Blog
What is the Origin / Etiology of Primary Hyperparathyroidism?
- The precise origin of PHPT is unknown:
- Although exposure to low-dose therapeutic ionizing radiation and familial predisposition account for some cases:
- Irradiation for acne:
- Could have accounted for a 2 to 3-fold increase in the incidence of this disease at some point in time
- 4-fold increase was noted in survivors of the atomic bomb
- Irradiation for acne:
- Schneider et al., in their study of 2555 patients followed for 50 years:
- Even low doses of radiation exposure during the teenage years:
- Was associated with a slight risk of developing PHPT
- In this study a dose response was documented in people receiving external-beam radiotherapy for benign diseases before their 16th birthday
- The latency period for the development of PHPT after radiation exposure:
- Is longer than that for the development of thyroid tumors:
- With most cases occurring 30 to 40 years after exposure
- Is longer than that for the development of thyroid tumors:
- Patients who have been radiated have:
- Similar clinical manifestations and serum calcium levels when compared to patients without a history of radiation exposure:
- However, the former tend to have higher PTH levels and a higher incidence of concomitant thyroid neoplasms
- Similar clinical manifestations and serum calcium levels when compared to patients without a history of radiation exposure:
- Even low doses of radiation exposure during the teenage years:
- Although exposure to low-dose therapeutic ionizing radiation and familial predisposition account for some cases:
- Certain medications have been implicated in the development of hypercalcemia:
- Lithium therapy has been known to:
- Shift the set point for PTH secretion in parathyroid cells:
- Thereby resulting in elevated PTH levels and mild hypercalcemia
- Lithium stimulates the growth of abnormal parathyroid glands in vitro and also in susceptible patients in vivo
- Unusual metabolic features associated with lithium use include:
- Low urinary calcium excretion
- Normal cyclic AMP excretion
- Lack of calcic nephrolithiasis
- The mechanism probably results from:
- Lithium linking with the calcium sensing receptor on the parathyroid glands resulting in PTH secretion
- Shift the set point for PTH secretion in parathyroid cells:
- Lithium therapy has been known to:
- Elevated serum calcium levels have been associated with thiazide diuretic:
- The overall annual age- and sex-adjusted (to 2000 U.S. whites) incidence was:
- 7.7 (95% CI, 5.9 to 9.5) per 100,000 individuals
- The average 24-hour plasma calcium concentrations are increased with thiazide diuretic use:
- But the mean 24-hour PTH levels remain unchanged:
- In subjects with normal baseline PTH levels and no evidence of hypercalciuria
- But the mean 24-hour PTH levels remain unchanged:
- Thiazides diuretics have several metabolic effects that may contribute to increased calcium levels:
- A decrease in urine calcium excretion is the most likely cause:
- But in some cases diuretic use has been associates with a metabolic alkalosis:
- That could also increase the total serum calcium levels through a pH-dependent increase in protein-bound calcium
- But in some cases diuretic use has been associates with a metabolic alkalosis:
- Although plasma 1,25 (OH) vitamin D levels are unchanged:
- Increased intestinal calcium absorption in response to thiazide diurectic use:
- Has been noted and could also contribute to an increase in serum calcium
- Increased intestinal calcium absorption in response to thiazide diurectic use:
- One last possible explanation for the elevated serum calcium levels associated with thiazide diuretic use is:
- Hemoconcentration associated with dieresis
- A decrease in urine calcium excretion is the most likely cause:
