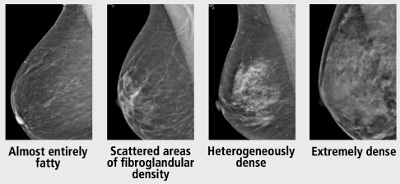
- According to the 5th edition of the ACR BI-RADS® Atlas, visual estimation of breast fibroglandular composition should be defined by one of the following four descriptions:
- Almost entirely fatty
- Scattered areas of fibroglandular density
- Heterogeneously dense
- Extremely dense
👉The U.S. population distribution of breast density is as follows:
- 10% almost entirely fatty
- 40% scattered areas of fibroglandular density
- 40% heterogeneously dense
- 10% extremely dense
👉Women with heterogeneously dense or extremely dense breasts are considered to have “dense breasts.”
👉Sensitivity of mammography decreases as breast density increases.
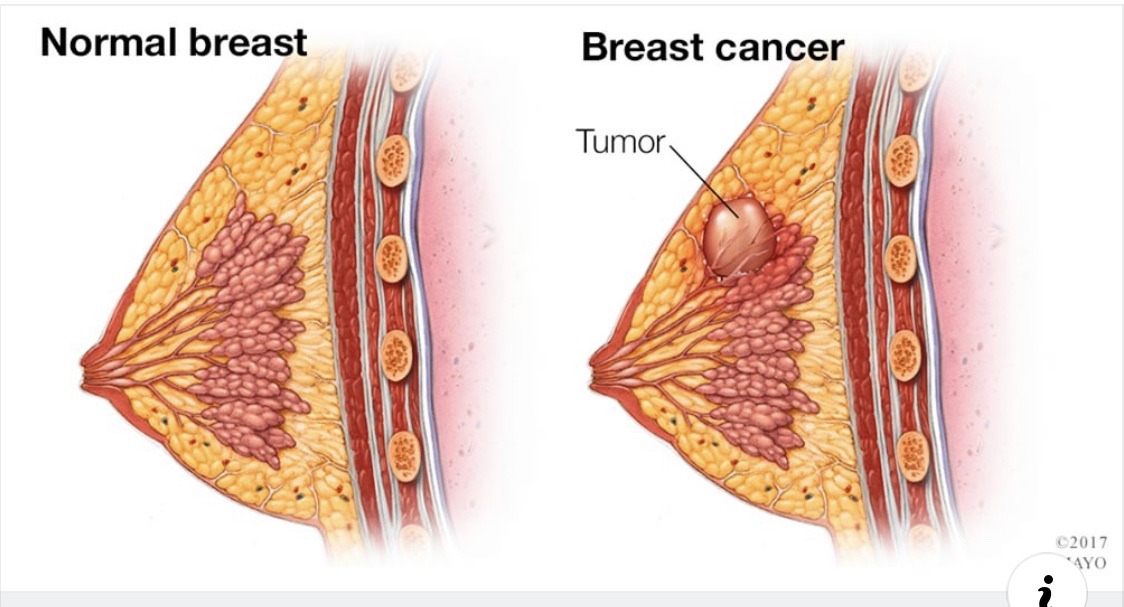
👉Increased breast density not only has a masking effect which may obscure masses, but also serves as an independent risk factor for breast cancer.
👉It has been reported that the increased risk may be as much as 4- to 6-fold.
👉Estimates this high are obtained when comparing women with dense breasts to those with fatty replaced breasts.
👉Since only 10% of women have fatty replaced breasts, it makes more sense to make the comparison with women of average breast density.
👉The relative risk for cancer in women with heterogeneously dense breasts compared with the average woman is approximately 1.2, and the relative risk for cancer in women with extremely dense breasts compared with the average woman is approximately 2.1.
👉In general, breast density decreases with increasing age and increasing body mass index, so it is not the absolute density that is a risk factor, but the difference in the observed and expected density—the so called “residual density.”
👉Several states have recently passed legislation requiring women with dense breasts to be specifically informed of their breast density.
👉Women are informed of the limitations of mammography in dense breasts and are instructed to discuss further management with their physicians.
👉An informed decision regarding potential use of supplemental screening options, in addition to mammography, should be discussed, factoring in elements such as overall breast cancer risk as well as the positives and negatives of additional screening.
👉Despite a lack of consensus, algorithms for screening women with dense breasts are available and often emphasize breast cancer risk.
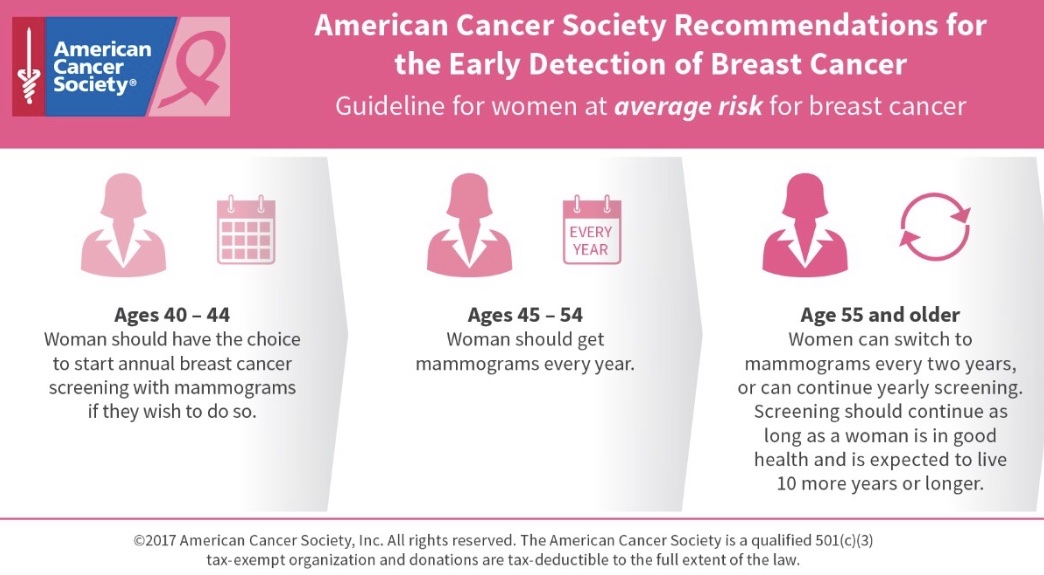
👉Women with heterogeneously dense breasts (or extremely dense breasts) with no additional risk factors require only annual mammography.
👉The decision to pursue additional imaging in patients with elevated risk should supplement but never entirely replace mammography.
👉Biannual screening mammography is not considered appropriate, and there is no indication for thermography.
👉Use of screening ultrasound or MRI are appropriate for women at increased risk, but the benefit remains to be determined in women of average risk for breast cancer.

