Will be found to be associated with an adjacent malignant lesion:
The risk may be higher with abnormal mammogram findings
There is no indication for annual breast magnetic resonance screening in a patient with a radial scar
As a radial scar does not confer an increased risk of developing breast cancer:
Chemoprevention with tamoxifen is not indicated
References:
Linda A, Zuiani C, Furlan A, Londero V, Girometti R, Machin P, et al. Radial scars without atypia diagnosed at imaging-guided needle biopsy: how often is associated malignancy found at subsequent surgical excision, and do mammography and sonography predict which lesions are malignant? AJR Am J Roentgenol. 2010;194(4):1146-1151.
Hayes BD, O’Doherty A, Quinn CM. Correlation of needle core biopsy with excision histology in screen-detected B3 lesions: the Merrion Breast Screening Unit experience. J Clin Pathol. 2009;62(12):1136-1140.
Kennedy M, Masterson AV, Kerin M, Flanagan F. Pathology and clinical relevance of radial scars: a review. J Clin Pathol. 2003;56(10):721-724.
Patterson JA, Scott M, Anderson N, Kirk SJ. Radial scar, complex sclerosing lesion and risk of breast cancer. Analysis of 175 cases in Northern Ireland. Eur J Surg Oncol. 2004;30(10):1065-1068.
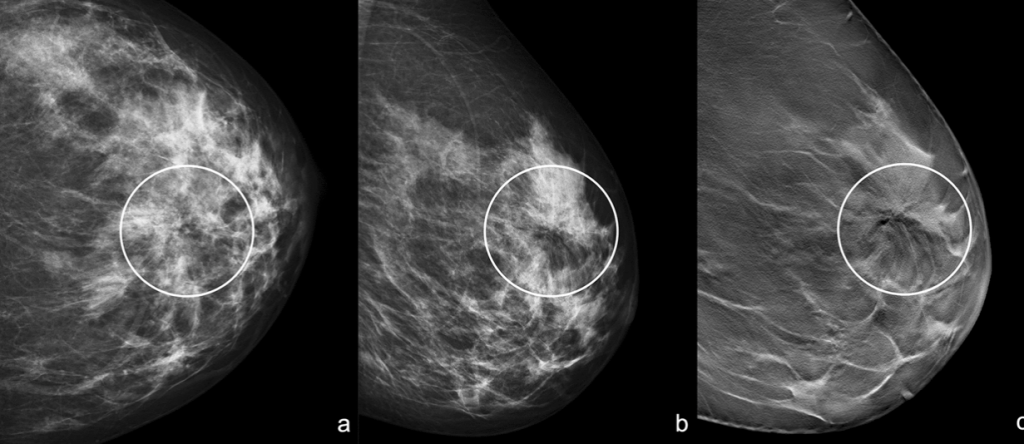
“Black Star”: Left craniocaudal (a) and mediolateral oblique (b) mammograms show an area of architectural distortion with radiolucent core in the union of upper quadrants (white circle). Left mediolateral oblique tomosynthesis (c) confirms the area of architectural distortion and shows better the radiolucent core with the radiating long thin spicules (white circle)
Anatomical triangle for the identification of the recurrent laryngeal nerve (RLN):
Often disclosed under other eponyms:
The triangular “area” as it is known today:
Was initially described by Frank H. Lahey:
Although the author (in his seminal article of 1938) does not refer to a triangle, he achieves an accurate description of the anatomical landmarks that have persisted over time
Lahey’s “Area” (1938):
Superior border:
Inferior thyroid artery
Medial border:
Trachea
Lateral border:
Common carotid artery
Content:
Recurrent laryngeal nerve
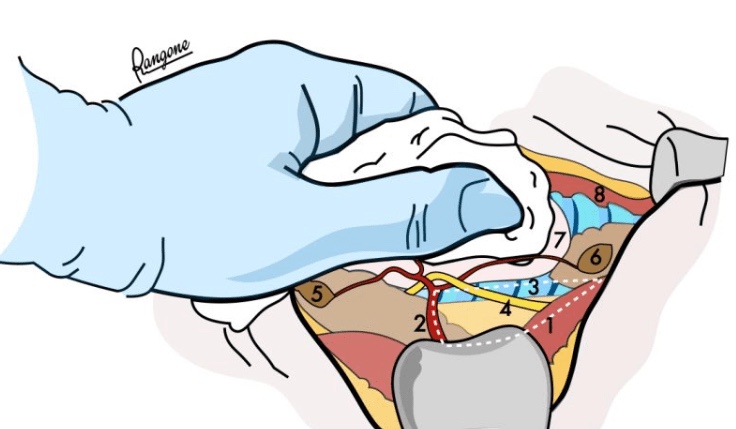
Image: “right paratracheal gutter”:
Common carotid artery (right)
Inferior thyroid artery
Trachea
Recurrent laryngeal nerve
Superior parathyroid gland
Inferior parathyroid gland
Thyroid lobe
Common carotid artery (left)
Triangle by Max M. Simon (1943):
Superior border:
Inferior thyroid artery
Medial border:
Recurrent laryngeal nerve
Lateral border:
Common carotid artery
Triangle by John M. Loré (1977?):
Superior border:
