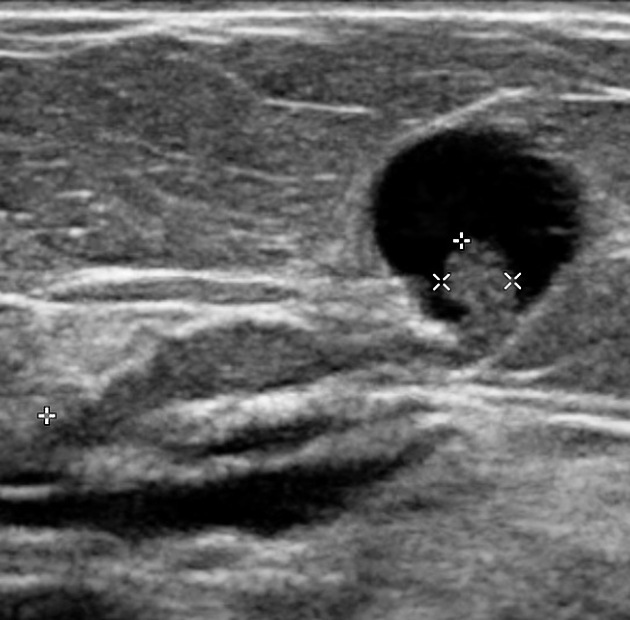
Large thyroid nodules in asymptomatic patients show malignancy and false-negative rates on fine needle aspiration (FNA) that are similar to those of small nodules, suggesting that nodule size alone should not be a reason for surgical resection, according to findings from a new meta-analysis.
-
- “Based on these data, surgical resection of large cytologically benign nodules is not recommended in the absence of other clinical indications,” for thyroidectomy, say Nicole A. Cipriani, MD, assistant professor of pathology, University of Chicago, Illinois, and coauthors of the study, recently published in Thyroid.
With conflicting data on whether larger nodule size is associated with a greater risk of malignancy and false-negative FNA rates, some surgeons choose to err on the side of caution and resect larger thyroid nodules, regardless of FNA results.
But the issue is controversial. Surgery itself is associated with potential risks, including increased physical and psychological morbidity, as well as a heavier financial burden, compared with the alternative approach of close clinical follow-up of cytologically benign nodules.
To assess the existing evidence, Cipriani and a team of multiple reviewers analyzed findings from 35 studies that stratified thyroid nodules by size and included data on benign and other cytology.
-
-
- The analysis included more than 20,000 nodules, of which more than 7000 had benign cytology.
-
-
- Of 21 datasets that allowed for comparison of malignancy rates by thyroid nodule size:
-
-
-
-
- 81% showed malignancy rates of larger nodules to be similar to or lower than rates of smaller nodules:
-
-
-
-
-
-
- The overall malignancy rate of large nodules (3 cm or greater) was 13.1% compared with 19.6% among nodules 3 cm or smaller (odds ratio [OR], 0.72).
-
-
-
-
-
-
- And in studies stratifying nodules as 4 cm or greater, the malignancy rate was similar, at 20.9%, to that of nodules 4 cm or smaller, at 19.9% (OR, 0.85).
False-negative FNA rates according to nodule size were available in 17 datasets, with only one study linking higher false-negative rates with larger nodules.
-
-
- In those studies, the overall false-negative rate of nodules 3 cm or greater was 7.2% compared with 5.7% of those smaller than 3 cm (OR, 1.47; CI, 0.80 – 2.69).
-
-
- And the overall false-negative rate of nodules 4 cm or greater was only slightly higher than that of nodules smaller than 4 cm, at 6.7% vs 4.5% (OR, 1.38; CI, 1.06 – 1.80), which was again not statistically significant.
-
- Although some studies have attempted to correlate larger thyroid nodule size with the risk of malignancy or false-negative FNA, the overall inconsistency of evidence is reflected in the American Thyroid Association (ATA) guidelines, which state that:
-
-
-
- “Based on the evidence, it is still unclear if patients with thyroid nodules 4 cm or larger and benign cytology carry a higher risk of malignancy and should be managed differently than those with smaller nodules.”
- It is surprising that multiple authors still recommend surgical resection of large cytologically benign nodules due to the perceived (but not actual) high false-negative rates:
-
-
- Based on the data provided by Cipriani et al I have (Rodrigo Arrangoiz) stopped recommending thyroidectomy for large cytologically being nodules based on size alone.
-
-
-
-
-
-
- The study by Cipriani et al showed no significant differences in the rate of malignancies between nodules smaller than 4 cm (140 of 546; 26.5%) compared with those 4 cm or larger (33 of 106; 31.1%).
-
-
-
-
-
-
- It also indicated that most malignancies among indeterminate thyroid nodules were low-risk regardless of tumor size, with the researchers concluding size should not be driving more aggressive diagnostic surgeries for cytologically indeterminate thyroid nodules.
ATA guidelines recommend resection primarily for nodules assessed on FNA to be malignant:
-
-
- But there are some exceptions for cytologically benign nodules, including those that are symptomatic, growing in size, of cosmetic concern, or substernal, with symptoms of concern including difficulty swallowing or breathing, or tracheal deviation.
-
-
-
-
-
- Close follow-up (including repeat ultrasound and/or FNA) can identify patients who ultimately require resection, and those with indolent disease may avoid surgery for cytologically benign but large thyroid
Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon / endocrine surgery specialist member of Sociedad Quirúrgica S.C at the America British Cowdray Medical Center in Mexico City:
-
-
-
-
-
-
-
He is an expert in the management of thyroid cancer:
-
-
-
-
-
-
-
If you have any questions about indications for surgery for thyroid nodules Dr. Arrangoiz:
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016

http://www.cirugiatiroides.com

























 • Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina:
• Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina: • Maestria en ciencias (Clinical research for healthprofessionals):
• Maestria en ciencias (Clinical research for healthprofessionals): • Cirugia de tumores de cabeza y cuello / cirugiaendocrina
• Cirugia de tumores de cabeza y cuello / cirugiaendocrina
