- In October 2016, the AJCC (www.cancerstaging.org) published the eighth edition of the AJCC / TNM cancer staging system:
- Which replaced the seventh edition that had been used by clinicians, cancer registries, and researchers since 2009
- On 1 January 2018, tumor registries officially began using the eighth edition for tumor staging
- Whereas the staging tables for medullary thyroid cancer and anaplastic thyroid cancer showed only minimal changes:
- The rules for the staging of well-differentiated thyroid cancer underwent substantial modifications:
- These included the following:
- An increase of the age cutoff:
- From 45 years to 55 years of age at diagnosis
- Removal of microscopic extra-thyroidal extension:
- As a key component of the staging system
- No longer mandating assignment of stage III to older patients with microscopic extra-thyroidal extension or lymph node metastases
- Establishment of a new T3b category for tumors of any size:
- That demonstrate gross extra-thyroidal extension involving only the surrounding strap muscles
- An increase of the age cutoff:
- These included the following:
- The rules for the staging of well-differentiated thyroid cancer underwent substantial modifications:
- The AJCC Differentiated Thyroid Cancer Committee:
- Carefully considered the possibility of inclusion of molecular markers (specifically, BRAFV600E and TERT promoter mutations) in the AJCC prognostic staging definitions:
- Whereas both of these mutations, particularly when present together:
- Have been shown to be predictors of poor clinical outcomes:
- They appeared to add only marginal benefit to the traditional anatomic staging factors (this might change in the next staging system with new data coming out)
- Thus, molecular characterization of differentiated thyroid cancers, although providing some prognostic information:
- Were not powerful enough factors to merit upstaging tumors to prognostic stages above those mandated by TNM risk factors
- Nonetheless, similar to the approach used in the ATA risk-stratification system:
- Molecular results can be used to refine further and individualize risk within risk categories or stages
- Whereas both of these mutations, particularly when present together:
- Carefully considered the possibility of inclusion of molecular markers (specifically, BRAFV600E and TERT promoter mutations) in the AJCC prognostic staging definitions:
- The three critical factors that determine the prognostic stage groups of the eighth edition AJCC / TNM cancer staging system include:
- The age at diagnosis
- The presence or absence of distant metastases
- The presence or absence of gross extra-thyroidal extension
- Rather than the use of the standard TNM staging tables provided in the AJCC / TNM manual, this flow diagram to stage patients rapidly based on the key clinical risk factors (age at diagnosis, distant metastasis, gross extrathyroidal extension, and lymph node metastases) may be easier