Inferior pole of the lateral lobe of the thyroid gland (retracted superiorly)
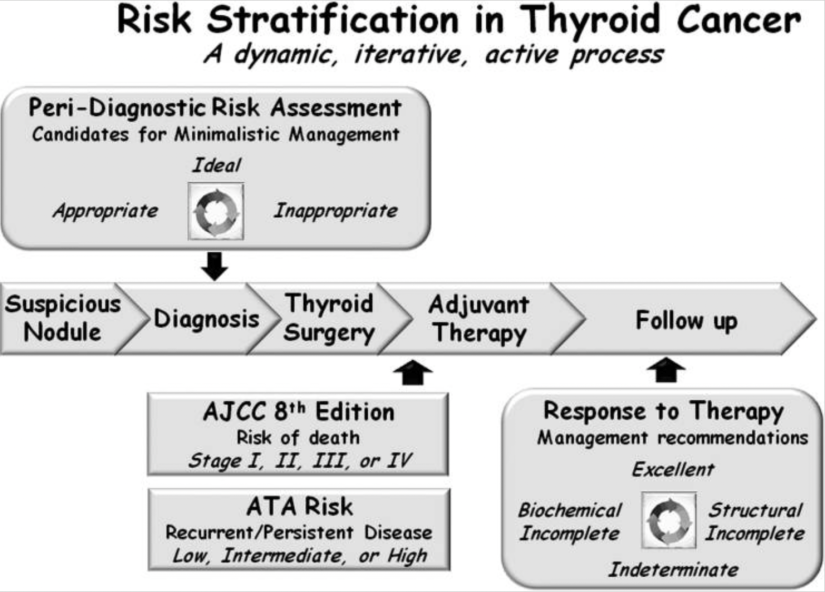
Although both the AJCC / TNM staging system and the ATA risk-stratification system provide valuable information with regard to initial risk stratification:
They are both static risk assessments that can only incorporate information available in the peri-diagnostic, preoperative, intraoperative, and early postoperative periods:
However, all of the static staging systems published provide suboptimal long-term predictions for individual patients:
As demonstrated by the proportion of variance explained, ranging from 20% to 30% across a wide range of studies (a measure of how well a predictive model correlates with the final outcome of interest)
However, when these initial risk estimates:
Are refined and modified over time as a response to therapy and as a reflection of the underlying biology of a particular patient’s thyroid cancer:
Risk estimates become more reliable and can achieve a proportion of variance explained as high as 70% to 80%
Over the last decade, several groups have developed and validated the general concept of dynamic risk stratification in which the baseline initial risk estimates are continually modified over time as new data become available:
Initially, dynamic risk stratification was validated only in the setting of total thyroidectomy and radioactive iodine and only in response to initial therapy
Over the last several years, it has become readily apparent that the concept of dynamic risk stratification should not be restricted to response to initial therapy:
But should rather be used to reclassify each patient when they return for their follow-up visits
Furthermore, definitions for response to therapy outcomes have been published and validated for patients receiving total thyroidectomy without radioactive iodine and even for low-risk patients treated with lobectomy alone
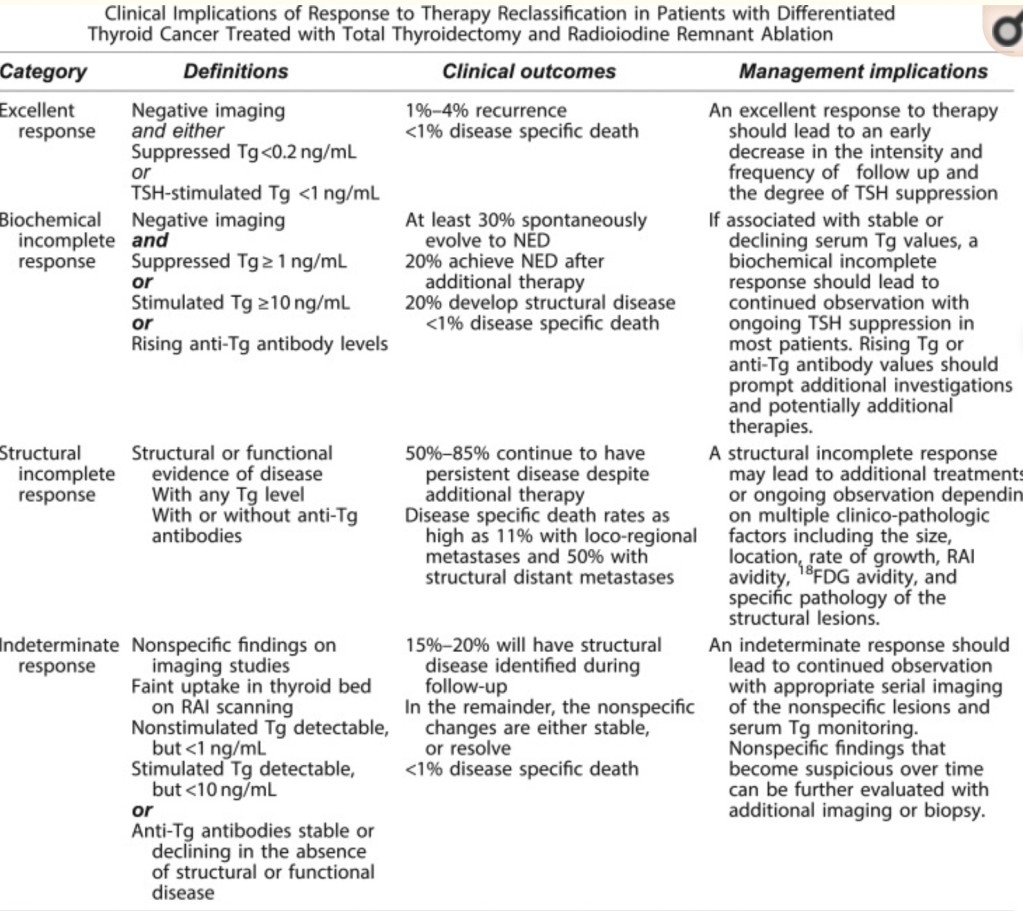
In patients treated with total thyroidectomy and radioactive iodine, the ATA guidelines provided a set of definitions, clinical outcomes, and management implications for the use of dynamic risk stratification:
In this paradigm, at each follow-up visit, the patient is classified as having an:
Excellent, biochemically incomplete, structurally incomplete, or indeterminate response to therapy Unlike the AJCC/TNM staging and the ATA risk-stratification systems, the response-to-therapy category can change over time as new data become available at each visit
Patients who have an excellent response to therapy:
