- In the year 2007 the National Cancer Institute Thyroid FNA State of the Science Conference presented consensus recommendations known as the Bethesda System for Reporting Thyroid Cytopathology:
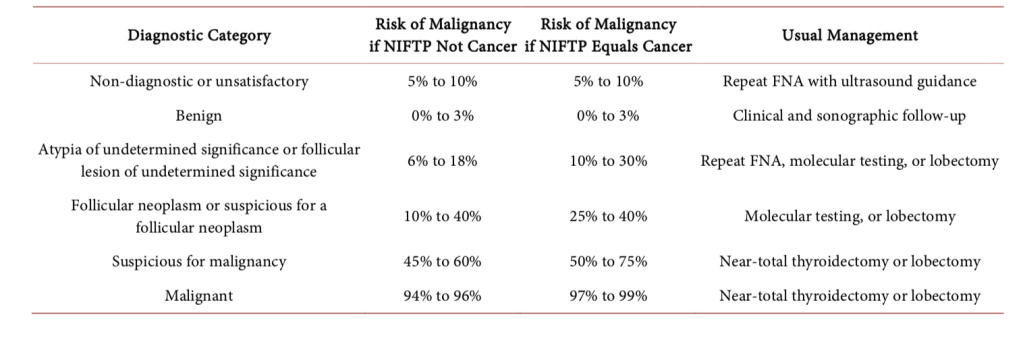
- The Bethesda system includes six diagnostic categories and offers an approximation of cancer risk within each category based upon literature review and expert opinion (Table)
- Current studies that utilized the criteria and terminology of the Bethesda system to a large series of patients have shown a good concordance in reporting FNA cytology:
- 89% to 95% of samples being satisfactory for interpretation:
- Benign:
- 55% to 74% of the cases
- Malignant:
- 2% to 5% of the cases
- Cytologically indeterminate (20% to 30% of the cases):
- Atypia of undetermined significance or follicular lesion of undetermined significance (AUS / FLUS):
- 2% to 18% of the thyroid nodules
- Follicular neoplasm or suspicious for follicular neoplasm (FN / SFN):
- 2% to 25% of the thyroid nodules
- Suspicious for malignancy:
- 1% to 6% of the thyroid nodules
- Atypia of undetermined significance or follicular lesion of undetermined significance (AUS / FLUS):
- Benign:
- 89% to 95% of samples being satisfactory for interpretation:
- The Bethesda system has proven highly beneficial, allowing physicinas to speak with the same terminology and better convey malignant risk
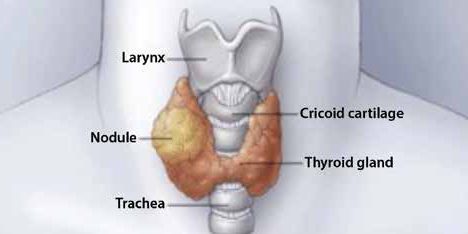
- Non-Diagnostic or Unsatisfactory FNA Results:
- Non-diagnostic or unsatisfactory FNAB are those that do not meet the established quantitative or qualitative requirements to say that the cytological assessment is adequate:
- The presence of at least six well-visualized groups of follicular cells, each group containing at least 10 well-preserved epithelial cells, preferably in a single slide
- When FNA is performed in a thyroid nodule and the initial cytology result is non-diagnostic:
- FNAB should be repeated with the support of ultrasound guidance, and if available, cytological assessment should be performed at the time of FNAB (recommendation # 10 of the ATA):
- It has been suggested that FNAB should be repeated no earlier than three months after initial FNAB to avoid a falsely positive interpretation due to reactive changes induced by the biopsy:
- Two recent studies have questioned the need for a three-month waiting period after the first FNAB because they found no correlation between the diagnostic/accuracy performance of the second FNAB and the waiting time between procedures
- It has been suggested that FNAB should be repeated no earlier than three months after initial FNAB to avoid a falsely positive interpretation due to reactive changes induced by the biopsy:
- Thyroid nodules that have undergone multiple FNABs that turned out to be non-diagnostic without having an ultrasonographic pattern of high suspicion:
- Can undergo a period of observation vs. surgical excision to have a definitive histopathological diagnosis (recommendation 10 of the ATA)
- Surgical excision should be considered for:
- Histopathologic diagnosis if the cytologically non-diagnostic nodule has a:
- High suspicion sonographic pattern
- Growth of the nodule:
- Greater than 20% in two dimensions
- Greater than 50% increase in the volumen of the nodule
- Is detected during US surveillance,
- Clinical risk factors for malignancy are present
- Histopathologic diagnosis if the cytologically non-diagnostic nodule has a:
- FNAB should be repeated with the support of ultrasound guidance, and if available, cytological assessment should be performed at the time of FNAB (recommendation # 10 of the ATA):
- In several published series of patients classified according to the Bethesda system:
- Non-diagnostic samples constituted 2% to 16% of all FNAB samples:
- Of which 7% to 26% were resected:
- The frequency of malignancy among all the FNAB initially classified as non-diagnostic was 2% to 4% and among the non-diagnostic samples that were finally resected the frequency of malignancy 9% to 32%
- Of which 7% to 26% were resected:
- Non-diagnostic samples constituted 2% to 16% of all FNAB samples:
- Non-diagnostic or unsatisfactory FNAB are those that do not meet the established quantitative or qualitative requirements to say that the cytological assessment is adequate:
- Benign Cytology:
- If the thyroid nodule turns out to be benign in cytology after FNAB, no addi- tional diagnostic or treatment studies are needed immediately (recommendation 11 of the ATA)
- Although prospective studies are lacking, the rates of malignancy in the retrospective series:
- Range from 1% to 2%
- Atypia of Undetermined Significance (AUS) or Follicular Lesion of Undetermined Significance (FLUS) on Cytology:
- Based on the Bethesda system, this diagnostic category is reserved for specimens that contain cells with:
- Architectural and / or nuclear atypia that are more prominent than expected for benign changes, but not sufficient to be placed in one of the highest-risk diagnostic categories
