My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
The European Organisation for Research and Treatment of Cancer (EORTC) 10981 After Mapping of the Axilla, Radiation or Surgery? (AMAROS) trial:
Randomized 4806:
Clinically node-negative
T1 to T2 tumors:
To completion axillary lymph node dissection (ALND) or axillary radiation (AR):
If they had positive nodes
Of the 1425 patients with positive sentinel nodes:
744 had been randomly assigned to ALND
681 to AR
Initially:
Patients with tumors 3 cm or smaller were eligible:
But the protocol was later modified to include:
Tumors up to 5 cm, multifocal tumors, or both
In the AR arm 21% of patients had T2 lesions
There were no age limits for eligibility:
Patients ranged from age 48 to 64 years
In the AR arm:
42% of women were premenopausal
Patients who had either partial or total mastectomy were enrolled in the trial:
18% of women had mastectomy
There was no limit on the number of positive nodes for the radiation arm:
But the majority of patients had 1 or 2 positive nodes
Crossover was allowed:
For patients with extensive axillary disease:
From the radiation arm to the dissection arm
Patients in the dissection arm who had 4 or more positive nodes:
Where allowed to have axillary radiation
Four percent of patients who stayed in the radiation arm had 3 positive nodes, and 1% had 4 or more positive nodes.
Importantly:
In the axillary dissection arm:
25% of patients had an additional 1 to 3 positive nodes (in addition to the positive sentinel nodes) at dissection
8% had 4 or more additional positive nodes
Since it was a randomized trial:
We can assume the same numbers were present in the radiation arm:
So these patients did not necessarily have low-volume axillary disease.
Axillary radiotherapy (RT) included:
The contents of all 3 levels of the axilla and the medial part of the supraclavicular fossa
The prescribed dose was 25 fractions of 2 Gy each
For patients in the AR arm who had mastectomy:
Radiation to the chest wall in addition to the axilla was optional but not mandatory
There were no significant differences:
In 5-year overall survival or disease-free survival between the two arms:
At 6.1 years of follow-up:
There was no significant difference:
In the rate of axillary failure:
0.43% ALND vs 1.19% RT
At 5-year follow-up there was a significant difference:
In clinical signs of lymphedema between the groups:
23% in ALND vs. 11% in AR:
There was greater than a 10% difference in arm size compared to the contralateral arm:
In 13% of the ALND arm and 5% of the AR arm
The AMAROS study findings would suggest that axillary RT is an appropriate alternative to ALND in patients with a positive sentinel node:
However, the clinical characteristics of the AMAROS cohort are remarkably similar to the American College of Surgeons Oncology Group (ACOSOG) Z0011 cohort:
With 80% of AMAROS patients having:
A tumor less than 2 cm
90% patients:
Receiving any systemic therapy
95% of patients:
Having only 1 to 2 positive sentinel nodes
Patients in ACOSOG Z0011 treated with sentinel lymph node biopsy only demonstrated:
Similar 5-year rates of regional recurrence as the AMAROS patients receiving axillary RT:
0.9% [ACOSOG Z0011] vs 1.2% [EORTC 10981 AMAROS axillary RT]):
Thus, while AMAROS indicates that sentinel node biopsy and nodal RT is an alternative to ALND:
It does not demonstrate that RT is necessary in all patients with a positive sentinel node:
Particularly in those treated with breast-conserving surgery
The decision to include axillary RT in patients with 1 to 2 positive sentinel nodes:
Should be tailored to the individual:
Taking into account other clinical factors which may place the patient at higher risk for locoregional recurrence
Multiple groups have attempted to define a favorable subgroup of women in whom the omission of adjuvant irradiation following a partial mastectomy is reasonable:The CALGB 9343 trial:Randomized women:Ages 70 years and older
With clinical stage I (T1,N0,M0) disease:To tamoxifen for 5 years versus tamoxifen plus whole-breast irradiationPatients with estrogen receptor-negative tumors were excluded
Most tumors were 2 cm or less
Surgical margins were required to be negative:Defined as the absence of tumor at the inked margin
Adjuvant whole-breast irradiation:Significantly reduced the risk of local or regional failure:From 10% to 2% at 10 yearsThere were no significant differences in:Distant disease-free survival or overall survival between the groups
The PRIME II trial:Enrolled 1326 patients:Ages 65 years and older
T1 to T2
Node-negative tumors
Clear margins
Following breast-conserving surgery:Patients received endocrine therapyAnd were randomized to adjuvant radiation therapy or no further treatment
At 5 years:Those undergoing radiation:Demonstrated a reduction in local recurrence:4.1% vs 1.3%
With no difference in survival
Typical breast tangents:Without targeted nodal irradiation:Would be appropriate for a patient with pN0 disease
Adjuvant irradiation reduces the risk of ipsilateral breast tumor recurrence regardless of whether the margins are positive:A positive margin:Significantly increases the risk of local failure despite irradiation
Following breast-conserving surgery (partial mastectomy, lumpectomy):
Adjuvant radiotherapy is recommended due to benefits in:
Local control
Potentially breast cancer mortality.
The Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) meta-analysis:
Found that for patients undergoing breast-conserving surgery that are N0:
Radiationreduced:
The risk of any recurrence:
From 31% to 16%
Reduced breast cancer mortality:
From 21% to 17%
The EBCTCG also found that for patients undergoing mastectomy with 1 to 3 positive nodes:
Radiotherapy was associated with a:
Reduction in locoregional recurrence (LRR):
From 20% to 4%
Reduction in breast cancer mortality:
From 50% to 42%
Although many have interpreted the EBCTCG findings to mean:
All postmastectomy patients with 1 to 3 positive nodes should have postmastectomy radiation therapy (PMRT):
The patients enrolled in the trials in that meta-analysis were from a different era:
Making it difficult to know how relevant the findings are to patients who are diagnosed and treated by current standards:
The patients were enrolled between 1964 and 1986
Many of them did not receive systemic therapy:
The 64% who received chemotherapy were treated with:
Cyclophosphamide, methotrexate, and fluorouracil:
Which is inferior to modern regimens
Only 24% of patients were treated with tamoxifen
No patients received an aromatase inhibitor.
The benefit of PMRT diminishes:
As the risk of LRR diminishes
Patients with 1 to 3 positive nodes in the meta-analysis who were not treated with PMRT:
Had a 20% rate of LRR (vs. 4%):
But recurrence is significantly lower with modern systemic treatment:
Sharma et al. retrospectively reviewed patients:
Who had mastectomies between 1997 and 2002 and did not receive PMRT:
The 10-year rate of LRR in patients with 1 to 3 positive nodes:
Was only 4.3%:
Compared to 20% in the EBCTCG meta-analysis
Another study of patients with 1 to 3 positive nodes:
Compared the risk of LRR:
Between two different eras, before and after the routine use of sentinel node biopsy, taxane therapy, and aromatase inhibitors:
Use of PMRT reduced the 15-year rate of LRR in the first era:
From 14.5% to 6.1%
PMRT did not appear to benefit patients treated in the second era:
With 5-year LRR rates of:
2.8% without PMRT
4.2% with PMRT
The NSABP B-28 study:
Randomized node-positive patients to:
Doxorubicin and cyclophosphamide versus doxorubicin and cyclophosphamide plus paclitaxel
Use of PMRT was not allowed in patients who were treated with mastectomy:
So the trial gives a good view of the risk of LRR for node-positive patients who are treated with mastectomy and relatively modern systemic therapy.
For patients with 1 to 3 positive nodes:
LRR at 10 years was:
6% for patients with high-risk oncotype DX recurrence scores
4.1% with intermediate-risk oncotype DX recurrence scores
2.4% with low-risk oncotype DX recurrence scores
Lai et al. recently reviewed 293 mastectomy patients with T1 to T2 breast cancer and 1 to 3 positive lymph nodes:
All received anthracycline or taxane based chemotherapy and none received PMRT.