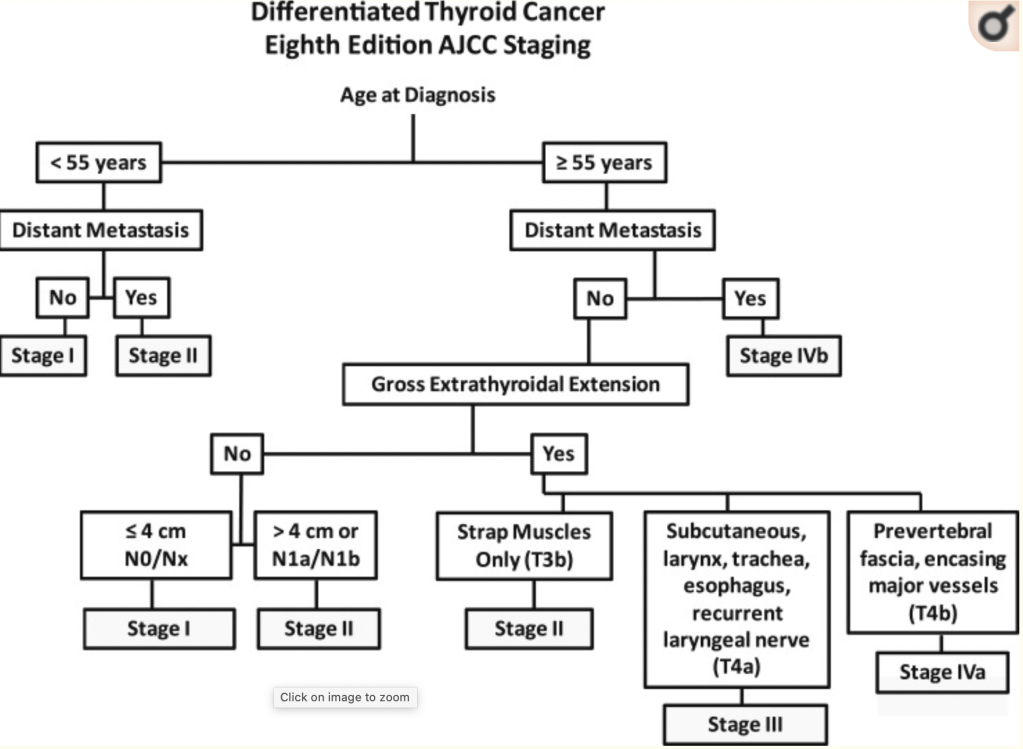
- Patients age less than 55 years:
- Rapidly classifies patients as either:
- Stage I:
- Any T, any N, M0 or
- Stage II:
- Any T, any N, M1
- Stage I:
- Rapidly classifies patients as either:
- In the older patients, additional factors, such as:
- The presence or absence of distant metastasis
- Invasion of strap muscles
- Extent of gross extra-thyroidal extension:
- Are also used to define the prognostic stage groups
- In the eighth edition of the AJCC / TNM cancer staging system:
- It was anticipated that the majority of patients would be classified as stage I or stage II:
- Reflecting the excellent outcomes expected in the majority of thyroid cancer patients
- A smaller number of patients, particularly the older patients with either distant metastases or gross extra-thyroidal extension:
- Were anticipated to do worse and are therefore classified as stage III or IV
- It was anticipated that the majority of patients would be classified as stage I or stage II:
- Multiple publications have demonstrated that the eighth edition of the AJCC / TNM cancer staging system:
- Moved a substantial number of patients into lower prognostic stage groups:
- Without affecting the overall survival of those lower-stage groups
- The patients who remained in the higher-stage groups:
- Had poorer prognoses, as expected
- This resulted in a much better separation of the four prognostic stage groups:
- With respect to survival:
- Such that 5- to 10-year disease-specific survival (DSS) was:
- 99% in stage I patients
- 88% to 97% in stage II patients
- 72% to 85% in stage III patients
- 67% to 72% in stage IV patients
- Such that 5- to 10-year disease-specific survival (DSS) was:
- With respect to survival:
- Unlike previous editions of the AJCC / TNM staging system in which there was substantial overlap in survival in patients with stage I, II, and III disease:
- The eighth edition provides meaningful separation among the prognostic stage groups that appear to be clinically relevant
- The differences in predicted and published ∼10-year survival rates:
- Are best seen when analyzed based on age group (age <55 years vs age ≥55 years)
- Moved a substantial number of patients into lower prognostic stage groups:
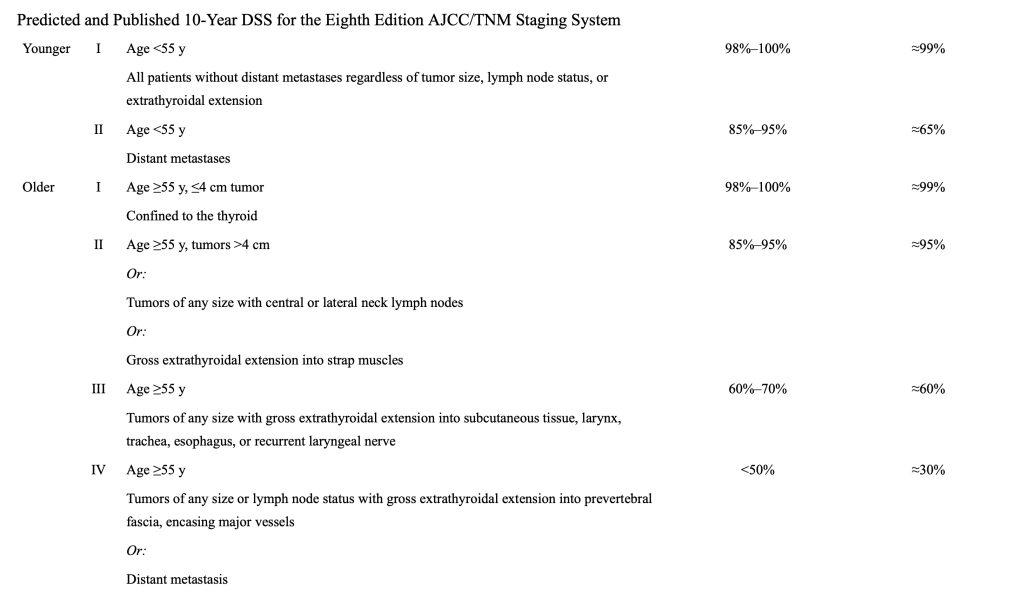
- The predicted 10-year DSS has been validated for all age and stage groups:
- With only the younger (age < 55 years) stage II patients:
- Appearing to do more poorly than anticipated
- The lower-than-anticipated 10-year DSS in the younger patients (age < 55 years) with stage II disease:L
- Was the result of the stage migration of patients in the 45- to 55-year age group:
- From seventh edition AJCC stage IV to eighth edition AJCC stage II
- Was the result of the stage migration of patients in the 45- to 55-year age group:
- With only the younger (age < 55 years) stage II patients:
#Arrangoiz #ThyroidSurgeon #ThyroidExpert #ThyroidCancer #CancerSurgeon #SurgicalOncologist #HeadandNeckCancer
