
- Following breast-conserving surgery (partial mastectomy, lumpectomy):
- Adjuvant radiotherapy is recommended due to benefits in:
- Local control
- Potentially breast cancer mortality.
- Adjuvant radiotherapy is recommended due to benefits in:
- The Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) meta-analysis:
- Found that for patients undergoing breast-conserving surgery that are N0:
- Radiation reduced:
- The risk of any recurrence:
- From 31% to 16%
- Reduced breast cancer mortality:
- From 21% to 17%
- The risk of any recurrence:
- Radiation reduced:
- The EBCTCG also found that for patients undergoing mastectomy with 1 to 3 positive nodes:
- Radiotherapy was associated with a:
- Reduction in locoregional recurrence (LRR):
- From 20% to 4%
- Reduction in breast cancer mortality:
- From 50% to 42%
- Reduction in locoregional recurrence (LRR):
- Radiotherapy was associated with a:
- Although many have interpreted the EBCTCG findings to mean:
- All postmastectomy patients with 1 to 3 positive nodes should have postmastectomy radiation therapy (PMRT):
- The patients enrolled in the trials in that meta-analysis were from a different era:
- Making it difficult to know how relevant the findings are to patients who are diagnosed and treated by current standards:
- The patients were enrolled between 1964 and 1986
- Many of them did not receive systemic therapy:
- The 64% who received chemotherapy were treated with:
- Cyclophosphamide, methotrexate, and fluorouracil:
- Which is inferior to modern regimens
- Cyclophosphamide, methotrexate, and fluorouracil:
- The 64% who received chemotherapy were treated with:
- Only 24% of patients were treated with tamoxifen
- No patients received an aromatase inhibitor.
- Making it difficult to know how relevant the findings are to patients who are diagnosed and treated by current standards:
- The patients enrolled in the trials in that meta-analysis were from a different era:
- The benefit of PMRT diminishes:
- As the risk of LRR diminishes
- Patients with 1 to 3 positive nodes in the meta-analysis who were not treated with PMRT:
- Had a 20% rate of LRR (vs. 4%):
- But recurrence is significantly lower with modern systemic treatment:
- Sharma et al. retrospectively reviewed patients:
- Who had mastectomies between 1997 and 2002 and did not receive PMRT:
- The 10-year rate of LRR in patients with 1 to 3 positive nodes:
- Was only 4.3%:
- Compared to 20% in the EBCTCG meta-analysis
- Was only 4.3%:
- The 10-year rate of LRR in patients with 1 to 3 positive nodes:
- Who had mastectomies between 1997 and 2002 and did not receive PMRT:
- Another study of patients with 1 to 3 positive nodes:
- Compared the risk of LRR:
- Between two different eras, before and after the routine use of sentinel node biopsy, taxane therapy, and aromatase inhibitors:
- Use of PMRT reduced the 15-year rate of LRR in the first era:
- From 14.5% to 6.1%
- PMRT did not appear to benefit patients treated in the second era:
- With 5-year LRR rates of:
- 2.8% without PMRT
- 4.2% with PMRT
- With 5-year LRR rates of:
- Use of PMRT reduced the 15-year rate of LRR in the first era:
- Between two different eras, before and after the routine use of sentinel node biopsy, taxane therapy, and aromatase inhibitors:
- Compared the risk of LRR:
- The NSABP B-28 study:
- Randomized node-positive patients to:
- Doxorubicin and cyclophosphamide versus doxorubicin and cyclophosphamide plus paclitaxel
- Use of PMRT was not allowed in patients who were treated with mastectomy:
- So the trial gives a good view of the risk of LRR for node-positive patients who are treated with mastectomy and relatively modern systemic therapy.
- For patients with 1 to 3 positive nodes:
- LRR at 10 years was:
- 6% for patients with high-risk oncotype DX recurrence scores
- 4.1% with intermediate-risk oncotype DX recurrence scores
- 2.4% with low-risk oncotype DX recurrence scores
- LRR at 10 years was:
- Randomized node-positive patients to:
- Lai et al. recently reviewed 293 mastectomy patients with T1 to T2 breast cancer and 1 to 3 positive lymph nodes:
- All received anthracycline or taxane based chemotherapy and none received PMRT.