After stratifying patients according to:
Luminal A and B, luminal HER2, HER2, and triple-negative subtypes:
They found patients with triple-negative breast cancer to have the highest 5-year LRR when compared to all other subtypes:
10.6% vs 4.2%:
P=0.05
Multivariate analysis found that the following factors significantly increased the risk of LRR:
Patients younger than age 40 years
Tumors larger than 3 cm
The presence of extensive intraductal components .
The authors concluded that:
Administering modern systemic therapy to early breast cancer patients not receiving PMRT:
Significantly reduces the rate of LRR.
In view of the fact that PMRT significantly increased overall mortality in node-negative patients in the EBCTCG (47.6% vs 41.6%; rate ratio 1.23):
Caution should be taken in extrapolating the results to all patients with 1 to 3 positive nodes in the modern era.
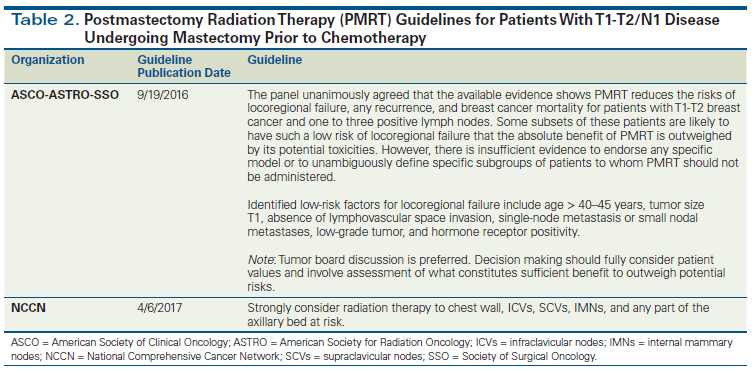
The American Society of Clinical Oncology, the American Society for Radiation Oncology, and the Society of Surgical Oncology:
Recently released an updated consensus statement regarding the role of PMRT in women with 1 to 3 positive lymph nodes:
The consensus panel unanimously agreed that PMRT in this subset of patients (with T1 to T2 breast cancer with 1 to 3 positive lymph nodes):
Reduces local-regional failure
Any recurrence
Breast cancer mortality in patients.
They agreed that the decision for PMRT:
Should be made in a multidisciplinary setting
With the involvement of the patient and her wishes after she is presented with all available data.
The panel went on to acknowledge that in some subsets of patients:
The risk of local-regional failure may be so low that the:
Absolute benefit of PMRT is outweighed by its toxicities.
Further, even if axillary lymph node dissection is omitted in the setting of a positive lymph node:
PMRT should only be used if there is already significant evidence justifying the benefit of PMRT without knowing the status of any additional axillary nodes.
When given:
PMRT should include the:
Internal mammary, supraclavicular, and apical axillary nodes and the chest wall or reconstructed breast.
All patients with a positive axillary node after receipt of neoadjuvant chemotherapy should receive PMRT
En Sociedad Quirúrgica S.C. nuestra prioridad y único interés es el bienestar de nuestros pacientes.
Nuestros servicios brindan total dedicación al paciente para restablecer su estado de salud mediante el empleo de conocimientos médicos vigentes y técnicas de vanguardia cuya efectividad se ha demostrado científicamente. Más aún, correspondemos a la confianza depositada en nosotros al brindar tratamiento óptimo con ética y honestidad.
Sociedad Quirúrgica S.C. está integrada por un selecto grupo de cirujanos generales con varias subespecialidades en distintas áreas quirúrgicas que permiten optimizar el manejo multidisciplinario de nuestros pacientes mediante el trabajo en equipo:
Todo el Staff de Sociedad Quirúrgica ha tenido entrenamiento de posgrado en distinguidas instituciones del extranjero tales como: Mayo Clinic (Rochester, Minnesota); Michigan State University (Michigan); Fox Chase Cancer Center (Philadelphia); Drexel University (Philadephia), Univerity of Chicago (IL), University of Pittsburgh (PA), y Darthmouth University (NH).
