- Thyroid nodules are a major health problem worldwide:
- The prevalence of palpable thyroid nodules in the general population is:
- Approximately 5% in women and 1% in men living in parts of the world with sufficient iodine
- In contrast, high resolution neck and thyroid ultrasound can detect thyroid nodules in:
- Approximately 19% to 68% of randomly selected people, with higher frequencies in women and the elderly
- The prevalence of palpable thyroid nodules in the general population is:
- The clinical importance of thyroid nodules lies in the need to rule out thyroid cancer:
- Which occurs anywhere between 7% and 15% of cases:
- Varying according to gender, age, history of exposure to radiation, family history, among other factors
- Which occurs anywhere between 7% and 15% of cases:
- The detection and diagnosis of differentiated thyroid cancer have evolved over the years with increased use of:
- High resolution cervical and thyroid ultrasound
- Fine needle aspiration biopsy (FNAB)
- Molecular testing
- Thyroglobulin as a serum tumor marker
- Definition of Thryoid Nodules:
- A thyroid nodule is defined as a discrete lesion within the thyroid gland that is radiologically different from the surrounding thyroid parenchyma:
- Certain palpable lesions may not resemble a distinct radiologic abnormality:
- Such abnormalities do not meet the stringent definition for a thyroid nodule
- Certain palpable lesions may not resemble a distinct radiologic abnormality:
- Non-palpable nodules detected on ultrasound or by other imaging studies are termed incidentally discovered nodules or “incidentalomas”:
- Non-palpable nodules have the same risk of malignancy as do ultrasonographically confirmed palpable nodules of the same size
- Usually, only nodules greater than 1 cm in size should be evaluated since they have a greater potential to be clinically significant cancers:
- Sporadically, there may be thyroid nodules less than 1 cm that require further evaluation because of clinical symptoms or associated lymphadenopathy:
- In very rare instances, some nodules less than 1 cm lack these ultrasonographic and clinical warning signs yet may nonetheless cause future morbidity and mortality
- Sporadically, there may be thyroid nodules less than 1 cm that require further evaluation because of clinical symptoms or associated lymphadenopathy:
- A thyroid nodule is defined as a discrete lesion within the thyroid gland that is radiologically different from the surrounding thyroid parenchyma:
- Initial Assessment of Thyroid Nodules:
- Upon discovery of a thyroid nodule, a complete clinical history and a physical examination centered on the thyroid gland and adjacent regional lymph nodes should be performed
- Relevant historical factors that predict malignancy in a thyroid nodule include:
- A history of childhood radiation therapy to the head and neck region
- Total body radiation for bone marrow transplant
- Exposure to ionizing radiation in childhood or adolescence
- Familial thyroid carcinoma
- Hereditary thyroid cancer syndrome:
- Cowden syndrome
- Familial polypoid adenomatosis
- Carney complex
- Werner syndrome
- Multiple endocrine neoplasia 2A
- Multiple endocrine neoplasia 2B
- A rapidly growing thyroid nodule and / or hoarseness
- Relevant physical findings suggesting possible malignancy include:
- Vocal cord paralysis
- Cervical lymphadenopathy
- Fixation of the thyroid nodule to surrounding tissues
