- The 2015 ATA guidelines:
- Now accept a minimalistic surgical approach (thyroid lobectomy without neck dissection):
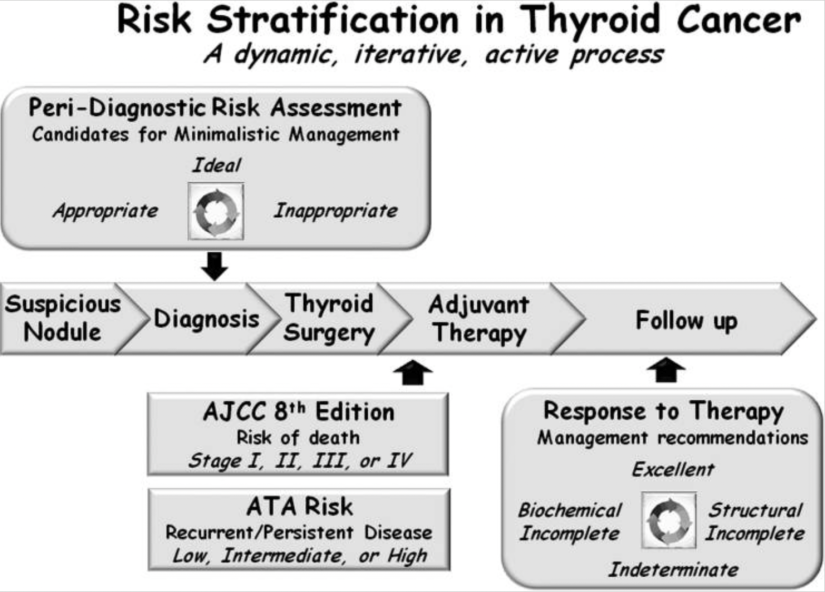
- To treat intra-thyroidal papillary thyroid carcinomas less than 4 cm in properly selected patients
- Now accept a minimalistic surgical approach (thyroid lobectomy without neck dissection):
- Careful peri-diagnosis, preoperative, and intra-operative risk stratification:
- Are the keys to successful use of thyroid lobectomy without having to perform an unacceptable rate of early-completion thyroidectomies
- Patients classified as being ideal for lobectomy would have:
- Papillary micro-carcinomas:
- That appeared to be confined to the thyroid:
- In the setting of an otherwise normal thyroid ultrasound and clinical N0 neck
- That appeared to be confined to the thyroid:
- Papillary micro-carcinomas:
- Patients are classified as appropriate for lobectomy if:
- The tumor is 1 to 4 cm in maximum dimension:
- If the contralateral lobe is normal, or if there are other abnormalities on the ultrasound, such as thyroiditis or benign-appearing nodules (again, in the setting of the clinical N0 neck)
- Patients with extra-thyroidal extension, clinical N1 disease, or distant metastasis:
- Would be considered inappropriate for thyroid lobectomy as initial therapy
- The tumor is 1 to 4 cm in maximum dimension:
- In addition to the relevance of peri-diagnostic and preoperative risk stratification with respect to the selection of thyroid lobectomy as initial therapy:
- It is important to recognize that there are intra-operative findings:
- That should alter that recommendation and lead to an immediate total thyroidectomy
- It is important to recognize that there are intra-operative findings:
- However, even with appropriate preoperative and intra-operative risk stratification:
- As many as 6% to 20% of patients:
- Will have unexpected findings on the final pathology report:
- That may lead to a completion thyroidectomy and usually, radioactive iodine
- Will have unexpected findings on the final pathology report:
- An additional 5% to 10% may require completion thyroidectomy at some later point during follow-up for diagnostic or therapeutic purposes
- As many as 6% to 20% of patients:
- The rate of early-completion thyroidectomy:
- Performed following review of the initial pathology report, will vary:
- Depending on how aggressive each management team is with regard to the use of radioactive iodine:
- For either remnant ablation or adjuvant treatment
- If minor factors, such as minor extrathyroidal extension, very small-volume lymph node metastasis, or small tumors with aggressive histologic features:
- Usually lead to radioactive iodine therapy,:
- Then the completion thyroidectomy rate may be as high as 20%
- Usually lead to radioactive iodine therapy,:
- Depending on how aggressive each management team is with regard to the use of radioactive iodine:
- The most common reason for completion thyroidectomy:
- Is unanticipated, extensive vascular invasion:
- Documented on the pathology report that obviously could not be visualized preoperatively or intra-operatively
- Is unanticipated, extensive vascular invasion:
- Performed following review of the initial pathology report, will vary:
- Thus, patients need to understand that the final determination of whether a thyroid lobectomy is the appropriate initial therapy:
- Can only be achieved by the integration of preoperative, intra-operative, and postoperative risk stratification
- Patients who are uncomfortable with this approach:
- Will often choose a total thyroidectomy as initial therapy
- Patients motivated to keep part of the thyroid will often accept that uncertainty:
- Recognizing that the final decision regarding the completeness of initial therapy cannot be completely known until several weeks after the surgery is completed when more complete risk stratification can be accomplished
#Arrangoiz #ThyroidSurgeon #ThyroidExpert #CancerSurgeon #HeadandNeckSurgeon #SurgicalOncologist #ThyroidCancer #DynamicRiskStratification