Además de nuestra práctica clínica, los cirujanos de Sociedad Quirúrgica estamos involucrados en actividades de docencia tanto de pregrado como posgrado a nivel institucional y privado:
Estamos involucrados en actividades académicas a través de nuestra participación en diferentes asociaciones médico-quirúrgicas tanto a nivel nacional como internacional y realizamos actividades de investigación clínica en las áreas que nos competen.
Estamos seguros que todas éstas actividades se complementan y resultan en beneficios tangibles para nuestros pacientes al permitirnos aplicar día a día las técnicas más avanzadas y eficaces para lograr diagnósticos certeros y tratamientos óptimos en nuestros pacientes.
En Sociedad Quirúrgica S.C. nos hemos dado a la tarea de satisfacer las demandas de salud de la población de Ciudad de México y sus alrededores ofreciendo servicios integrales de prevención y tratamiento contra las enfermedades:
Para lograr esto, contamos con la tecnología más avanzada en instalaciones y equipos, así como médicos profesionales especializados en diversas áreas de la medicina.
Hyperthyroidism is approximately 10 times less common than hypothyroidism:
Symptoms and signs of thyrotoxicosis are listed in the Table.
Hyperthyroid elderly patients often have more cardiac symptoms but less systemic manifestations of thyrotoxicosis.
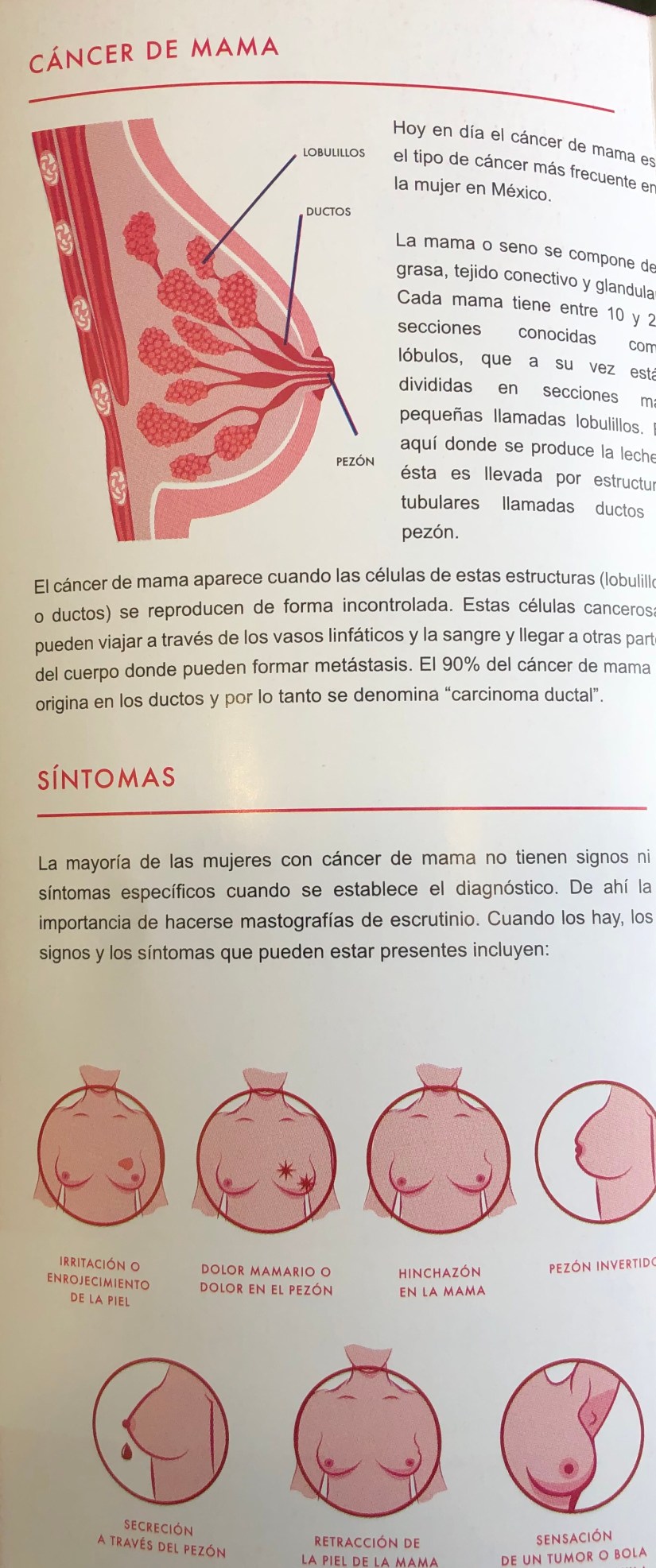
Patients with suspected hyperthyroid syndrome should be evaluated for signs or symptoms of:
Weight loss, heat intolerance, tremor, palpitations, anxiety, menstrual abnormalities, and new onset atrial fibrillation.