- The overall annual age- and sex-adjusted (to 2000 U.S. whites) incidence was:
- Numerous genetic abnormalities have been identified in the development of PHPT, including:
- Anomalies in tumor suppressor genes and proto-oncogenes
- Specific DNA mutations in a parathyroid cell:
- May confer a proliferative advantage over normal neighboring cells:
- Thus allowing for clonal growth:
- Large populations of these altered cells containing the same mutation within hyper functioning parathyroid tissue:
- Suggest that such glands are a result of:
- Clonal expansion
- Suggest that such glands are a result of:
- Large populations of these altered cells containing the same mutation within hyper functioning parathyroid tissue:
- Thus allowing for clonal growth:
- Anomalies in tumor suppressor genes and proto-oncogenes
- The majority of PHPT cases are:
- Sporadic
- Nonetheless, PHPT also occurs within the spectrum of a number of inherited disorders such as:
- Multiple endocrine neoplasia syndromes (MEN):
- MEN type 1 (Wermer Syndrome)
- MEN type 2A (Sipple Syndrome)
- Isolated familial HPT
- Familial HPT with jaw-tumor syndrome
- Multiple endocrine neoplasia syndromes (MEN):
- All of these are inherited in an:
- Autosomal dominant fashion

#Arrangoiz #ParathyroidSurgeon #ParathyroidExpert #Hyperparathyroidism #PrimaryHyperparathyroidism #CancerSurgeon #EndocrineSurgery #Teacher #Surgeon #HeadandNeckSurgeon #SurgicalOncologist #ParathyroidAdenoma #Hypercalcemia #ElevatedCalciumLevels #Miami #MountSinaiMedicalCenter #MSMC #Mexico #Hialeah
Para spinal Space
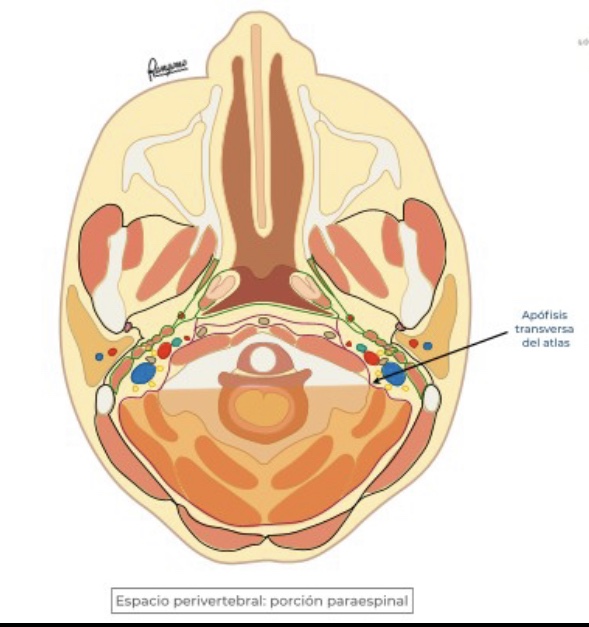
- Towards the posterior of the transverse processes of the cervical vertebrae, deep cervical aponeurosis delimits the “paraspinal portion” of the perivertebral space
- It contains, the paraspinal muscles in the skull and neck
- Among the muscles in intimate relationship with the skull we will highlight the lateral rectum of the head, the splenium capitis and the muscles of the nape of the neck
- In the neck the paraspinal portion of the perivertebral space houses the middle and posterior scalene muscles, the levator muscle of the scapula, the cervical splenium and (a segment) of the splenio capitis… among others
Epidemiology of Primary Hyperparathyroidism
- Primary hyperparathyroidism (PHPT):
- There are approximately 100,000 new cases per year reported in the United States
- Since the advent of routine laboratory testing:
- The prevalence of the disease has increased from:
- 0.1% to 0.4%:
- One to seven cases per 1000 adults
- 0.1% to 0.4%:
- The prevalence of the disease has increased from:
- In a study by Yeh et al:
- The incidence of PHPT fluctuated between:
- 36.3 and 120.2 cases per 100,000 women-years
- 13.4 and 35.6 cases per 100,000 men-years
- The incidence of PHPT fluctuated between:
- PHPT may present at any age:
- With the vast majority of cases occur in patients:
- Older than 45 years of age
- The mean age at diagnosis has remained between:
- 52 and 56 years
- With the vast majority of cases occur in patients:
- Women have consistently made up the preponderance of cases:
- With a female-to-male ratio of:
- 3:1 to 4:1
- Based on a population based study from Rochester Minnesota:
- The higher incidence of this could be secondary (hypothetically) to:
- Estrogen deficiency after menopause:
- That reveals underlying HPT
- Estrogen deficiency after menopause:
- The higher incidence of this could be secondary (hypothetically) to:
- With a female-to-male ratio of:

#Arrangoiz #ParathyroidSurgeon #ParathyroidExpert #Hyperparathyroidism #PrimaryHyperparathyroidism #CancerSurgeon #EndocrineSurgery #Teacher #Surgeon #HeadandNeckSurgeon #SurgicalOncologist #ParathyroidAdenoma #Hypercalcemia #ElevatedCalciumLevels #Miami #MountSinaiMedicalCenter #MSMC #Mexico #Hialeah
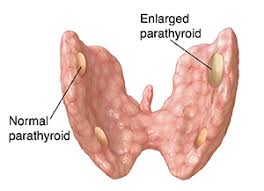
What is Primary Hyperparathyroidism?