Are expected to have essentially a normal overall survival and a very low risk of disease recurrence and therefore may not require intensive follow-up
Patients with biochemical incomplete response:
Have an abnormal Tg value but no structurally identifiable disease:
Are usually followed with observation unless the Tg or Tg antibodies are rising:
In which case additional imaging and evaluations are warranted to try to identify the source of the abnormal Tg
The indeterminate response category:
Initially described as acceptable response:
Was designed to be a temporary holding area for patients with nonspecific findings that could not be confidently described as benign or malignant
Over time, roughly 15% to 20% of these patients:
Will develop structural disease that may require additional therapy
In the remainder, the nonspecific changes are either stable or resolve:
Many of these patients can be reclassified as having an excellent response over time
Whereas patients with rising anti-Tg antibodies are classified as having a:
Biochemical incomplete response
Patients with stable or declining anti-Tg antibodies are categorized as having an:
Indeterminate response to therapy
Although Tg assays that use a liquid chromotography-tandem mass spectroscopy (LC-MS/MS) methodology:
Can identify some Tg antibody-positive patients as having detectable Tg in the setting of known structural disease:
Up to 20% to 40% of patients with structural disease will have undetectable Tg measurements on LC-MS/MS
Thus, in the setting of antithyroglobulin antibodies, an undetectable Tg obtained on the current LC-MS/MS assays is insufficient evidence to classify a patient as having an excellent response
Patients with a structural incomplete response:
Are particularly challenging in that the majority of them:
Will continue to have persistent disease despite additional therapies:
In this is the category of patients from which nearly all of the disease-specific mortality arises
These patients are likely to need additional imaging, ongoing thyroid-stimulating hormone suppression, and additional therapies over time
Now accept a minimalistic surgical approach (thyroid lobectomy without neck dissection):
To treat intra-thyroidal papillary thyroid carcinomasless than 4 cm in properly selected patients
Careful peri-diagnosis, preoperative, and intra-operative risk stratification:
Are the keys to successful use of thyroid lobectomywithout having to perform an unacceptable rate of early-completion thyroidectomies
Patients classified as being ideal for lobectomy would have:
Papillary micro-carcinomas:
That appeared to be confined to the thyroid:
In the setting of an otherwise normal thyroid ultrasound and clinical N0 neck