Evaluation should be considered, especially in patients with increased risk of hyperthyroidism, including:
A strong family history of thyroid dysfunction (hypothyroidism and hyperthyroidism)
Other autoimmune conditions
Long-standing goiter:
Especially after contrast or amiodarone administration.
Routine screening of asymptomatic patients for hyperthyroidism is not recommended.
General
Skin
Weight loss
Excess perspiration
Heat intolerance
Palmer erythema
Anxiety / nervousness
Insomnia
Nervous System
Muscle weakness
Tremor
Anxiety / nervousness
Cardiovascular
Hyperkinesis
Tachycardia
Palpitations
Gastrointestinal
Dyspnea on exertion
Frequent stools / diarrhea
Bounding pulses
Atrial fibrillation
Reproductive
Irregular menstrual periods / amenorrhea
Head and Neck
Light menstrual flow
Ophthalmopathy (Graves’ disease only: proptosis and chemosis)
Infertility
Stare
Gynecomastia (males)
Goiter
Thyroid Tests in the Evaluation of Thyrotoxicosis
Measurement of serum TSH:
Is the most sensitive way to diagnose hyperthyroidism:
As it is always suppressed in primary hyperthyroidism.
Patients with hyperthyroidism will almost always have a serum TSH concentration of:
Less than 0.1 mIU/L and often under 0.05 mIU/L:
The use of a second-generation TSH assay with a functional sensitivity of < 0.2 mIU/L is sufficient for the diagnosis and management of hyperthyroidism.
Secondary hyperthyroidism from a:
Is extremely rare but should be suspected when the patient has symptoms suggestive of hyperthyroidism with an inappropriately “normal” TSH:
This rare clinical condition should be referred to an endocrinologist for further diagnosis and management.
Certain medical conditions (severe non-thyroidal illness, acute starvation, first-trimester pregnancy) and medications (glucocorticoids, dopamine), in addition to hypothalamic or pituitary disease:
Can result in low TSH:
If any of these conditions are suspected:
The help of a specialist is invaluable for determining the thyroid status of the patient.
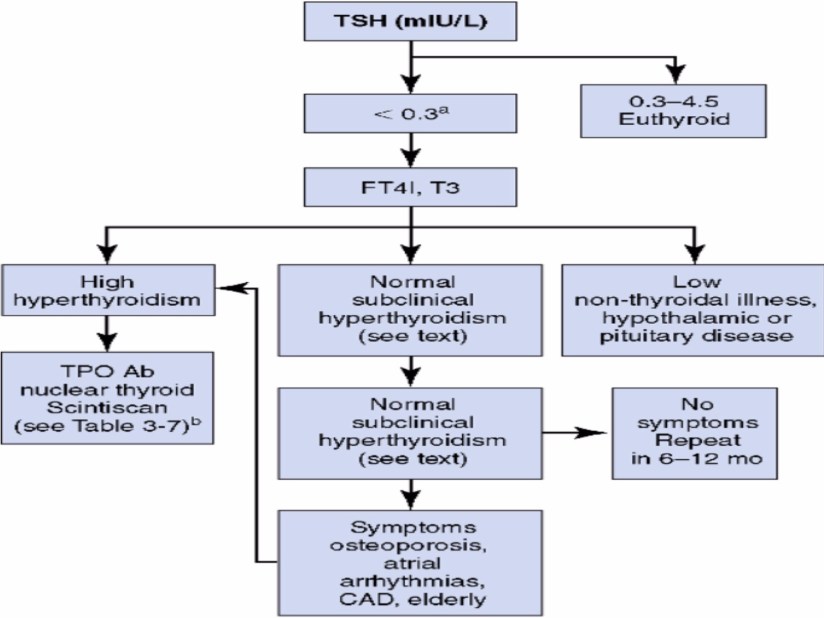
An algorithm for ambulatory thyroid function testing for hyperthyroidism is shown:
If the TSH is within normal limits:
The patient does not have hyperthyroidism:
No further workup is indicated:
Thyroid function tests should be repeated as clinically indicated.