- In the studies that used the criteria established by the Bethesda system, the risk of cancer for patients with AUS / FLUS who underwent surgery was:
- 6% to 18% if NIFT (non-invasive follicular thyroid neoplasia with papillary nuclear characteristics) it is not considered cancer, and 10% to 30% if NIFT is considered a cancer
- For thyroid nodules with AUS / FLUS cytology after a FNAB, with clinical and ultrasonographic features of concern:
- The assessment can be continued by repeating the FNAB or if the technology is available, molecular tests can be used to complement the risk assessment of malignancy instead of preceding directly with a strategy of either surveillance or diagnostic surgery (lobectomy)
- Patient preference should be considered in decision-making (recommendation 15 of the ATA)
- If FNAB is not repeated, and molecular tests are not performed, or both studies were inconclusive:
- A diagnostic surgical excision may be performed for the thyroid nodules with Bethesda AUS / FLUS classification, according to the clinical risk factors, the ultrasonographic pattern, and patient preference (recommendation 15 of the ATA)
- Based on the Bethesda system, this diagnostic category is reserved for specimens that contain cells with:
- Folicular Neoplasm / Suspicious Folicular Neoplasm Cytology (FN / SFN):
- This diagnostic category of the Bethesda system is used for cellular aspirates:
- Composed by follicular cells arranged in an altered architectural pattern characterized by cell crowding and / or microfollicular formation, lacking nuclear characteristics of papillary carcinoma or
- Composed almost exclusively oncocytic cells (Hurthle)
- This is a category has an intermediate risk of malignancy in the Bethesda system, with an estimated risk of malignancy:
- Between 10% and 40% if NIFT is not considered cancer and between 25% to 40% if NIFT is considered cancer
- This category represents 1% to 25% (average, 10%) of all FNA samples
- Diagnostic surgical excision (lobectomy) is the long-established standard for the treatment of thyroid nodules with a FN / SFN cytology:
- However, if you have the technology, after taking into account the clinical assessment and the ultra- sonographic characteristics, molecular tests can be used to complement the assessment of the risk of malignancy instead of proceeding directly with surgery (recommendation 16) of the ATA)
- Patient preference should be considered in clinical decision making
- If the molecular tests cannot be performed or are indeterminate:
- Surgical excision can be considered for the definitive diagnosis of thyroid nodules classified as FN / SFN (recommendation 16 of the ATA)
- This diagnostic category of the Bethesda system is used for cellular aspirates:
- Suspicious Cytology for Malignancy:
- This diagnostic category of the Bethesda system represents 1% to 6% of all FNABs and is reserved for aspirates with cytological features that generate a high suspicion of malignancy (mainly for papillary thyroid carcinoma) but that are not sufficient for a conclusive diagnosis
- This is the highest risk category for indeterminate cytology in the Bethesda System, with an estimated cancer risk of :
- 45% to 60% if NIFT is not considered cancer and 50% to 75% if NIFT is considered cancer:
- Due to the high risk of cancer, the diagnosis of suspicious papillary carcinoma is an indication for surgery
- 45% to 60% if NIFT is not considered cancer and 50% to 75% if NIFT is considered cancer:
- If FNAB results in a suspicious cytology for papillary thyroid carcinoma, the surgical treatment should be very similar to the management of a frankly malig- nant reported for the FNA:
- Factors that we must take into account in offering the definitive treatment with a suspicious cytology for papillary thyroid carcinoma, are the clinical risk factors, the ultrasonographic characteristics, the patient’s preference, and possibly the results of the molecular tests (BRAF, RAS, RET/PTC, PAX8/PPAR) (recommendation 17 of the ATA)
- Malignant Cytology:
- If the cytological result is diagnostic of primary thyroid malignancy, surgery is usually recommended (recommendation 12 of the ATA)
- A cytology diagnosis of primary thyroid malignancy will almost always lead to thyroid surgery
- However, in some parts of the world under research protocol active surveillance can be offered as an alternative to immediate surgery in certain patients who meet some very specific criteria:
- Patients with very low risk tumors (papillary microcarcinomas without clini- cally evident metastases or local invasion, and without convincing cytological evidence of aggressive disease)
- Patients with high surgical risk due to multiple comorbidities
- Patients with a relatively short lifespan (severe cardiopulmonary disease,other malignancies, very old age)
- Patients with concurrent medical or surgical problems that must be ad-dressed before thyroid surgery
