- TYPE I GLOSSECTOMY (MUCOSECTOMY):Definition:
-
- Incision of the mucosa in healthy tissue with appropriate safety margins (0.5 cm to 1.0 cm depending on whether or not the lesion is well defined):
- The mucosa and submucosa are included up to the intrinsic muscle fibers of the tongue
- The deep resection margin should include:
- A thin layer of the intrinsic muscles:Because of a possible invasion of the submucosa
- Incision of the mucosa in healthy tissue with appropriate safety margins (0.5 cm to 1.0 cm depending on whether or not the lesion is well defined):
- Generally:
- The wound is left to heal by secondary intention
- Although the defect may be:Partially closed primarilyOr covered with a skin graft
- Indication:Precancerous, superficial suspicious lesions, limited to the epithelium of the tongue without previous biopsy:
-
- The aim of surgery:
- Is to remove all the lesion with adequate margins up to the healthy tissue with both diagnostic and curative intent
- The aim of surgery:
-
-

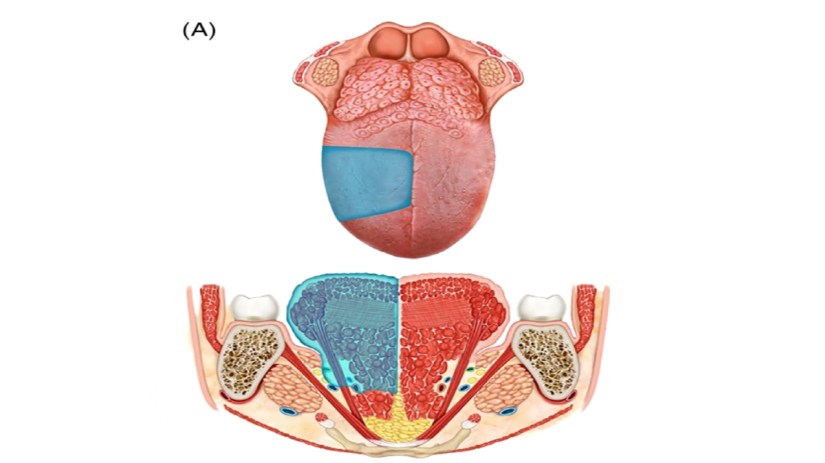
- TYPE II GLOSSECTOMY (PARTIAI GLOSSECTOMY):Definition: It includes the lesion and adjacent normal mucosa, submucosa, and the intrinsic muscles up to the surface of the extrinsic muscles (when the directions of the muscle fibers change)
-
- With appropriate safety margins (approximately 1.5 cm):The resection usually is diamond shaped on the surface, while more deeply, it is shaped like a truncated cone with the intrinsic muscles as the apex. The terminal branches of the lingual artery should be ligated
- The lingual nerve is usually preserved
- With appropriate safety margins (approximately 1.5 cm):The resection usually is diamond shaped on the surface, while more deeply, it is shaped like a truncated cone with the intrinsic muscles as the apex. The terminal branches of the lingual artery should be ligated
- Closure may be partial or total with the objective of avoiding:Bleeding, postoperative edema, and retracted scars
-
- Indication: Lesions infiltrating submucosa and superficially into intrinsic muscles, but not extrinsic muscles, or infiltration less than 10 mm deep

