With HER2 negative breast cancer and residual disease after undergoing neoadjuvant chemotherapy to:
Standard postsurgical treatment and capecitabine or placebo
The primary end point was:
Disease-free survival (DFS)
Secondary end points included:
Overall survival (OS)
DFS was longer in the capecitabine group than in the control group:
74.1% vs. 67.6% of the patients were alive and free from recurrence or second cancer at 5 years
Among patients with triple-negative disease:
DFS was 69.8% in the capecitabine group versus 56.1% in the control group
The OS rate was 78.8% versus 70.3%
Residual disease after completion of neoadjuvant chemotherapy:
Is associated with worse outcomes
References:
Masuda N, Lee SJ, Ohtani S, Im YH, Lee ES, Yokota I, et al. Adjuvant capecitabine for breast cancer after preoperative chemotherapy. N Eng J Med. 2017;376(22):2147-2159.
Symmans WF, Wei C, Gould R, Yu X, Zhang Y, Liu M, et al. Long-term prognostic risk after neoadjuvant chemotherapy associated with residual cancer burden and breast cancer subtype. J Clin Oncol. 2017;35(10):1049-1060.
That provides prognostic and predictive information in hormone receptor positive breast cancer
The recurrence score based on the 21-gene assay ranges from:
0 to 100:
Is predictive of chemotherapy benefit:
When it is higher than 25
Both tamoxifen and aromatase inhibitors:
Have been shown to:
Reducerecurrence rates and improve survival in postmenopausal women
Although chemotherapy has been shown to be beneficial in many patient subsets:
The 21-gene recurrence score was developed:
To help ascertain which patients with:
ER-positive, node-negative breast cancer:
Would be most likely to benefit from chemotherapy in addition to adjuvant tamoxifen
In patients with an intermediate recurrence score:
The benefit of chemotherapy is unclear
The Trial Assigning IndividuaLized Options for Treatment (Rx) [TAILORx] trial:
Is a randomized prospective trial:
That randomized women with ER-positive breast cancer:
With a score of 11 to 25 to:
Chemotherapy plus endocrine therapy to endocrine therapy alone
This trial is closed to accrual, and the results of this trial for this cohort are pending:
However:
Outcomes data from a subset of 1626 patients with a recurrence score of less than 10:
Were recently published
These patients were assigned to:
Receive endocrine therapy alone without chemotherapy
This study reported a 5-year local recurrence rate of:
0.5% in women with a recurrence score of:
Less than 10
Furthermore:
At 5 years:
The invasive disease–free survival was:
93.8%
The rate of freedom from recurrence of breast cancer at a distant site was:
99.3%
At distant or local site was:
98.7%
Overall survival rate of:
98%
The authors concluded that a favorable gene expression profile:
Is associated with a very low rate of recurrence:
At 5 years with endocrine therapy alone
References:
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), Dowsett M, Forbes JF, et al. Aromatase inhibitors versus tamoxifen in early breast cancer: patient-level meta-analysis of the randomised trials. Lancet. 2015;386(10001):1341-1352.
Sparano JA, Gray RJ, Makower DF, et al. Prospective validation of a 21-gene expression assay in breast cancer. N Engl J Med. 2015;373(21):2005-2014.
Sparano JA et al, N Engl J Med 2018 Sparano JA, Gray RJ, Makower DF, Pritchard KI, Albain KS, Hayes DF, et al. Adjuvant chemotherapy guided by a 21-gene expression assay in breast cancer. N Engl J Med 2018;379(2):111-121.
Paik S, Tang G, Shak S, Kim C, Baker J, Kim W, et al. Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor-positive breast cancer. J Clin Oncol; 2006;24(23):3726-3734.
👉Three important conclusions are agreed upon regarding this clinical entity:
– Prognosis of occult primary breast cancer is the same or slightly better than women with classic stage IIA disease (T0, N1, M0)
– An exhaustive workup for the non-breast primary is usually not fruitful
– Treatment of the breast in some manner decreases the risk of local failure over time.
👉Modified radical mastectomy has been the traditional surgical treatment for many years.
👉Previously, the primary breast cancer was found in the mastectomy specimen 40% to 80% of the time, but with the advent of much better mammography and ultrasound along with breast MRI, this rate is much lower now.
👉However, what was true then and still holds today is that no treatment to the breast itself results in an unacceptably high local recurrence rate.
👉An alternative to a modified radical mastectomy is complete ALND followed by whole-breast irradiation.
👉Axillary dissection provides local control while also fine tuning staging.
👉Theoretically the whole-breast radiation should control any subclinical disease in the breast not detected on imaging.
👉Primary radiation to the breast, axilla, and supraclavicular area without any surgery of the breast or axilla results in higher local and regional recurrence compared to surgery and radiation combined.