If the TSH is less than 0.3:
Thyroid hormone levels should be determined in addition to repeat measurement of TSH:
Small increases of the thyroid hormone level will cause:
A disproportionate suppression of TSH because of their inverse log-linear relationship.
The degree of hyperthyroidism cannot be assessed by second-generation assay TSH:
Because even very mild thyrotoxicosis will suppress the TSH to very low levels.
Although a third-generation assay can better differentiate between the degrees of hyperthyroidism:
Routine laboratory measurements of:
Total T4, THBR, FT4I, and total T3 can easily and accurately assess the degree of hyperthyroidism.
Measurement of total T3 is needed in the evaluation of hyperthyroidism:
Graves’ disease excretes a relatively high ratio of T3 / T4.
If serum TSH is less than 0.3 and FT4I and total T3 is low:
Hypothalamic or pituitary disease needs to be considered.
Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon / endocrine surgeon / surgical oncologist and is a member of Sociedad Quirúrgica S.C at the America British Cowdray Medical Center in Mexico City:
He is an expert in the surgical management of thyroid diseases.
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012
• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
A dermal neoplasm with cytoplasmic, dense-core neuroendocrine granules and keratin filaments.
MCC is a rare primary cutaneousneuroendocrine malignancy
The incidence of MCC in the United States has recently been reported to have increased by an estimated annual percentage change of 8% from 1986 to 2001:
Approximately 1500 new cases were predicted by the American Cancer Society in the United States alone in 2008.
MCC is one of the few cancers found to be:
Associated with immune suppression
Polyomavirus has been shown to be integrated within the genome
Merkel cell carcinoma (MCC) is an uncommon and aggressive cutaneous neoplasm that lacks distinguishing clinical features.
More than half of Merkel cell carcinomas (MCCs) occur in the head and neck of elderly people in areas of actinically damaged skin:
The most common site of occurrence is the periorbital region.
Merkel cell carcinoma (MCC) has a propensity to recur and to cause:
Local (25% to 30% of the cases) and distant metastases (30% to 35% of the cases).
Distant metastases indicate a condition that is nearly always fatal.
Merkel cell carcinoma (MCC) is a deadly disease with a poor likelihood for survival:
Local recurrence occurs in:
44% of patients:
Multiple local recurrences occur in 15% of patients.
These tumors appear as:
Rapidly growing, painless nodules in elderly caucasian individuals or in young adults with ectodermal dysplasia syndromes.
Merkel cell carcinomas (MCCs) usually appear as:
Indurated plaques or violaceous (red or deep purple) solitary and dome-shaped nodules.
The surface is typically shiny, with telangiectasias and possibly ulceration.
Most tumors measure 0.7 cm to 1.2 cm in diameter.
Merkel cell carcinomas (MCCs) usually occur in sun-damaged skin.
They are often found near other lesions of actinically damaged skin, including skin involved with:
Bowen disease, squamous cell carcinoma, basal cell carcinoma, solar keratoses, or lentigo maligna.
The mean age at presentation is 68 years:
No gender bias is observed.
Merkel cell carcinoma (MCC) has also been linked to:
Previous radiation exposure and B-cell lymphoma.
