Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon / surgical oncologist and is a member of Sociedad Quirúrgica S.C at the America British CowdrayMedical Center in Mexico City:
-
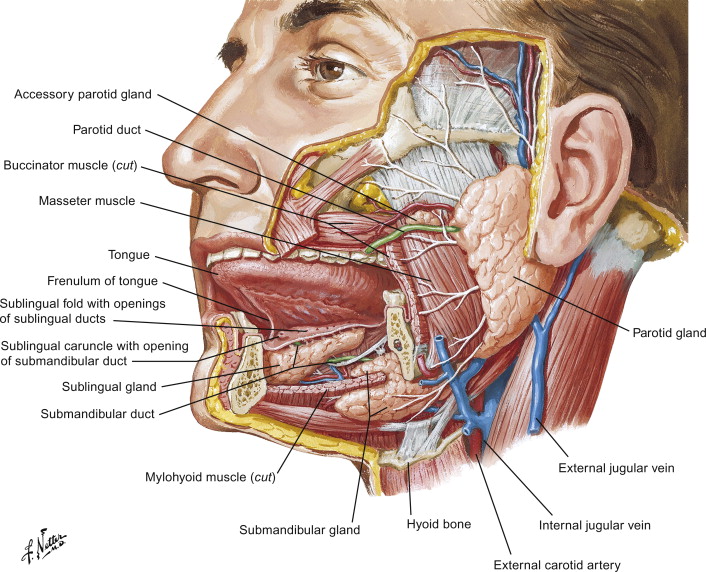
He is an expert in the management of salivary gland neoplasms:
-
If you have any questions about salivary gland neoplasms please fill free to ask Dr. Arrangoiz
Training:
• General surgery:
• Michigan State University:
• 2005 al 2010

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016

#Arrangoiz
#HeadandNeckSurgeon
#SurgicalOncologist
#Surgeon
#CancerSurgeon
#CirujanodeCabezayCuello
#CirujanoOncologo
http://www.sociedadquirurgica.com