Patients are classified as appropriate for lobectomy if:
The tumor is 1 to 4 cm in maximum dimension:
If the contralateral lobe is normal, or if there are other abnormalities on the ultrasound, such as thyroiditis or benign-appearing nodules (again, in the setting of the clinical N0 neck)
Patients with extra-thyroidal extension, clinical N1 disease, or distant metastasis:
Would be considered inappropriate for thyroid lobectomy as initial therapy
In addition to the relevance of peri-diagnostic and preoperative risk stratification with respect to the selection of thyroid lobectomy as initial therapy:
It is important to recognize that there are intra-operative findings:
That should alter that recommendation and lead to an immediate total thyroidectomy
However, even with appropriate preoperative and intra-operative risk stratification:
As many as 6% to 20% of patients:
Will have unexpected findings on the final pathology report:
That may lead to a completion thyroidectomy and usually, radioactive iodine
An additional 5% to 10% may require completion thyroidectomy at some later point during follow-up for diagnostic or therapeutic purposes
The rate of early-completion thyroidectomy:
Performed following review of the initial pathology report, will vary:
Depending on how aggressive each management team is with regard to the use of radioactive iodine:
For either remnant ablation or adjuvant treatment
If minor factors, such as minor extrathyroidal extension, very small-volume lymph node metastasis, or small tumors with aggressive histologic features:
Usually lead to radioactive iodine therapy,:
Then the completion thyroidectomy rate may be as high as 20%
The most common reason for completion thyroidectomy:
Is unanticipated, extensive vascular invasion:
Documented on the pathology report that obviously could not be visualized preoperatively or intra-operatively
Thus, patients need to understand that the final determination of whether a thyroid lobectomy is the appropriate initial therapy:
Can only be achieved by the integration of preoperative, intra-operative, and postoperative risk stratification
Patients who are uncomfortable with this approach:
Will often choose a total thyroidectomy as initial therapy
Patients motivated to keep part of the thyroid will often accept that uncertainty:
Recognizing that the final decision regarding the completeness of initial therapy cannot be completely known until several weeks after the surgery is completed when more complete risk stratification can be accomplished
Unlike many cancers, the risk of recurrencedoes not parallel the risk of mortality in differentiated thyroid cancer