The nonspecific characteristics of Merkel cell carcinoma (MCC) lead to a lengthy differential diagnosis that includes:
Basal cell carcinoma
Squamous cell carcinoma
Keratoacanthoma
Amelanotic melanoma
Epidermal cysts
Lymphoma
Metastatic carcinoma of the skin
As a result:
Merkel cell carcinoma (MCC) is rarely diagnosed until biopsy is performed
Approximately 53% of Merkel cell carcinomas (MCCs) occur in the head and neck:
35% occur in the extremities.
In the head and neck:
46% of tumors occur in the periorbital region
29%, on the cheek
18%, on the eyelid
17%, on the forehead.
Other sites in the head and neck include:
The lips (9%)
Ears (7%)
Nose and neck (5.4%)
Scalp (4%)
Tumors have also been reported in areas not exposed to sun, such as the:
Nasal cavity
Buccal mucosa
Gingiva
Hard palate
Postauricular skin
Approximately 3% of patients with Merkel cell carcinoma (MCC) have tumors at several sites.
MCC is an aggressive tumor:
With an overall five-year survival of 40%
Reported five year survival rates of local, nodal and metastatic disease are:
64%, 39% and 18%, respectively
Reported rates of regional lymph node involvement at the time of presentation vary from 10% to 45%:
Around 50% of patients with lymph node metastases harbor concurrent distant metastases:
Most often in the:
Liver, lung, brain, bone or skin
MCC has high rates of local recurrence:
25% to 30% of patients.
MCC has high rates of distant metastasis:
30% to 35% of patients.
Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon / endocrine surgeon / surgical oncologist and is a member of Sociedad Quirúrgica S.C at the America British Cowdray Medical Center in Mexico City:
He is an expert in the management Merkel Cell Carcinoma.
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012
• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
Tumor volume (TV) of papillary thyroid carcinoma (PTC) increases exponentially during active surveillance, and the growth rate differs for each patient.
TV doubling time (TVDT) is considered a strong dynamic marker for the prediction of the growth rate and progression of the tumor.
Methods:
This cohort study analyzed 273 PTC patients who underwent active surveillance for more than one year rather than immediate thyroid surgery.
TVDT was calculated in each patient, and patients were divided into two groups:
Rapid-growing (TVDT less than 5 years)
Stable (TVDT of 5 years or more)
Clinical and initial ultrasonography (US) features between the two groups were compared.
Results:
The median patient age was 51.1 years (interquartile range [IQR] 42.2–61.0 years)
76% of the patients were women.
The initial TV of PTC was 62.1 mm3 (IQR 28.1–122.8 mm3)
During a median of 42 months (IQR 29– 61 months) of active surveillance:
10.3% of the patients had a TVDT of less than two years
5.1% had a TVDT between two and three years
6.2% had a TVDT between three and four years
6.6% had a TVDT between four and five years
71.8% had a TVDT of five years or more
Patients in the rapid-growing group (77 patients; 28.2%) were:
Significantly younger ( p = 0.004) than those in the stable group (196 patients; 71.8%):
Being younger than 50 years of age was significantly associated with rapid tumor growth of PTC (odds ratio = 2.31 [confidence interval 1.30–4.31], p = 0.004) in multivariate analysis.
In ultrasound findings:
MacrocalcificatioN:
Was independently associated with rapid tumor growing of PTCs (odds ratio = 4.98 [confidence interval 2.19–11.69], p < 0.001)
Conclusions:
TVDT is a good indicator for presenting the growing velocity of PTCs during active surveillance
Younger age and macrocalcification in the initial US:
Were associated with rapid-growing PTCs
Determination of TVDT during the early phase of active surveillance may be helpful for the prediction of rapidly progressing PTCs and deciding whether to adopt an early surgical approach.
Rodrigo Arrangoiz MS, MD, FACS es especialista en Cirugía de Tumores de Cabeza y Cuello / Cirugía Endocrina y Cirugía Oncológica compleja. Fue egresado como Médico General de la Universidad Anahuac Suma Cum Laude. Es miembro de Sociedad Quirúrgica S.C. que es el único grupo quirúrgico en México en donde todos los socios se entrenaron en las mejores instituciones académicas de los Estados Unidos de América. El Doctor Arrangoiz es experto en el manejo del Cáncer de Tiroides, Patología Quirúrgica de Tiroides, Hiperparatiroidismo Primario, Tumores de Cabeza y Cuello y Cáncer de Mama.