- After stratifying patients according to:
- Luminal A and B, luminal HER2, HER2, and triple-negative subtypes:
- They found patients with triple-negative breast cancer to have the highest 5-year LRR when compared to all other subtypes:
- 10.6% vs 4.2%:
- P=0.05
- 10.6% vs 4.2%:
- They found patients with triple-negative breast cancer to have the highest 5-year LRR when compared to all other subtypes:
- Multivariate analysis found that the following factors significantly increased the risk of LRR:
- Patients younger than age 40 years
- Tumors larger than 3 cm
- The presence of extensive intraductal components .
- The authors concluded that:
- Administering modern systemic therapy to early breast cancer patients not receiving PMRT:
- Significantly reduces the rate of LRR.
- Administering modern systemic therapy to early breast cancer patients not receiving PMRT:
- Luminal A and B, luminal HER2, HER2, and triple-negative subtypes:
- Sharma et al. retrospectively reviewed patients:
- In view of the fact that PMRT significantly increased overall mortality in node-negative patients in the EBCTCG (47.6% vs 41.6%; rate ratio 1.23):
- Caution should be taken in extrapolating the results to all patients with 1 to 3 positive nodes in the modern era.
- But recurrence is significantly lower with modern systemic treatment:
- Had a 20% rate of LRR (vs. 4%):
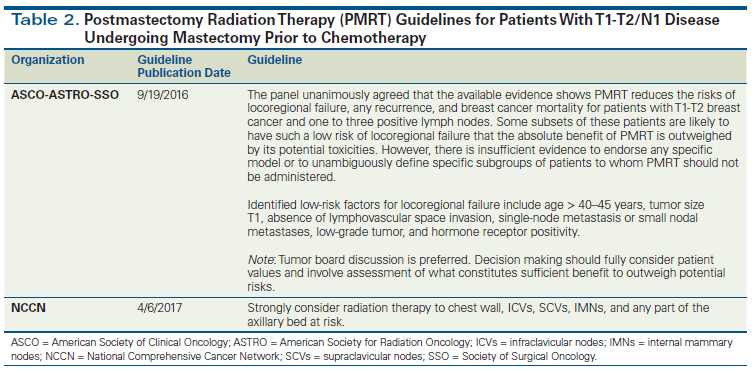
- The American Society of Clinical Oncology, the American Society for Radiation Oncology, and the Society of Surgical Oncology:
- Recently released an updated consensus statement regarding the role of PMRT in women with 1 to 3 positive lymph nodes:
- The consensus panel unanimously agreed that PMRT in this subset of patients (with T1 to T2 breast cancer with 1 to 3 positive lymph nodes):
- Reduces local-regional failure
- Any recurrence
- Breast cancer mortality in patients.
- They agreed that the decision for PMRT:
- Should be made in a multidisciplinary setting
- With the involvement of the patient and her wishes after she is presented with all available data.
- The panel went on to acknowledge that in some subsets of patients:
- The risk of local-regional failure may be so low that the:
- Absolute benefit of PMRT is outweighed by its toxicities.
- The risk of local-regional failure may be so low that the:
- Further, even if axillary lymph node dissection is omitted in the setting of a positive lymph node:
- PMRT should only be used if there is already significant evidence justifying the benefit of PMRT without knowing the status of any additional axillary nodes.
- When given:
- PMRT should include the:
- Internal mammary, supraclavicular, and apical axillary nodes and the chest wall or reconstructed breast.
- PMRT should include the:
- All patients with a positive axillary node after receipt of neoadjuvant chemotherapy should receive PMRT
- The consensus panel unanimously agreed that PMRT in this subset of patients (with T1 to T2 breast cancer with 1 to 3 positive lymph nodes):
- Recently released an updated consensus statement regarding the role of PMRT in women with 1 to 3 positive lymph nodes:
- All postmastectomy patients with 1 to 3 positive nodes should have postmastectomy radiation therapy (PMRT):
- Found that for patients undergoing breast-conserving surgery that are N0:
#Arrangoiz
#Teacher
#Surgeon
#Cirujano
#SurgicalOncologist
#CirujanoOncologo
#CancerSurgeon
#CirujanodeCancer
#BreastSurgeon
#BreastCancer
#CancerdeMama
#CirujanodeMama