- Primary hyperparathyroidism (PHPT):
- Arises from an unregulated overproduction of parathyroid hormone (PTH) from an abnormal parathyroid gland
- Hypercalcemia or widely fluctuating levels of serum calcium resulting from:
- The inappropriate or autogenous secretion of PTH:
- By one or more parathyroid glands:
- In the absence of a known or recognized stimulus
- By one or more parathyroid glands:
- The inappropriate or autogenous secretion of PTH:
- The most common cause of hypercalcemia in the outpatient setting is:
- Primary hyperparathyroidism (PHPT)
#Arrangoiz #ParathyroidSurgeon #ParathyroidExpert #Hyperparathyroidism #PrimaryHyperparathyroidism #CancerSurgeon #EndocrineSurgery #Teacher #Surgeon #HeadandNeckSurgeon #SurgicalOncologist #ParathyroidAdenoma #Hypercalcemia #ElevatedCalciumLevels #Miami #MountSinaiMedicalCenter #MSMC #Mexico #Hialeah
Advancements in the Treatment of Differentiated Thyroid Cancer (DTC)
Radioiodine Ablation
- The American Thyroid Association (ATA) recommends radioiodine (RAI) adjuvant therapy for:
- High risk DTC patients after total thyroidectomy
- Prior to RAI therapy:
- Serum TSH, thyroglobulin (Tg), and anti-Tg antibody measurements should be obtained
- Patients should be instructed to:
- Maintain a low iodine diet (50 mg / day) for 1 to 2 weeks
- And undergo thyroid hormone withdrawal
- Levothyroxine (LT4):
- Should be discontinued 3 to 4 weeks prior to RAI, and
- Liothyronine (LT3):
- Should be discontinued 2 weeks prior to therapy
- ATA low and intermediate risk DTC patients and patients with contraindications to a hypothyroid state:
- May undergo recombinant human TSH stimulation instead of thyroid hormone withdrawal
- The 5-year follow-up results of the ESTIMABL1 trial:
- A randomized control trial investigating rhTSH versus thyroid hormone withdrawal and low activity (1.1 GBq) versus high activity (3.7GBq) RAI in patients with low-risk DTC:
- Showed no evidence of disease regardless of preparation method or radioiodine dose used, providing further support for the use of rhTSH and 1.1 GBq radioactive iodine in these patients
- A randomized control trial investigating rhTSH versus thyroid hormone withdrawal and low activity (1.1 GBq) versus high activity (3.7GBq) RAI in patients with low-risk DTC:
- For advanced DTC:
- Dosimetry might be appropriate to quantify RAI uptake and determine dosing given the variability from person to person, and within cells of the same tissue
- The goals of RAI therapy include:
- Destroying occult disease foci
- Eliminating residual healthy tissue that may serve as a locus for neoplastic transformation
- Improving the specificity of Tg as a tumor marker, and of whole body RAI scans during long-term surveillance
- A dose of 30mCi is recommended over higher doses in lower-risk patients, but high-risk patients may require 100 to 200 mCi
- During RAI ablation, 131I is taken up by follicular thyroid cells, where the molecules accumulate and undergo beta decay:
- This process is optimized by functional sodium iodide symporter expression (NIS):
- Dedifferentiating tumors lose NIS expression and become fluorodeoxyglucose (FDG) avid as they lose RAI avidity:
- For this reason, FDG-PET (positron emission tomography) positive tumors:
- Tend to be more aggressive and unlikely to respond to RAI
- This process is optimized by functional sodium iodide symporter expression (NIS):
- Age greater than 40 years, large tumor burden, and Hürthle cell histology:
- Are also indicators of poor response
- MAPK and PI3K / AKT activation:
- Is thought to decrease NIS activity
- Tumors with RAS mutations may be more likely to be RAI avid than those with BRAF and TERTmutations
- Side effects of RAI therapy include:
- Nausea
- Temporary or permanent salivary gland and lacrimal duct dysfunction
- Sialadenitis
- Parotitis
- Thyroiditis
- Bone marrow and gonadal dysfunction
- Adequate hydration might help alleviate symptoms
- There is also a risk of second primary cancer of:
- Soft tissue, salivary gland, colon, and blood, associated with higher cumulative doses
- Less than 10% of DTC patients will develop metastatic disease
- Of these, approximately one in three experience complete remission after RAI therapy
- The ATA recommends a whole body scan with or without single photon emission computed tomography (SPECT) / computed tomography (CT) to determine RAI avidity for residual structural disease after therapy
#Arrangoiz #ThyroidSurgeon #ThyroidCancer #ThyroidExpert #CancerSurgeon #HeadandNeckSurgeon #EndocrineSurgery #MountSinaiMedicalCenter #MSMC #Miami #Mexico #RAI #RadioActiveIodine
Rodrigo Arrangóiz MS, MD, FACS, FSSO
