape: A top-level analysis by Oncofocus.. Shukla A, Keeshara V, Chamaria M, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):e18029. doi:10.1200/JCO.2026.44.16_suppl.e18029.
Recent Highlights and Breakthroughs in Immunotherapy for Head and Neck Cancers. Vuille JA, Szturz P. Current Opinion in Oncology. 2026;38(3):201-211. doi:10.1097/CCO.0000000000001211.
Immunotherapy in Locally Advanced Head and Neck Squamous Cell Carcinoma: The Current Status and Future Outlook. Köylü B, Selçukbiricik F, Aksoy S, Güven DC. Critical Reviews in Oncology/Hematology. 2026;:105145. doi:10.1016/j.critrevonc.2026.105145.
Perioperative Immunotherapy – KEYNOTE-689 Continues to Shape Practice:
The KEYNOTE-689 phase 3 trial:
Which led to the FDA approval of perioperative pembrolizumab (June 2025):
For resectable locally advanced HNSCC with PD-L1 CPS ≥ 1:
Remains a central focus
New ASCO 2026 exploratory analyses demonstrate that the EFS benefit of neoadjuvant / adjuvant pembrolizumab:
Persists across surgical outcome subgroups, including:
Patients with and without extranodal extension or positive margins
Notably, fewer patients in the pembrolizumab arm had ENE or positive margins post-surgery:
Suggesting neoadjuvant pembrolizumab contributes to pathologic downstaging
A pooled meta-analysis of three phase 3 trials (KEYNOTE-689, NIVOPOSTOP, and IMvoke010; n=1,786) presented at ASCO 2026:
Confirmed a significant improvement in event-free / disease-free survival with perioperative or adjuvant PD-1 / PD-L1 blockade (pooled HR 0.79, 95% CI 0.68–0.91):
With no meaningful increase in treatment-related deaths
The following figure from the KEYNOTE-689 trial illustrates the event-free survival benefit across PD-L1 subgroups:
Neoadjuvant Bispecific Antibody Combinations: Ivonescimab Leads the Way:
Several ASCO 2026 abstracts highlight the emerging role of bispecific antibodies in the neoadjuvant setting:
All patients with CPS >30 achieved pCR, and 100% laryngeal / pharyngeal preservation was achieved
A randomized phase II trial comparing ivonescimab (PD-1 / VEGF), cadonilimab (PD-1 /CTLA-4), and penpulimab (PD-1 alone), each combined with chemotherapy:
Showed the highest pCR rate with ivonescimab at 60%, compared to 42.1% with cadonilimab and 40% with single-agent PD-1
An 87.5% ORR and a 95.8% larynx preservation rate in resectable LA-HNSCC:
With all p16-positive and CPS ≥ 20 patients responding
Novel Agents in Recurrent / Metastatic HNSCC:
Bispecific antibodies are generating significant excitement in the recurrent / metastatic setting:
Ficerafusp alfa (EGFR × TGF-β) + pembrolizumab:
Two-year follow-up data showed a confirmed ORR of 54% in HPV-negative R/M HNSCC (21% CR), with a median DOR of 21.7 months and median OS of 21.3 months
The phase 2 / 3 FORTIFI-HN01 trial is now actively enrolling
Petosemtamab (EGFR × LGR5) + pembrolizumab:
Updated phase 2 data showed a 60% ORR (including 5 CRs) in first-line PD-L1+ R/M HNSCC, with median DOR of 11 months
Two phase 3 trials (LiGeR-HN1 and LiGeR-HN2) are recruiting
CRB-701 (Nectin-4 ADC):
A phase 1 / 2 study in heavily pretreated R/M HNSCC (85% refractory to immunotherapy and platinum):
Showed a confirmed ORR of 33.3% at both 2.7 and 3.6 mg/kg doses, regardless of HPV status
Becotatug vedotin (EGFR ADC):
A new randomized phase II trial is evaluating neoadjuvant becotatug vedotin alone or combined with immune checkpoint inhibitors in resectable LA-HNSCC
The deep response rate was 87.9%, with 86% of patients receiving de-escalated definitive therapy
At 23 months median follow-up, 2-year PFS was 86% and OS was 100%
Circulating tumor HPV-DNA was significantly associated with recurrence
Evolving First-Line R / M HNSCC Pipeline:
A landscape analysis presented at ASCO 2026 identified 145 active regimens (111 unique assets) in the first-line R / M HNSCC pipeline
Key trends include a shift toward chemotherapy-free combinations alongside PD-1 blockade:
With bispecific antibodies (10.8%), ADCs (10.8%), and cancer vaccines (9.0%) representing the most common novel modalities
Eight key phase 3 trials are underway:
All incorporating PD-1 as a target, with pembrolizumab as the backbone in 7 of 8
Overall, ASCO 2026 highlights a transformative period in head and neck oncology:
With perioperative immunotherapy now established as a new standard, bispecific antibodies and ADCs showing compelling early efficacy, and biomarker-driven strategies (PD-L1 CPS, HPV status, ctHPV-DNA, MRD) increasingly guiding treatment selection
References
Neoadjuvant and Adjuvant Pembrolizumab in Locally Advanced Head and Neck Cancer. Uppaluri R, Haddad RI, Tao Y, et al. The New England Journal of Medicine. 2025;393(1):37-50. doi:10.1056/NEJMoa2415434.
FDA approves neoadjuvant and adjuvant pembrolizumab for resectable locally advanced head and neck squamous cell carcinoma | FDA. Food and Drug Administration. 2025-06-13.
Neoadjuvant and adjuvant pembrolizumab (pembro) plus standard of care (SOC) for resectable locally advanced head and neck squamous cell carcinoma (LA HNSCC): Efficacy by surgical outcomes in the phase 3 KEYNOTE-689 trial.. Adkins D, Haddad R, Tao Y, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):6057. doi:10.1200/JCO.2026.44.16_suppl.6057.