In most patients, the risk of recurrence far exceeds the risk of disease-specific mortality:
Thus staging systems designed to predict mortality in thyroid cancer:
Would not be anticipated to be predictive of disease recurrence
To address this issue, a risk-stratification system:
Was developed and validated to predict the risk of structural disease recurrence:
Based on information obtained around the time of initial therapy
A modified version of this original risk-stratification system was endorsed in the 2009 ATA guidelines and subsequently modified in the 2015 ATA guidelines
Whereas initially conceived as a three-category model of risk assessment:
Low, intermediate, or high risk
The ATA risk-stratification system:
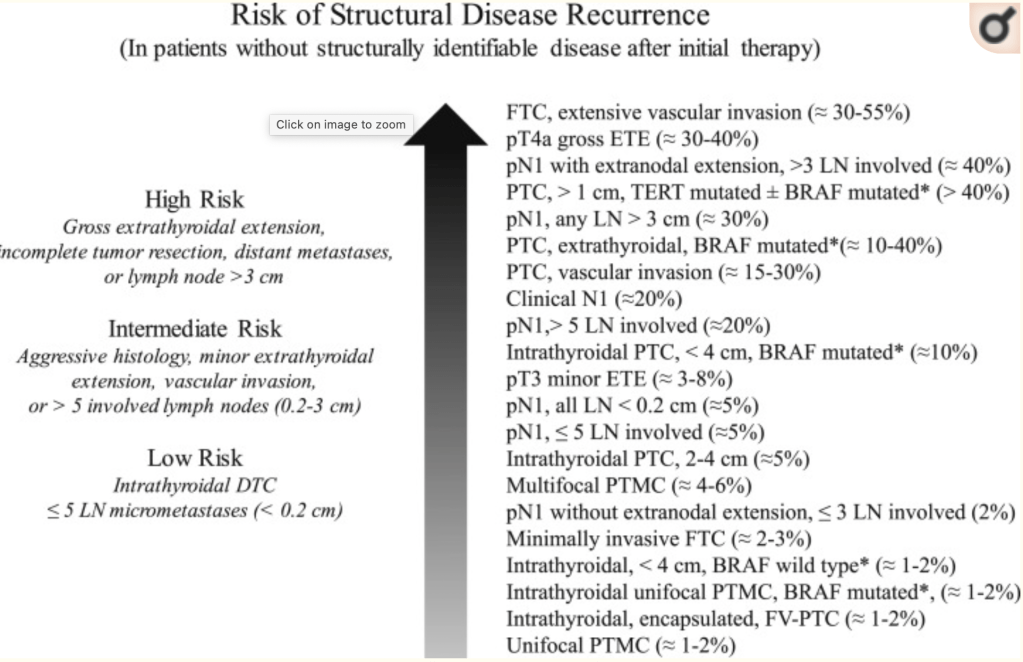
Is now visualized as a continuum of risk:
Ranging from very low to very high risk of structural disease recurrence
As described in the ATA guidelines, individualized risk stratification is best visualized as a “continuum of risk” rather than as three discrete risk categories that predict the risk of structural disease recurrence. [Adapted with permission from Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger M, Schuff KG, Sherman SI, Sosa JA, Steward DL, Tuttle RM, Wartofsky L. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26(1):1–133.]
The three-category model was proven to be very useful and reproducible across multiple studies
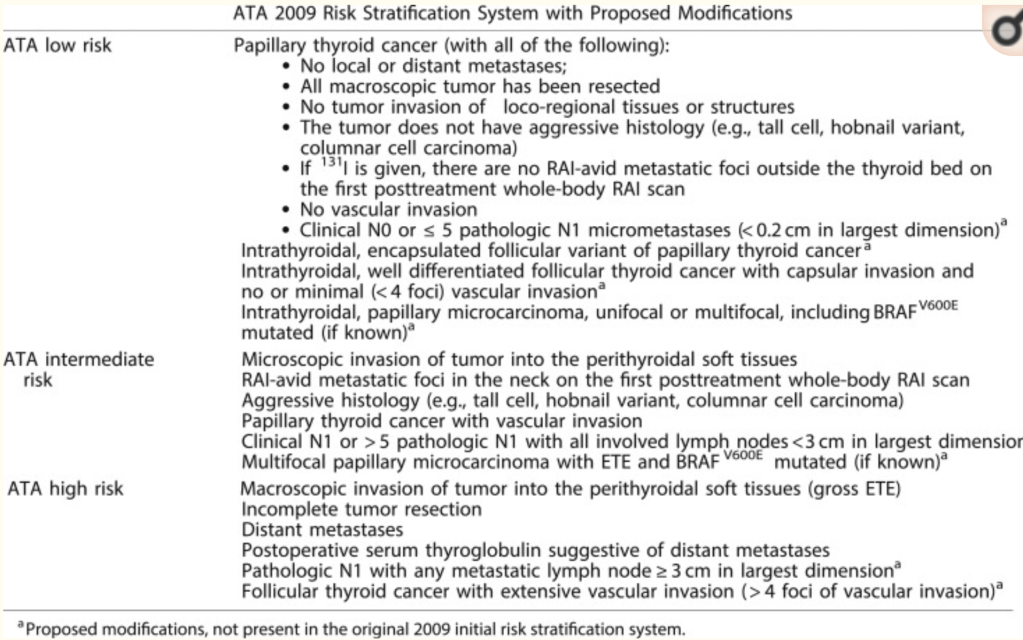
The 2015 ATA guideline:
Expanded the low-risk category to include not only intra-thyroidal papillary thyroid cancer but also patients with:
With capsular invasion and fewer than fourfoci of vascular invasion
Intra-thyroidal encapsulated follicular variant of papillary thyroid carcinoma:
Now known as noninvasive follicular thyroid neoplasm with papillary-like nuclear features
Either unifocal or multifocal intra-thyroidal papillary micro-carcinoma:
Even if they have known BRAFV600E mutations
The high-risk category was also expanded to include:
Follicular cancer with more than four foci of vascular invasion and
Pathologic lymph node metastasis:
With any metastatic lymph node ≥ 3 cm in largest dimension
The remaining tumors were classified as intermediate risk based on the data available at the time the guidelines were written
The 2015 ATA guidelines expanded the inclusion criteria for ATA low-risk and ATA high-risk disease categories as described in this table. [Adapted with permission from Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger M, Schuff KG, Sherman SI, Sosa JA, Steward DL, Tuttle RM, Wartofsky L. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26(1):1–133.]