👉Rodrigo Arrangoiz MS, MD, FACS cirujano oncology y cirujano de mamá de Sociedad Quirúrgica S.C en el America British Cowdray Medical Center en la ciudad de Mexico:
-
Es experto en el manejo del cáncer de mama.

👉Es miembro de la American Society of Breast Surgeons:

Training:
• General surgery:
• Michigan State University:
• 2004 al 2010

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016


#Arrangoiz
#Surgeon
#Cirujano
#SurgicalOncologist
#CirujanoOncologo
#BreastSurgeon
#CirujanodeMama
#CancerSurgeon
#CirujanodeCancer










 • Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina: • Fox Chase Cancer Center (Filadelfia): • 2010 al 2012
• Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina: • Fox Chase Cancer Center (Filadelfia): • 2010 al 2012 • Maestria en ciencias (Clinical research for healthprofessionals): • Drexel University (Filadelfia): • 2010 al 2012
• Maestria en ciencias (Clinical research for healthprofessionals): • Drexel University (Filadelfia): • 2010 al 2012 • Cirugia de tumores de cabeza y cuello / cirugiaendocrina • IFHNOS / Memorial Sloan Kettering Cancer Center: • 2014 al 2016
• Cirugia de tumores de cabeza y cuello / cirugiaendocrina • IFHNOS / Memorial Sloan Kettering Cancer Center: • 2014 al 2016