Perioperative or adjuvant PD-1/PD-L1 blockade with curative-intent multimodality therapy for locally advanced head and neck squamous cell carcinoma: A systematic review and meta-analysis of randomized trials.. Daher S, Daher H, Altal H, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):e18074. doi:10.1200/JCO.2026.44.16_suppl.e18074.
Neoadjuvant ivonescimab (AK112, a PD-1/VEGF bispecific antibody) combined with nab-paclitaxel and cisplatin (AP) for resectable locally advanced head and neck squamous cell carcinoma (LA-HNSCC): An exploratory phase II study.. Kunyu Yang, Xiaomeng Zhang and Lu Wen. Journal of Clinical Oncology. 2026;44(Suppl 16):6014. doi:10.1200/JCO.2026.44.16_suppl.6014.
Neoadjuvant immunotherapy in combination with chemotherapy in resectable locally advanced head and neck squamous cell carcinoma: Updated efficacy and safety data from a randomized phase II trial.. Liu L, Chen F, Li Y, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):6091. doi:10.1200/JCO.2026.44.16_suppl.6091.
Neoadjuvant adebrelimab plus chemotherapy in untreated locally advanced head and neck squamous cell carcinoma: Efficacy and biomarker insights from a single-arm phase 2 trial.. Fang R, Lei W, Huang B, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):6106. doi:10.1200/JCO.2026.44.16_suppl.6106.
Ficerafusp Alfa (BCA101) With Pembrolizumab for Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma: Two-Year Results of an Expansion Cohort of a Phase I/Ib Trial. Hanna GJ, Zandberg DP, Wong DJ, et al. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2026;:JCO2502027. doi:10.1200/JCO-25-02027.
A multicenter, randomized, double-blind, phase 2/3 study of ficerafusp alfa (BCA101) or placebo in combination with pembrolizumab for first-line treatment of HPV-negative, PD-L1–positive, recurrent or metastatic (R/M) head and neck squamous cell carcinoma (HNSCC): FORTIFI-HN01.. Ferrarotto R, Kaczmar J, Spigel D, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):TPS6129. doi:10.1200/JCO.2026.44.16_suppl.TPS6129.
Petosemtamab (MCLA-158) with pembrolizumab as first-line (1L) treatment of PD-L1+ recurrent/metastatic (r/m) head and neck squamous cell carcinoma (HNSCC): Phase 2 trial. Herpen C, Daste A, Arrazubi V, et al. Journal of Clinical Oncology. 2025;43(Suppl 16):6024. doi:10.1200/JCO.2025.43.16_suppl.6024.
LiGeR-HN Phase III Trials of Petosemtamab + Pembrolizumab and Petosemtamab Monotherapy in Recurrent or Metastatic HNSCC. Machiels JP, Fayette J, Haddad R, et al. Future Oncology (London, England). 2025;21(16):2007-2016. doi:10.1080/14796694.2025.2511470.
A phase 1/2 study of the next-generation nectin-4–targeting antibody-drug conjugate CRB-701 (SYS6002) in patients with recurrent or metastatic head and neck squamous cell carcinoma.. Mantia C, Hanna G, Loriot Y, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):6062. doi:10.1200/JCO.2026.44.16_suppl.6062.
A randomized, non-comparative, multicenter phase II trial of neoadjuvant becotatug vedotin alone or combined with immune checkpoint inhibitors (penpulimab/ivonescimab) in resectable locally advanced head and neck squamous cell carcinoma.. Wei X, Xiang Z, Zeng Y, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):TPS6135. doi:10.1200/JCO.2026.44.16_suppl.TPS6135.
Neoadjuvant HPV16-specific viral immunotherapy (HB200) plus chemotherapy with response-adapted de-escalation in HPV16+ oropharyngeal squamous cell carcinoma: TARGET-HPV trial.. Rosenberg A, Juloori A, Cursio J, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):6097. doi:10.1200/JCO.2026.44.16_suppl.6097.
Emerging trends in research strategies in the first-line recurrent or metastatic head and neck cancer (R/M SCCHN) landscape: A top-level analysis by Oncofocus.. Shukla A, Keeshara V, Chamaria M, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):e18029. doi:10.1200/JCO.2026.44.16_suppl.e18029.
Recent Highlights and Breakthroughs in Immunotherapy for Head and Neck Cancers. Vuille JA, Szturz P. Current Opinion in Oncology. 2026;38(3):201-211. doi:10.1097/CCO.0000000000001211.
Immunotherapy in Locally Advanced Head and Neck Squamous Cell Carcinoma: The Current Status and Future Outlook. Köylü B, Selçukbiricik F, Aksoy S, Güven DC. Critical Reviews in Oncology/Hematology. 2026;:105145. doi:10.1016/j.critrevonc.2026.105145.
Avoids all the disadvantages of a lateral mandibulotomy and the sequelae of a midline mandibulotomy
A paramedian mandibulotomy offers significant advantages:
Wide exposure to the surgical field
Preservation of the geniohyoid and genioglossus muscles:
Leading to preservation of:
The hyomandibular complex
The only muscle requiring division is the mylohyoid muscle:
Which leads to minimal swallowing difficulties
A paramedian mandibulotomy does not cause denervation or devascularization of the skin of the chin or the teeth and mandible
Fixation at the mandibulotomy site is easy
The site of the mandibulotomy does not fall within the lateral portal of radiation therapy if the patient needs postoperative radiotherapy:
Thus at present a paramedian mandibulotomy remains an optimal surgical approach for access to posteriorly located larger lesions of the oral cavity and tumors of the oropharynx and parapharyngeal space