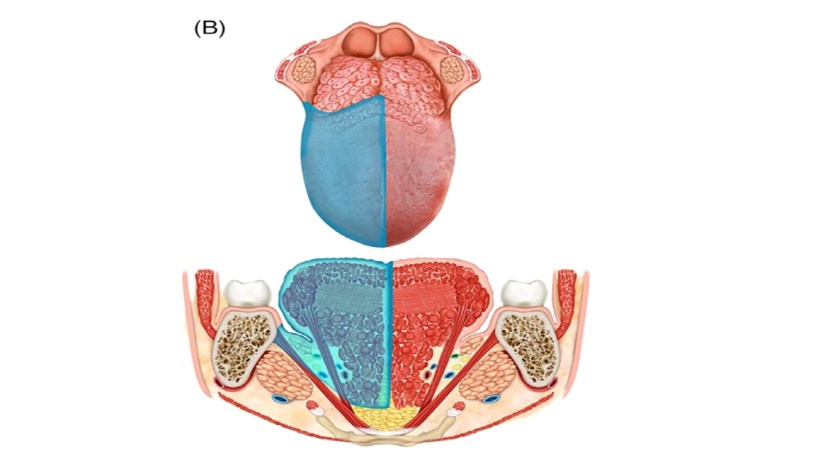
- TYPE III GLOSSECTOMY:Type IIIa glossectomy (hemiglossectomy):Definition: The specimen includes the mucosa, submucosa, and intrinsic and extrinsic muscles ipsilateral to the lesion:The mucosa is resected up to healthy tissue with appropriate safety margins (at least 1.5 cm)
-
-
-
- The lingual artery must be ligated and removed en bloc with the lingual and hypoglossal nerves, in the specimen of the primary tumor and neck nodes
- The base of the ipsilateral tongue is preserved
- The tip of the tongue can be preserved or not
-
- Indication: Lesions infiltrating the intrinsic and minimally extrinsic muscles or infiltration greater than 10 mm but confined within the ipsilateral tongue
-
- Type IIIb glossectomy (compartmental hemiglossectomy):Definition: The specimen includes the mucosa, submucosa, intrinsic and extrinsic muscles ipsilateral to the lesion, genioglossus, hyoglossus and styloglossus muscles, and the inferior portion of the palatoglossus muscle.
-
- Medially:The midline raphe is included in the resection
- The lingual nerve is resected as far cranially as possible
- The hypoglossal nerve is removed after the ansa
- The lingual artery and vein is ligated in proximity to the horn of the hyoid bone, and removed en bloc with specimen and neck nodes
- Indication: Lesions massively infiltrating the intrinsic and extrinsic muscles but confined to the ipsilateral tongue
-
-
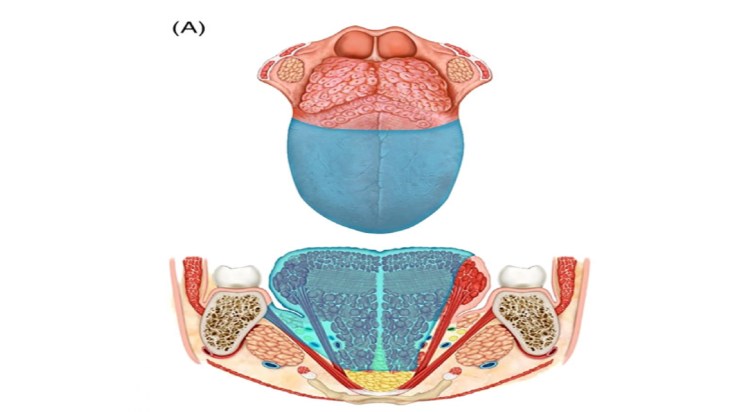
- TYPE IV GLOSSECTOMY:Type IVa glossectomy (subtotal glossectomy):Definition: This is an anterior subtotal glossectomy
-
-
- With preservation of both sides of the base of the tongue, posterior hyoglossus muscle, and hypoglossal and lingual nerves, from the less involved side.
- Indication:Lesions that arise in the anterior portion of the mobile tongue and exceed the hemilingual area of origin involving the contralateral genioglossus muscle but limited to mobile tongue
-
-
-
- Type IVb (near-total glossectomy):Definition: Type IVa glossectomy with extension to the ipsilateral base of the tongue:The following contralateral structures are preserved:Hyoglossus and styloglossus muscles, hypoglossal and lingual nerves, and lingual artery (functional unit of the base of the tongue)Indication: Massive lesions that exceed the border of the hemilingual area of origin infiltrating the ipsilateral base of the tongue and the contralateral genioglossus muscle

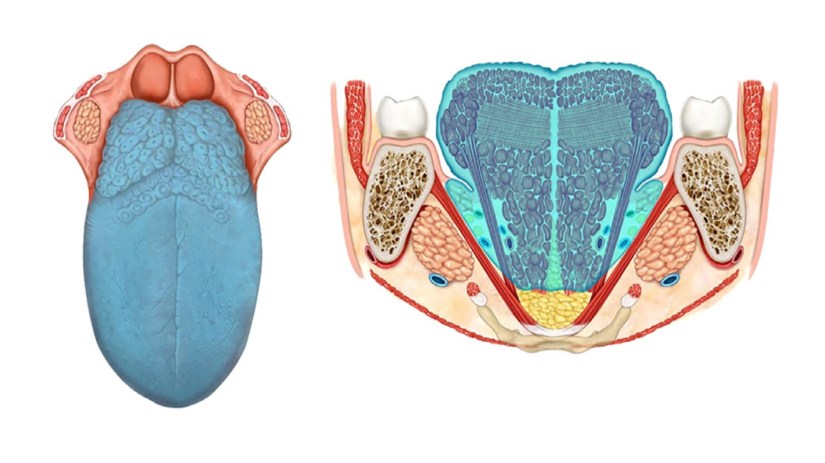
- TYPE V GLOSSECTOMY (TOTAL GLOSSECTOMY):Definition: The specimen includes all of the mobile tongue and the base of the tongue transected at the level of the lingual arteries, hypoglossal, lingual nerves, and the floor of the mouth.Indication:Massive infiltrating lesions, for instance, those of the anterior ventral surface of the tongue, dorsum of the tongue, or the tongue base, which bilaterally involve the extrinsic genioglossus, hyoglossus, and styloglossus with impairment of the mobility of the tongue