The last several years have seen an abundance of published data confirming the association among specific molecular alterations,histological subtypes, and clinical outcomes in follicular cell-derived thyroid cancer
Point mutations in BRAFV600E:
Are associated with:
Increased risk of recurrence
Radioactive iodine refractoriness
Extrathyroidal extension
Lymph node metastases
Disease-specific mortality
Likewise, oncogenic genetic alterations in TERT promoter, TP53, EIF1AX, and β-catenin:
Are associated with more aggressive tumor behavior and poorer clinical outcomes
Furthermore, mutational combinations (such as BRAFV600E + TERT promoter mutations or RAS + TERT promoter mutations):
Are associated with significantly increased risk beyond that associated with either mutation in isolation
Appropriate molecular risk stratification requires integration of the genetic abnormality into the proper clinical context:
As the presence of a specific mutation does not always portend a poor prognosis:
e.g., BRAFV600E mutations are found in > 50% of papillary micro-carcinomas:
Which usually display an indolent clinical course
Although not yet proven:
It seems reasonable to consider either:
More careful follow-up or potentially more aggressive therapies for tumors with the highest risk mutational profiles:
Particularly those with mutational combinations associated with the poorest clinical outcome
It is important to remember that there is no guarantee that more aggressive surgery, radioactive iodine therapy, thyroid-stimulating hormone suppression, or other systemic therapies:
Will necessarily provide therapeutic benefit simply because we can identify a patient at high risk for poorer outcomes on the basis of clinic-pathological presentation or molecular profiling
Prospective studies evaluating the impact of more aggressive surgical and systemic therapies in the setting of high-risk mutational profiles are needed
The ATA risk-stratification system performs well in clinical practice:
With low-risk patients:
Demonstrating no evidence of disease 80% to 90% of the time
Biochemical incomplete responses 15% of the time
Structural incomplete responses 3% to 5% of the time
Intermediate-risk patients achieve:
Excellent response ∼60% of the time
Have a biochemical incomplete response ∼15% to 20% of the time,
Structural incomplete response ∼20% of the time
High-risk patients achieve:
No evidence of disease status in less than 30% of the cases
Structural incomplete response 50% to 75% of the cases
Biochemical incomplete response 10% to 15% of the cases
The studies contributing to these approximations are extensively reviewed in the ATA guidelines
Interestingly:
Age is a major determinant of response to therapy:
In ATA high-risk patients:
The proportion of excellent responders was found to be significantly higher among younger patients (age < 55 years) than among older patients (age ≥ 55 years; 40.3% vs 27.5%, P = 0.02)