Fue entrenado en las mejores instituciones académicas de los Estados Unidos y mantiene certificaciones por los Consejos de Cirugía General y Cirugía Oncológica en México y en los Estados Unidos de América. Su entrenamiento incluyó:
Cirugía General y Gastrointestinal – Michigan State University (2004 – 2010)
Cirugía Oncológica / Tumores de Cabeza y Cuello / Cirugía Endocrina – Fox Chase Cancer Center en Filadelfia (2010 al 2012)
Maestría en Ciencias (Clinical Research for Health Professionals) – Drexel University (Filadelfia) (2010 – 2012)
Cirugía de Tumores de Cabeza y Cuello / Cirugía Endocrina (2014 al 2016) – IFHNOS / Memorial Sloan Kettering Cancer Center
Ha participado en múltiples cursos y congresos como Conferencista y Profesor Invitado, así mismo ha realizado diversas publicaciones y artículos sobre temas relacionados con su especialidad. Se encuentra certificado por el Consejo Mexicano de Cirugía General y el Consejo Mexicano de Oncología así como es de los pocos mexicanos certificado por, el AMERICAN BOARD OF SURGERY, el cuál le faculta como cirujano con licencia en los EU. Es miembro de diversas asociaciones médicas como el American College of Surgeons, American Thyroid Association, American Society of Endocrine Surgeons, American Medical Association, American Society of Clinical Oncology, Association of Academic Surgeons, Society of Surgical Oncology, The Society of Surgery of the Alimentary Tract, Society of American Gastrointestinal Endoscopic Surgeons, y la American Society of Breast Surgeons, entre otras.
Es pionero en México de la cirugía minimamente invasiva radioguiada de paratiroides, técnica inventada por el Dr. James Norman, para el tratamiento del hiperparatiroidismo primario. Tiene múltiples publicaciones en revista internacionales sobre la patología del hiperparatiroidismo primario.
Gracias a esto el Dr. Rodrigo Arrangoiz es reconocido como uno de los mejores especialistas en Cirugía de Tumores de Cabeza y Cuello / Cirugía Endocrina / Cirugía Oncológica en México, además de ser galardonado como uno de los 50 mejores médicos de México en los Top Doctors Awards 2018.
El Dr. Fernando Cordera González de Cosío es un experimentado Cirujano Oncólogo con formación en instituciones de alto prestigio como la Clínica Mayo Rochester, Fox Chase Cancer Center de Filadelfia, EITS en Francia y Memorial Sloan Kettering de Nueva York.
Su trayectoria se ha desarrollado principalmente en USA y México. Actualmente ejerce como Cirujano Oncólogo en el Centro Médico ABC y en el Hospital Ángeles Lomas.
Cuenta con más de 20 años de experiencia siendo experto en el tratamiento y diagnóstico del Cáncer de mama, Cáncer de Tiroides, Cirugía Oncológica cabeza y cuello, Melanoma, Sarcoma, entre otros.
Asimismo, es Presidente de la Práctica Médica Grupal de Cirugía Oncológica del Centro Médico ABC en la Ciudad de México.
Está Certificado por el American Board of Surgery, el Consejo Mexicano de Cirugía General y el Consejo Mexicano de Oncología.
Su aportación a la investigación y formación de acuerdo a su especialidad es extensa; cuenta con más de 10 años de experiencia en intervenciones como profesor y ponente en cursos, congresos y simposios a nivel nacional e internacional.
Ha publicado más de 45 artículos médicos a nivel nacional e internacional. En el 2004 fue galardonado con el Kaare K. Nygaard Award de la Clínica Mayo para Outstanding Surgical Research Achievement y en el 2009 recibió otro premio, el Prize to the Medical Achievement for a Better Life por la Organización Internacional para la Capacitación e Investigación Médica.
Gracias a esto el Dr. González de Cosío es reconocido como uno de los mejores especialistas en Cirugía Oncológica de la Ciudad de México.