- Mount Sinai Medical Center (Main Campus)4306 Alton Road, 2nd Floor, Miami Beach, FL 33140
- Mount Sinai Emergency Center and Primary & Specialty Care Hialeah6050 West 20th Ave., Hialeah, FL 33016


Rodrigo Arrangóiz MS, MD, FACS, FSSO
My Locations
- Mount Sinai Medical Center (Main Campus)4306 Alton Road, 2nd Floor, Miami Beach, FL 33140
- Mount Sinai Emergency Center and Primary & Specialty Care Hialeah6050 West 20th Ave., Hialeah, FL 33016

Papillary Thyroid Carcinoma in a Thyroglossal Duct
- Thyroglossal duct remnants are commonly seen:
- Comprising more than:
- 75% of midline neck tumors in children
- 7% in adults
- Comprising more than:
- Finding a cancer within one of these cysts is rare:
- One large study reported a prevalence of cancer:
- In 1.3% of remnants
- PTC is the most common tumor (90%):
- Most are less than 1 cm
- They are typically confined to the cyst
- One large study reported a prevalence of cancer:
- Because so few cases have been reported,:
- No consensus exists about the optimal management
- Most agree that a Sistrunk procedure is the best way to excise a thyroglossal duct cancer:
- The necessity for total thyroidectomy is controversial:
- As only 25% to 56% of patients have concomitant malignancy in the thyroid
- A retrospective analysis of 18 patients treated at one institution found that:
- 75% had lateral with or without central lymph node metastases
- 56% were found to have tumor foci in the thyroid
- Twelve patients were given radioiodine
- With a median follow-up of 12 years (range 1 to 22 years), 11 patients had stimulated thyroglobulin levels available; 10 were undetectable, the other was 2 ng/mL, and all had a negative neck ultrasound
- Other studies have reported similarly encouraging results with follow-up, regardless of the treatment
- The necessity for total thyroidectomy is controversial:
#Arrangoiz #ThyroidSurgeon #CancerSurgeon #SurgicalOncologist #HeadandNeckSurgeon #EndocrineSurgery #ThyroidCancer #ThyroglossalDuctCystCancer #PapillaryThyroidCancer #Miami #Mexico #MountSinaiMedicalCenter
Thyroid surgery for differentiated thyroid cancer — recent advances and future
Thyroid surgery for differentiated thyroid cancer — recent advances and future directions
Tracy S. Wang & Julie Ann Sosa
Nature Reviews Endocrinology volume 14, pages670–683 (2018)
Key points
The incidence of thyroid cancer is increasing; this includes thyroid cancers of all tumour sizes and stages.
Molecular testing for indeterminate thyroid nodules continues to evolve and guide recommendations for the extent of thyroid surgery.
Appropriate extent of thyroidectomy for patients with low-risk thyroid cancer remains dynamic and might include active surveillance, thyroid lobectomy or total thyroidectomy.
Given the excellent outcomes for most patients with differentiated thyroid cancer, patient preference and a robust discussion regarding options for the extent of surgery and long-term surveillance are critical.
A strong association exists between surgeon volume and patient outcomes; surgeons’ awareness of their own outcomes is critical.
Referring providers, payers and policymakers should be aware of the implications of the association between surgeon volume and patient outcomes so that patient access to experienced thyroid surgeons can be optimized.
-
El entrenamiento y el volumen del cirujano son factores críticos para obtener el mejor resultado con las menores complicaciones en la cirugía de tiroides.

-
Ashok Shaha MD, FACScirujano de cabeza y cuello de Memorial Sloan Kettering Cancer Center experto en tiroides durante su plática inaugural de la American Head and Neck Society nos habla de quien debe estar realizando cirugía de tiroides.
REPORT THIS AD
Rodrigo Arrangoiz MS, MD, FACS cirujano de tumores de cabeza y cuello y cirugía endocrina de Mount Sinai Medical Center cumple con los requisitos determinados por el Dr. Saha para realizar cirugía de tiroides.
Su entrenamiento fue el siguiente:
• Cirugia general y gastrointestinal
• Michigan State University:
• 2004 al 2010 • Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina:
• Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012 • Maestria en ciencias (Clinical research for healthprofessionals):
• Maestria en ciencias (Clinical research for healthprofessionals):
• Drexel University (Filadelfia):
• 2010 al 2012 • Cirugia de tumores de cabeza y cuello / cirugiaendocrina
• Cirugia de tumores de cabeza y cuello / cirugiaendocrina
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016
#Arrangoiz
#CirugiadeTumoresdeCabezayCuello
#CirugiaEndocrina
#CirugiaOncologica
#HeadandNeckSurgery
#EndocrineSurgery
#SurgicalOncology
#MountSinaiMedicalCenter
#Miami #Mexico