The proportion of structural incomplete responders was significantly larger among older patients than among younger patients (53% vs 33%, P = 0.002)
Moreover, ATA high-risk younger patients with a structural incomplete response to therapy had a significantly better DSS than older patients (74% vs 12%, respectively, P < 0.001)
In October 2016, the AJCC (www.cancerstaging.org) published the eighth edition of the AJCC / TNM cancer staging system:
Which replaced the seventh edition that had been used by clinicians, cancer registries, and researchers since 2009
On 1 January 2018, tumor registries officially began using the eighth edition for tumor staging
Whereas the staging tables for medullary thyroid cancer and anaplastic thyroid cancer showed only minimal changes:
The rules for the staging of well-differentiated thyroid cancer underwent substantial modifications:
These included the following:
An increase of the age cutoff:
From 45 years to 55 years of age at diagnosis
Removal of microscopic extra-thyroidal extension:
As a key component of the staging system
No longer mandating assignment of stage III to older patients with microscopic extra-thyroidal extension or lymph node metastases
Establishment of a new T3b category for tumors of any size:
That demonstrate gross extra-thyroidal extension involving only the surrounding strap muscles
The AJCC Differentiated Thyroid Cancer Committee:
Carefully considered the possibility of inclusion of molecular markers (specifically, BRAFV600Eand TERT promoter mutations) in the AJCC prognostic staging definitions:
Whereas both of these mutations, particularly when present together:
Have been shown to be predictors of poor clinical outcomes:
They appeared to add only marginal benefit to the traditional anatomic staging factors (this might change in the next staging system with new data coming out)
Thus, molecular characterization of differentiated thyroid cancers, although providing some prognostic information:
Were not powerful enough factors to merit upstaging tumors to prognostic stages above those mandated by TNM risk factors
Nonetheless, similar to the approach used in the ATA risk-stratification system:
Molecular results can be used to refine further and individualize risk within risk categories or stages
The three critical factors that determine the prognostic stage groups of the eighth edition AJCC / TNM cancer staging system include:
The age at diagnosis
The presence or absence of distant metastases
The presence or absence of gross extra-thyroidal extension
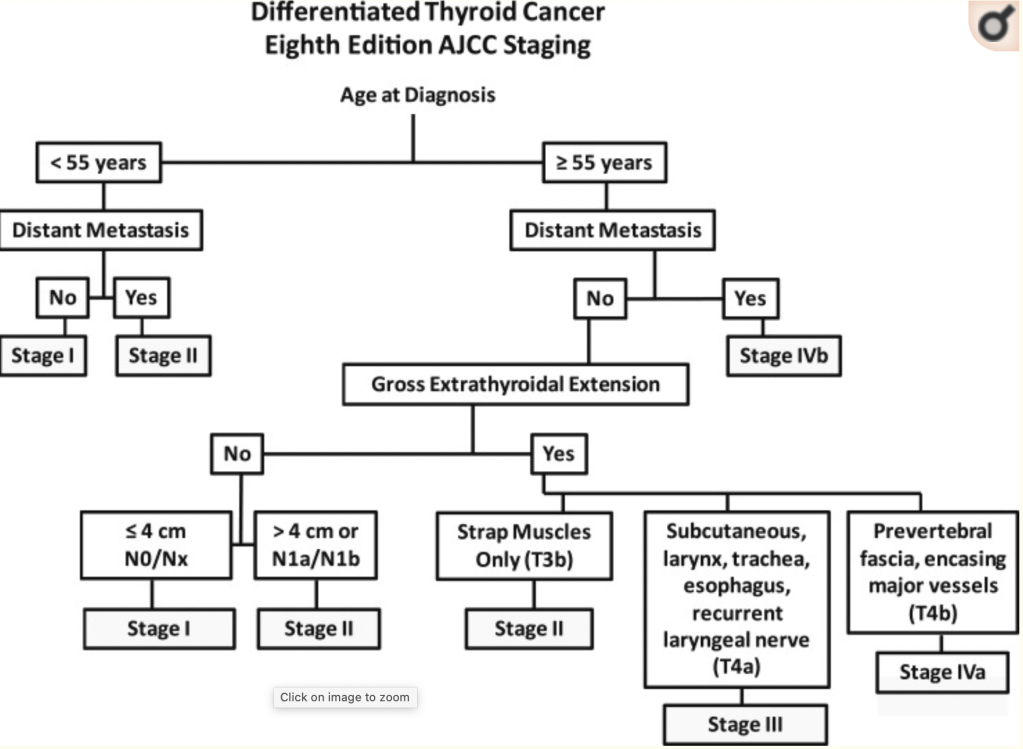
Rather than the use of the standard TNM staging tables provided in the AJCC / TNM manual, this flow diagram to stage patients rapidly based on the key clinical risk factors (age at diagnosis, distant metastasis, gross extrathyroidal extension, and lymph node metastases) may be easier
A simplified approach to AJCC staging in differentiated thyroid cancer, emphasizing the critical decision nodes, which include age at diagnosis, distant metastasis, and gross extrathyroidal extensions.