- With the discovery of a thyroid nodule greater than 1 cm in any diameter:
- A serum thyroid stimulating hormone level (TSH) should be obtained (recommendation # 2 of the American Thyroid Association [ATA]):
- If the TSH is low:
- A thyroid scan should be performed (this is the only indication nowadays to perform this study) to document whether the thyroid nodule is hyperfunctioning (“hot”, tracer uptake is greater than the adjacent normal thyroid), iso-functioning (“warm”, tracer uptake is equal to the surrounding normal thyroid), or non-functioning (“cold”, tracer uptake is less than the adjacent normal thyroid tissue)
- Since hyperfunctioning thyroid nodules rarely contain malignancy, if one is found that corresponds to the nodule in question:
- A cytological evaluation is not necessary
- If there is obvious or subclinical hyperthyroidism:
- An additional evaluation with a thyroid scan is required
- High serum levels of TSH:
- Even within high normal range, are associated with an increased risk of malignancy in the thyroid nodule, as well as a more advanced stage of the thyroid cancer
- If the TSH is low:
- Thyroglobulin (Tg) has a very high specificity for thyroid tissue and has led to its evaluation as a disease marker for more than 30 years:
- Serum Tg concentrations were found to be increased in a range of thyroid disorders, most prominently in advanced thyroid carcinoma:
- Nevertheless, considerable overlap was found between levels observed in benign thyroid disorders and those observed in tumor patients
- Furthermore, many patients with relatively small thyroid carcinomas had serum Tg concentrations that fell within the range of values found in healthy individuals
- Based on this evidence during the initial evaluation of thyroid nodules, it is not recommended to routinely obtain serum Tg (recommendation 3 of the ATA)
- As mentioned previously serum levels of Tg may be elevated in the vast majority of thyroid diseases (benign and malignant) and it is an insensitive and nonspecific test for the diagnosis of thyroid cancer
- Even when the diagnosis of thyroid cancer is established standard preoperative measurement of serum Tg or anti-Tg antibodies is not recommended by the ATA (recommendation # 34)
- Evidence from a systematic review and meta-analysis indicated that elevated preoperative levels of serum Tg may foresee a higher sensitivity for postoperative surveillance with serum Tg
- Serum Tg concentrations were found to be increased in a range of thyroid disorders, most prominently in advanced thyroid carcinoma:
- Anti-Tg antibodies obtained in the preoperative period do not appear to be an independent preoperative prognosticator of stage in patients with differentiated thyroid cancer (DTC), but the evidence is limited:
- Evidence from the National Thyroid Cancer Treatment Cooperative Study (a large thyroid cancer registry that enrolled patients between 1987 and 2011), serum anti-Tg antibody status was not significantly associated with stage of disease on multivariate analysis, or with disease-free or overall survival on univariate or multivariate analyses
- Data that preoperative measurement of serum Tg impacts patient management or outcomes is not yet available
- A serum thyroid stimulating hormone level (TSH) should be obtained (recommendation # 2 of the American Thyroid Association [ATA]):