👉Axillary node dissection and whole-breast irradiation has been found to have equivalent survival as a modified radical mastectomy.
👉A recent meta-analysis of seven studies and more than 240 patients with occult primary breast cancers (0.3% to 0.8% of all breast cancers). found 39% were treated with ALND and radiation while 47% had modified radical mastectomy and 15% had ALND alone.
👉With a mean follow-up of 5 years, the study found no difference in local regional recurrence (12.7 vs 9.8 %), distant metastasis (7.2 vs 12.7 %), or mortality (9.5 vs 17.9 %) between ALND and radiation vs modified radical mastectomy (all p>0.16).
👉ALND with radiation was superior to ALND alone in terms of local regional recurrence (12.7 vs 34.3 %, p < 0.01) and trended towards improved survival but this was not statistically significant (P=0.09).
REFERENCES
Barton SR, Smith IE, Kirby AM, Ashley S, Walsh G, Parton M. The role of ipsilateral breast radiotherapy in management of occult primary breast cancer presenting as axillary lymphadenopathy.Eur J Cancer. 2011;47:2099-2106. PMID: 21658935.http://www.ncbi.nlm.nih.gov/pubmed/21658935
Macedo FI, Eid JJ, Flynn J, Jacobs MJ, Mittal VK. Optimal surgical management for occult breast carcinoma: a meta-analysis.Ann Surg Oncol. 2016;23:1838-1844.https://www.ncbi.nlm.nih.gov/pubmed/26832884
Rueth NM, Black DM, Limmer AR, et al. Breast conservation in the setting of contemporary multimodality treatment provides excellent outcomes for patients with occult primary breast cancer.Ann Surg Oncol. 2015;22:90-95. [epub ahead of print].http://www.ncbi.nlm.nih.gov/pubmed/25249256
Walker GV, Smith GL, Perkins GH, et al. Population-based analysis of occult primary breast cancer with axillary lymph node metastasis.Cancer. 2010;116:4000-4006. PMID: 20564117.http://www.ncbi.nlm.nih.gov/pubmed/20564117
Woo SM, Son BH, Lee JW, et al. Survival outcomes of different treatment methods for the ipsilateral breast of occult breast cancer patients with axillary lymph node metastasis: a single center experience.J Breast Cancer. 2013;16:410-416.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3893343/
👉Rodrigo Arrangoiz MS, MD, FACS miembro de Sociedad Quirúrgica y cirujano oncólogo de mama.
👉The thyroid gland, located at the base of the neck, is shaped like a butterfly, and produces hormones that regulate heart rate, blood pressure, body temperature, and weight.
👉In thyroid cancer does not cause any symptoms most of the time in the initial stages, but as it grows it can cause:
A lump (nodule) that can be felt through the skin of the neck
Voice changes, including increasing hoarseness
Difficulty to swallow
Pain in the neck and throat
Swollen lymph nodes in the neck
👉Thyroid cancer is classified into different subtypes based on the types of cells found in the tumor:
Papillary thyroid cancer.
Follicular thyroid cancer.
Anaplastic thyroid cancer.
Medullary thyroid cancer.
Dr. Rodrigo Arrangóiz from Center for Advanced Surgical Oncology, is an expert in the treatment of this disease
👉The number of new thyroid cancer cases has increased over recent years, especially the number of small, low-risk papillary thyroid cancers.
👉It is clear now that treating these small cancers aggressively with surgery results in more potential harm to patients than if the small cancer was simply watched.
👉Because of this, simply watching, known as active surveillance, became a promising alternative to surgery for these low-risk cancers in select patients.
👉Active surveillance involves closely monitoring the thyroid cancer over time, instead of treating it with immediate surgery.
👉Prior studies have shown that active surveillance is safe in papillary thyroid cancers measuring 1 cm or smaller and confined to the thyroid without any lymph node involvement or spread outside of the neck.
👉However, little is known about outcomes of active surveillance for patients with larger cancers measuring 1 to 2 cm and confined to the thyroid.
👉This study compared outcomes of active surveillance for these patients to this with cancers less than 1 cm.
👉The authors also examined outcomes of patients who had surgery for these small cancers.
👉THE FULL ARTICLE TITLE: Sakai T et al 2019 Active surveillance for T1bN0M0 papillary thyroid carcinoma. Thyroid 29:59–63. Epub 2019 Jan 8. PMID: 30560718.
👉The study included patients who were followed at the Cancer Institute Hospital in Tokyo, Japan, since 1995.
👉Among 406 patients with papillary thyroid cancer less than 1 cm, 360 (89%) underwent active surveillance and 46 (11%) underwent surgery.
👉Among 392 patients with papillary thyroid cancer 1 to 2 cm, 331 (84%) underwent active surveillance and 61 (16%) underwent surgery.