- What is Head and Neck Surgery?:
- It is a surgical sub-specialty that deals mainly with benign and malignant tumors of the head and neck region, including:
- The scalp, facial region, eyes, ears, nose, nasal fossae, paranasal sinuses, oral cavity, pharynx (nasopharynx, oropharynx, hypopharynx), larynx (supraglotic larynx, glottis larynx, subglotic larynx), thyroid gland, parathyroid gland, salivary glands (parotid glands, submandibular glands, sublingual glands, minor salivary glands), soft tissues of the neck, skin of the head and neck region.
- The head and neck surgeon’s work area:Does not cover tumors or diseases of the brain and other areas of the central nervous system or those of the cervical spine:This is the neurosurgeon field.
- The scalp, facial region, eyes, ears, nose, nasal fossae, paranasal sinuses, oral cavity, pharynx (nasopharynx, oropharynx, hypopharynx), larynx (supraglotic larynx, glottis larynx, subglotic larynx), thyroid gland, parathyroid gland, salivary glands (parotid glands, submandibular glands, sublingual glands, minor salivary glands), soft tissues of the neck, skin of the head and neck region.
- Among the diagnostic procedures performed by the head and neck surgeon, are the following:
- Nasopharyngolaryngoscopy:
- Performed to examine, evaluate and, possibly perform a biopsy, of oral cavity, pharyngeal and laryngeal lesions.
- Nasopharyngolaryngoscopy:
- The surgeries most commonly performed by the head and neck surgeon are:
- Total or near total thyroidectomies
- Hemithryoidectomies (lobectomies)
- Comprehensive neck dissections
- Selective neck dissections
- Maxillectomies:
- Total maxillectomy
- Subtotal maxillectomy
- Infrastructure maxillectomy
- Suprastructure maxillectomy
- Medial maxillectomy
- Mandibulectomy:
- Segmental
- Marginal
- Tracheostomy
- Salivary gland surgeries:
- Parotid gland operations:
- Limited superficial parotidectomy with identification and preservation of the facial nerve
- Superficial parotidectomy with identification and preservation of the facial nerve
- Near total parotidectomy with identification and preservation of the facial nerve
- Total parotidectomy
- Submandibular gland resection
- Sublingual gland resection
- Parotid gland operations:
- Resection of tumors of the oral cavity:
- Glossectomy
- Resection of the floor of the mouth tumors
- Resection of tumors of the pharynx
- Resection of tumors of the larynx
- Split-thickness skin grafts
- Full-thickness skin grafts
- Sentinel lymph node mapping and sentinel lymph node biopsy
- Resection of malignant skin tumors (BCC, SCC, melanoma) of the head and neck region
- It is a surgical sub-specialty that deals mainly with benign and malignant tumors of the head and neck region, including:
- The formation of the head and neck surgeon includes mastering the following subjects:
- Surgical Anatomy
- History and Basic Principles of Head and Neck Surgery
- Epidemiology, Etiology, and Pathology of Head and Neck Diseases
- Diagnostic Radiology of the Head and Neck Region
- Tumors of the Scalp, Skin and Melanoma
- Eyelids and Orbit
- Nasal Cavity and Paranasal Sinuses
- Skull Base and Temporal Bone
- Lips and Oral Cavity
- Pharynx and Esophagus
- Larynx and Trachea
- Cervical Lymph Nodes
- Thyroid and Parathyroid Glands
- Salivary Glands
- Neurogenic Tumors and Paragangliomas
- Soft Tissue Tumors
- Bone Tumors and Odontogenic Lesions
- Reconstructive Surgery
- Oncologic Dentistry and Maxillofacial Prosthetics
- Principles of Radiation Oncology
- Principles of Chemotherapy
- Molecular Oncology, Genomics and Immunology
- Nutrition
- Biostatistic
Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon / endocrine surgeon / surgical oncologist and is a member of Center for Advanced Surgical Oncology at Palmetto General Hospital:

Training:
• General surgery:
• Michigan State University:
• 2004 al 2010

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016

#Arrangoiz
#Teacher
#Surgeon
#Cirujano
#ThyroidExpert
#ThyroidSurgeon
#CirujanodeTiroides
#ExpertoenTiroides
#ExpertoenParatiroides
#Paratiroides
#Hiperparatiroidismo
#CancerdeTiroides
#ThyroidCancer
#PapillaryThyroidCancer
#SurgicalOncologist
#CirujanoOncologo
#CancerSurgeon
#CirujanodeCancer
#HeadandNeckSurgeon
#CirugiaEndocrina
#CirujanodeTumoresdeCabezayCuello
#OralCavityCancer
#CASO
#CenterforAdvancedSurgicalOncology
#PalmettoGeneralHospitalwww.centerforadvancedsurgicaloncology.com