- The usefulness of serum calcitonin in the initial assessment of thyroid nodules has been evaluated in non-randomized prospective studies, with mixed results:
- Therefore, the ATA cannot recommend either for or against the routine measurement of serum calcitonin in patients with thyroid nodules (recommendation 4 of the ATA)
- A high-resolution ultrasound of the neck and thyroid should be performed in all patients with suspected thyroid nodules, nodular goiter, or any radiographic abnormality that suggests a thyroid nodule detected incidentally in another imaging study (computed tomography or magnetic resonance imaging, or 18 FDG-PET) (recommendation 6 of the ATA):
- The neck and thyroid ultrasound should evaluate the following characteristics:
- The thyroid parenchyma:
- Homogeneous or heterogeneous
- The size of the thyroid gland
- The size, location, and ultrasonographic features of any thyroid nodule
- The presence or absence of suspicious cervical lymph nodes in the central or lateral compartments of the neck
- The thyroid parenchyma:
- The characteristics that should be evaluated on ultrasound are:
- Node size (in three dimensions)
- The location (example—right upper lobe / if it is anterior or posterior)
- Description of the ultrasonographic characteristics of the thyroid nodule:
- Composition of the nodule:
- Solid, cystic or spongiform
- Echogenicity:
- Isoechoic, hyperechoic, hypoechoic
- Margins:
- Regular
- Irregular:
- Defined as infiltrative, microlobulated or speculated
- Presence and type of calcifications:
- Macro or microcalcifications
- Shape:
- If the nodule is taller than wider
- Vascularity:
- Central or peripheral
- Composition of the nodule:
- The neck and thyroid ultrasound should evaluate the following characteristics:

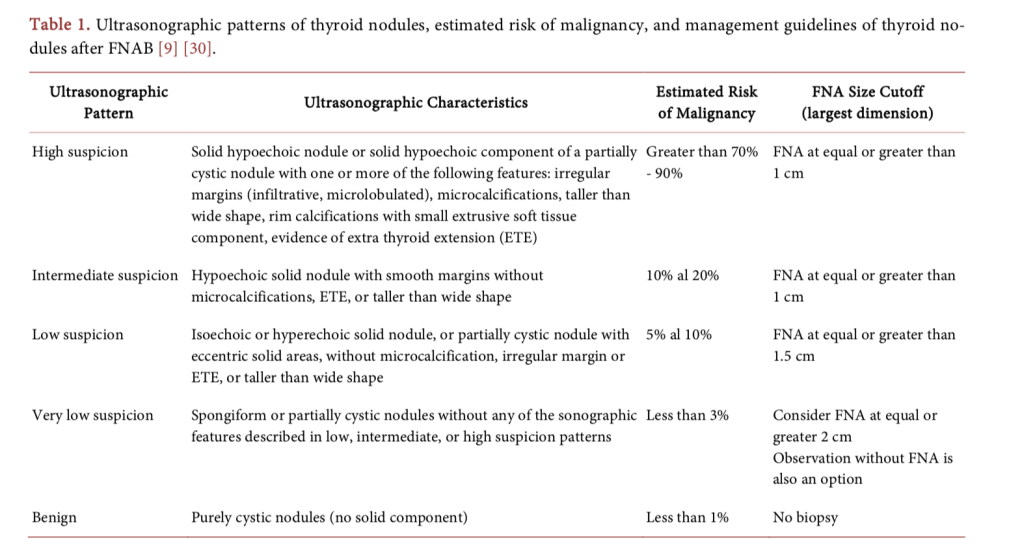
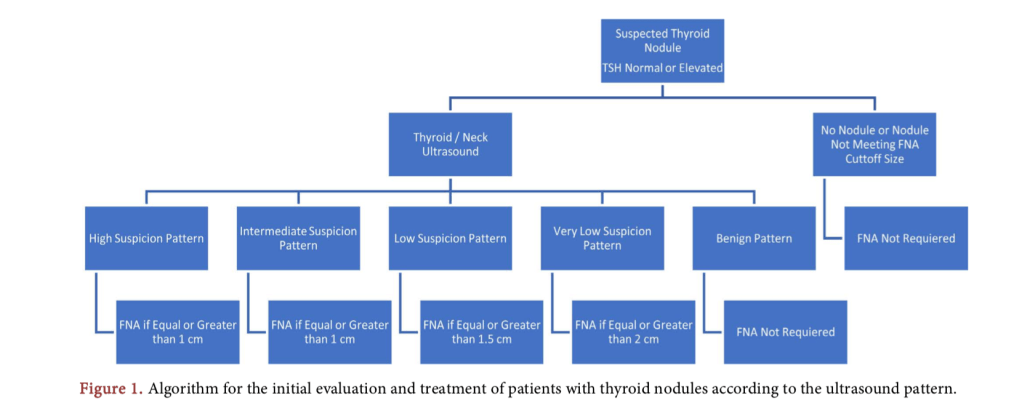
- The ultrasonographic pattern associated with a thyroid nodule confers a risk of malignancy, and combined with the size of the nodule, guides decision-making (Table 1).
- The ultrasonographic pattern of high suspicion of malignancy includes:
- Hypoechoic nodules, solid nodules, or nodules with mixed components (a solid and partially cystic hypoechoic nodule) with one or more of the following characteristics: irregular margins (infiltrative, microlobulated), microcalcifica- tions, shape than wider, peripheral calcifications on the cyst wall, evidence of extra thyroid extension
- The ultrasonographic pattern of high suspicion of malignancy includes:
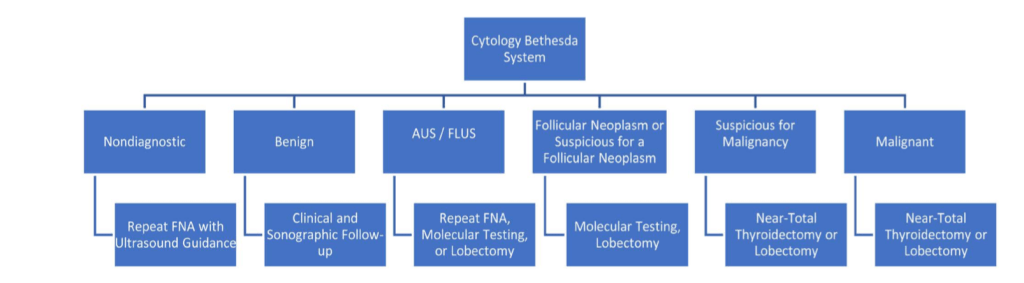
- Fine needle aspiration biopsy (FNAB) is the most accurate and cost-effective way de evaluate suspicious thyroid nodules (recommendation # 7 of the ATA):
- Thyroid nodules with a higher probability of obtaining a non-diagnostic cytology (cystic component greater than 25% to 50%) or a sampling error (nodules difficult to palpate or located in the posterior portion of the thyroid lobe):
- It is preferred to perform a FNAB ultrasound guided
- Thyroid nodules with a higher probability of obtaining a non-diagnostic cytology (cystic component greater than 25% to 50%) or a sampling error (nodules difficult to palpate or located in the posterior portion of the thyroid lobe):
- References:
- Arrangoiz, R., et al. (2018) Management Approach to Thyroid Nodules. Interna- tional Journal of Otolaryngology and Head & Neck Surgery, 7, 214-227. https://doi.org/10.4236/ijohns.2018.74023

