- Although both the AJCC / TNM staging system and the ATA risk-stratification system provide valuable information with regard to initial risk stratification:
- They are both static risk assessments that can only incorporate information available in the peri-diagnostic, preoperative, intraoperative, and early postoperative periods:
- However, all of the static staging systems published provide suboptimal long-term predictions for individual patients:
- As demonstrated by the proportion of variance explained, ranging from 20% to 30% across a wide range of studies (a measure of how well a predictive model correlates with the final outcome of interest)
- However, when these initial risk estimates:
- Are refined and modified over time as a response to therapy and as a reflection of the underlying biology of a particular patient’s thyroid cancer:
- Risk estimates become more reliable and can achieve a proportion of variance explained as high as 70% to 80%
- Are refined and modified over time as a response to therapy and as a reflection of the underlying biology of a particular patient’s thyroid cancer:
- However, all of the static staging systems published provide suboptimal long-term predictions for individual patients:
- They are both static risk assessments that can only incorporate information available in the peri-diagnostic, preoperative, intraoperative, and early postoperative periods:
- Over the last decade, several groups have developed and validated the general concept of dynamic risk stratification in which the baseline initial risk estimates are continually modified over time as new data become available:
- Initially, dynamic risk stratification was validated only in the setting of total thyroidectomy and radioactive iodine and only in response to initial therapy
- Over the last several years, it has become readily apparent that the concept of dynamic risk stratification should not be restricted to response to initial therapy:
- But should rather be used to reclassify each patient when they return for their follow-up visits
- Furthermore, definitions for response to therapy outcomes have been published and validated for patients receiving total thyroidectomy without radioactive iodine and even for low-risk patients treated with lobectomy alone
- In patients treated with total thyroidectomy and radioactive iodine, the ATA guidelines provided a set of definitions, clinical outcomes, and management implications for the use of dynamic risk stratification:
- In this paradigm, at each follow-up visit, the patient is classified as having an:
- Excellent, biochemically incomplete, structurally incomplete, or indeterminate response to therapy Unlike the AJCC/TNM staging and the ATA risk-stratification systems, the response-to-therapy category can change over time as new data become available at each visit
- In this paradigm, at each follow-up visit, the patient is classified as having an:
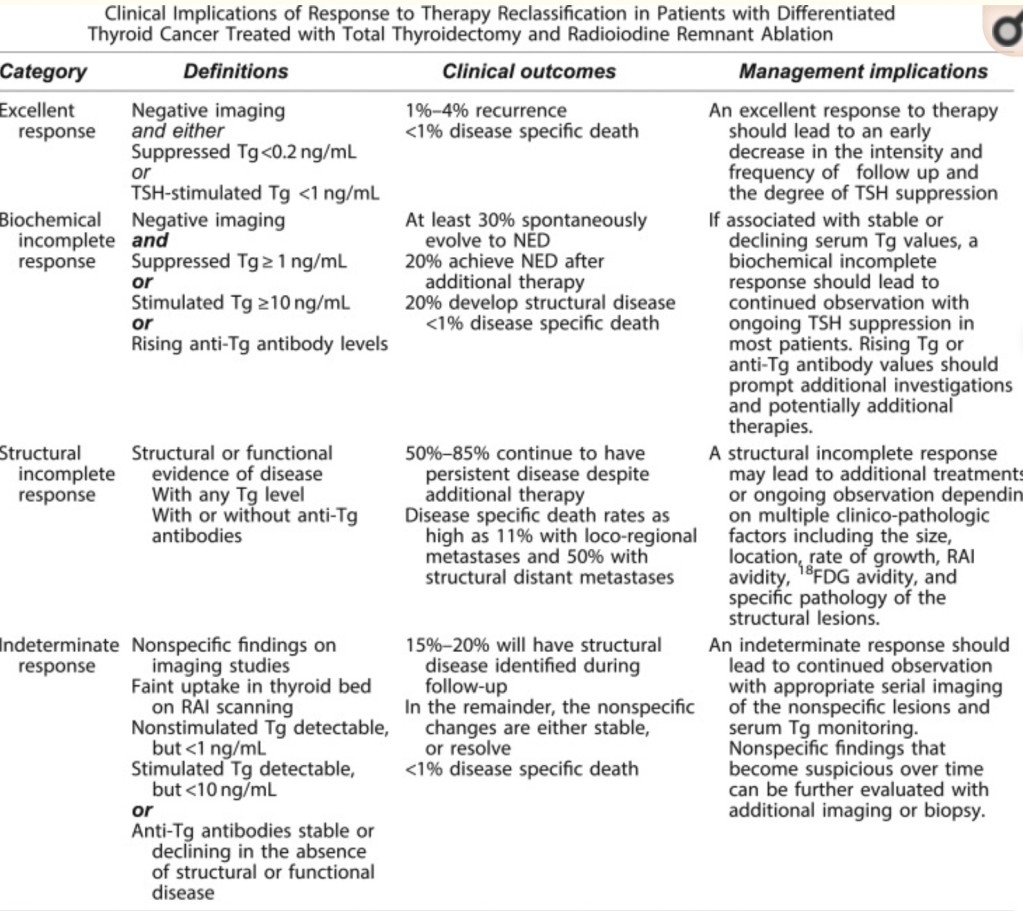
- Patients who have an excellent response to therapy:
- Are expected to have essentially a normal overall survival and a very low risk of disease recurrence and therefore may not require intensive follow-up
- Patients with biochemical incomplete response:
- Have an abnormal Tg value but no structurally identifiable disease:
- Are usually followed with observation unless the Tg or Tg antibodies are rising:
- In which case additional imaging and evaluations are warranted to try to identify the source of the abnormal Tg
- Are usually followed with observation unless the Tg or Tg antibodies are rising:
- Have an abnormal Tg value but no structurally identifiable disease:
- The indeterminate response category:
- Initially described as acceptable response:
- Was designed to be a temporary holding area for patients with nonspecific findings that could not be confidently described as benign or malignant
- Over time, roughly 15% to 20% of these patients:
- Will develop structural disease that may require additional therapy
- In the remainder, the nonspecific changes are either stable or resolve:
- Many of these patients can be reclassified as having an excellent response over time
- Whereas patients with rising anti-Tg antibodies are classified as having a:
- Biochemical incomplete response
- Patients with stable or declining anti-Tg antibodies are categorized as having an:
- Indeterminate response to therapy
- Although Tg assays that use a liquid chromotography-tandem mass spectroscopy (LC-MS/MS) methodology:
- Can identify some Tg antibody-positive patients as having detectable Tg in the setting of known structural disease:
- Up to 20% to 40% of patients with structural disease will have undetectable Tg measurements on LC-MS/MS
- Thus, in the setting of antithyroglobulin antibodies, an undetectable Tg obtained on the current LC-MS/MS assays is insufficient evidence to classify a patient as having an excellent response
- Can identify some Tg antibody-positive patients as having detectable Tg in the setting of known structural disease:
- Patients with a structural incomplete response:
- Are particularly challenging in that the majority of them:
- Will continue to have persistent disease despite additional therapies:
- In this is the category of patients from which nearly all of the disease-specific mortality arises
- Will continue to have persistent disease despite additional therapies:
- These patients are likely to need additional imaging, ongoing thyroid-stimulating hormone suppression, and additional therapies over time
- Are particularly challenging in that the majority of them:
- Initially described as acceptable response:
#Arrangoiz #ThyroidSurgeon #ThyroidExpert #HeadandNeckSurgeon #CancerSurgeon #SurgicalOncologist