👉The patients in the active surveillance program were followed with physical exam, neck ultrasound and chest X-rays every 6 to 12 months after diagnosis.
👉These patients were evaluated for increase in cancer size, development of spread to the lymph nodes and spread to other parts of the body.
👉The follow-up was 7.3 – 7.9 years.
👉If progression of the cancer was seen or the patient changed their mind, surgery was performed.
👉The authors found that the 5- and 10-year rates of progression were similar in patients with papillary thyroid cancer less than 1 cm compared with those with 1 cm to 2 cm cancers during active surveillance.
👉A total of 11 patients with 1 to 2 cm cancers had surgery after active surveillance and none had the cancer come back.
👉Of the patients with 1 to 2 cm cancers who had immediate surgery, 8 had the cancer come back.
👉The rate of cancer coming back was significantly higher for cancers ≥ 1.5 cm than < 1.5 cm in this group.
👉WHAT ARE THE IMPLICATIONS OF THIS STUDY? 1. This study showed that patients with 1 to 2 cm papillary thyroid cancers had similar progression rates to patients with less than 1 cm cancers during active surveillance. 2. Additionally, delayed surgery was not associated with any harm in these patients. 3. These findings are important as they show that active surveillance of small thyroid cancers, especially those less than 15 mm in size, is safe. 4. Expanding active surveillance to larger cancers would decrease the number of thyroid surgeries and subsequent complications. However, more research is still needed to determine exactly which thyroid cancer patients are ideal for active surveillance, considering age, other health issues and the expertise of treatment team.
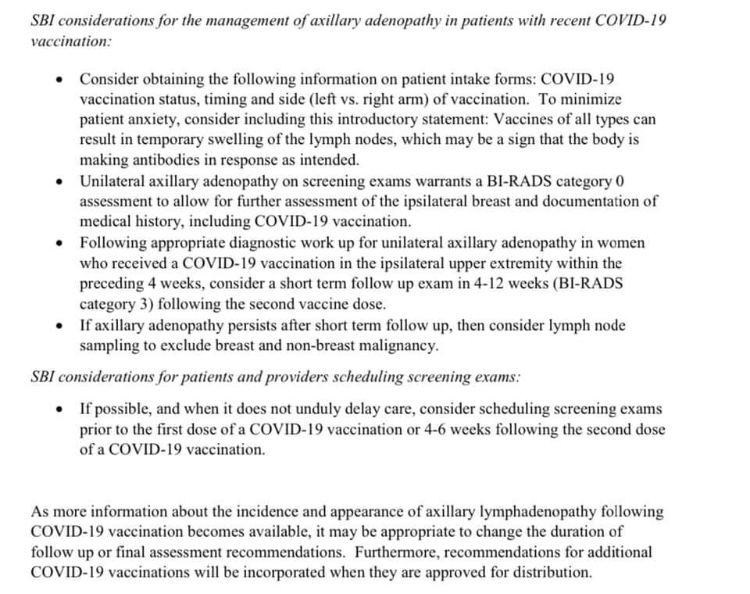
Society of Breast Imaging recently recently guidelines on management of unilateral axillary adenopathy in patients who have recently received Covid vaccine. Also, here’s a newly published paper on this topic we are encountering commonly in clinical practice.
👉The first guidelines ever released for screening mammography for older survivors of breast cancer (>75 years) recommend that routine mammography be discontinued for women whose life expectancy is less than 5 years but that screening continue for those whose life expectancy is more than 10 years.
👉For women who have a life expectancy of 5 to 10 years, the guidelines recommend that consideration be given to discontinuing mammography.
👉Overall, the guidelines encourage shared decision making that is individualized for each woman after weighing the benefits and harms associated with surveillance mammography and patient preferences.
👉The panel also recommended that patients with clinical findings and symptoms receive ongoing clinical breast examinations and diagnostic mammography and that patients be reassured that these practices will continue.
👉Guidelines on breast cancer screening for healthy women already “acknowledge the limitations of mammograms and the need to consider one’s health status and preferences when making decisions on how and when to stop routine mammograms.
The current study validates the clinical performance of Thyroseq v3 at 10 institutions.
Compared to the prior 56-gene version (Thyroseq v2), the expanded 112-gene ThyroSeq v3 showed improved sensitivity (94%, vs. 90–91% for Thyroseq v2) at the expense of a decrease in specificity (82%, vs. 91–93% for ThyroSeq v2) (2-4).
Thyroseq v2 had a very high benign call rate, allowing many patients with cytologically indeterminate thyroid nodules to avoid surgery.
The risk of cancer in nodules with a negative Thyroseq v3 result (false-negative rate) was 3%, which is comparable to the false-negative rate of a benign FNA cytology result.