Patients age less than 55 years:
Rapidly classifies patients as either:
Stage I:
Any T, any N, M0 or
Stage II:
Any T, any N, M1
In the older patients, additional factors, such as:
The presence or absence of distant metastasis
Invasion of strap muscles
Extent of gross extra-thyroidal extension:
Are also used to define the prognostic stage groups
In the eighth edition of the AJCC / TNM cancer staging system:
It was anticipated that the majority of patients would be classified as stage I or stage II:
Reflecting the excellent outcomes expected in the majority of thyroid cancer patients
A smaller number of patients, particularly the older patients with either distant metastases or gross extra-thyroidal extension:
Were anticipated to do worse and are therefore classified as stage III or IV
Multiple publications have demonstrated that the eighth edition of the AJCC / TNM cancer staging system:
Moved a substantial number of patients into lower prognostic stage groups:
Without affecting the overall survival of those lower-stage groups
The patients who remained in the higher-stage groups:
Had poorer prognoses, as expected
This resulted in a much better separation of the four prognostic stage groups:
With respect to survival:
Such that 5- to 10-year disease-specific survival (DSS) was:
99% in stage I patients
88% to 97% in stage II patients
72% to 85% in stage III patients
67% to 72% in stage IV patients
Unlike previous editions of the AJCC / TNM staging system in which there was substantial overlap in survival in patients with stage I, II, and III disease:
The eighth edition provides meaningful separation among the prognostic stage groups that appear to be clinically relevant
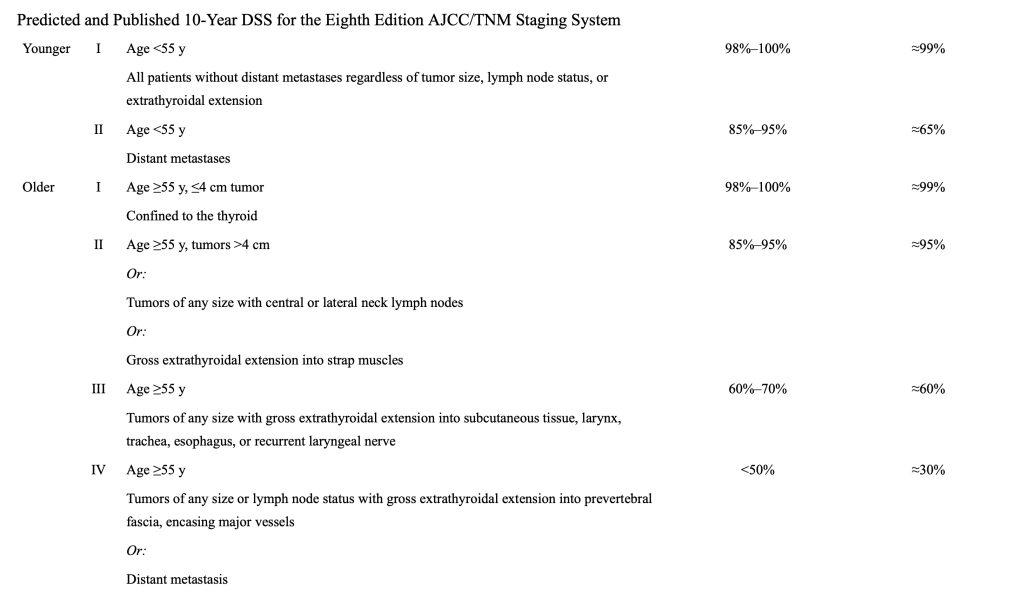
The differences in predicted and published ∼10-year survival rates:
Are best seen when analyzed based on age group (age <55 years vs age ≥55 years)
Ten-year median DSS estimates approximated from data extrapolated from publications examining eighth edition AJCC prognostic stages
The predicted 10-year DSS has been validated for all age and stage groups:
With only the younger (age < 55 years) stage II patients:
Appearing to do more poorly than anticipated
The lower-than-anticipated 10-year DSS in the younger patients (age < 55 years) with stage II disease:L
Was the result of the stage migration of patients in the 45- to 55-year age group:
From seventh edition AJCC stage IV to eighth edition AJCC stage II