My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
👉Targeted therapies are expanding treatment options in metastatic thyroid cancer (MTC).
👉In the past 10 years, four VEGF inhibitors have been approved for MTC: sorafenib and lenvatinib for differentiated thyroid cancer, and cabozantinib and vandetanib for medullary thyroid cancer.
👉Cabozantinib and vandetanib are also moderate RET inhibitors.
👉In addition, larotrectinib was recently approved for all solid tumors that harbor TRK fusions, and patients with differentiated thyroid cancer are frequently TRK positive.
👉Consequently, knowing what genetic mutations a patient harbors can greatly affect the choice of therapies.
👉Multiple groups have attempted to define a favorable subgroup of women: – In whom the omission of adjuvant irradiation following a partial mastectomy is reasonable
👉One study (CALGB 9343): Randomized women:
– Ages 70 years and older
– Clinical stage I (T1, N0, M0) disease
– To tamoxifen for 5 years versus tamoxifen plus whole-breast irradiation
– Patients with estrogen receptor-negative tumors were excluded
– Most tumors were 2 cm or less, and surgical margins were required to be negative (defined as the absence of tumor at the inked margin)
👉Adjuvant whole-breast irradiation: – Significantly reduced the risk of local or regional failure: From 10% to 2% at 10 years
👉There were no significant differences in: – Distant disease-free survival or overall survival between the groups
👉The PRIME II trial: – Enrolled 1326 patients. – Ages 65 years and older. – With T1 to T2, node negative tumors and clear margins
👉Following breast-conserving surgery: – Patients received endocrine therapy and were randomized to adjuvant radiation therapy or no further treatmento
👉At 5 years those undergoing radiation demonstrated a reduction in local recurrence: – 4.1% vs 1.3% with no difference in survival
They should be carefully differentiated from a complex cyst:
That may require alternative management
Radiographic features:
Ultrasound characteristics:
Thin wall:
With or without posterior acoustic enhancement
Homogenous hypoechoic content
Low-level internal echoes:
Which may change the shape with the patient position o
Sloping fluid / fluid levels
The challenge is to differentiate a complicated from a complex cyst:
As the low internal echos of a complicated cyst:
May appear as a homogeneous hypoechoic mass
If there is hemorrhagic or inflammatory debris which is adherent to the wall:
Applying power Doppler:
Detection of internal vascularity:
Can positively prove it to be a solid mass lesion:
On the other hand, Doppler cannot exclude it
Treatment and prognosis:
Complicated breast cysts:
Have less than 2% risk of malignancy and are recommended to be reported as probably benign
The management is limited to:
Short interval follow up:
If the size changes over six months by greater than 20%:
A diagnostic biopsy is indicated
Aspiration is indicated in a:
Symptomatic patient to relieve the symptoms
Newly detected cyst (+/-)
Enlarging cysts o In all cases, if aspiration reveals serosanguineous fluid:
Cytological analysis:
Should be performed
References:
Impact of In-Person and Electronic Training by Breast Radiologists on Rwandan General Practitioners’ and Nurses’ Skills in Diagnostic Breast Ultrasound. K. Shabani et al., JCO Global Oncology, 2018
Impact of Training on Rwandan Health Care Staffs’ Skills in Diagnostic Breast Ultrasound. John Butonzi et al., JCO Global Oncology, 2018
A meta-analysis demonstrated that a positive surgical margin:
Defined as the presence of invasive disease or ductal carcinoma in situ on ink:
Is associated with at least a 2-fold increase in the risk of ipsilateral breast tumor recurrence (IBTR):
Odds ratio, 1.96:
Which has been confirmed by other series
While a boost may partially mitigate the effect of a positive surgical margin:
The risk of a local failure:
Remains higher than in a patient with a cleared surgical margin treated with boosted whole-breast irradiation
Furthermore, a randomized clinical trial showed:
That increasing the boost dose:
Does not nullify the increased risk of local recurrence associated with a positive surgical margin:
17.5% vs 10.8%:
P=>0.1
This is true regardless of the type and fractionation pattern of the radiotherapy
Neither favorable tumor biology (including receptor status) nor the administration of systemic therapy:
Can completely offset the effect of a positive margin
REFERENCES
Houssami N, Macaskill P, Marinovich ML, Morrow M. The association of surgical margins and local recurrence in women with early-stage invasive breast cancer treated with breast-conserving therapy: a meta-analysis. Ann Surg Oncol. 2014;21:717-730.
Mansfield CM, Komarnicky LT, Schwartz GF, et al. Ten-year results in 1070 patients with stages I and II breast cancer treated by conservative surgery and radiation therapy. Cancer. 1995;75:2328-2336.
Moran MS, Schnitt SJ, Giuliano AE, et al; Society of Surgical Oncology; American Society for Radiation Oncology. Society of Surgical Oncology-American Society for Radiation Oncology consensus guideline on margins for breast-conserving surgery with whole-breast irradiation in stage I and II invasive breast cancer. J Clin Oncol. 2014;32:1507-1515.
Poortmans PM, Collette L, Horiot JC, et al. Impact of the boost dose of 10 Gy versus 26 Gy in patients with early stage breast cancer after a microscopically incomplete lumpectomy: 10-year results of the randomized EORTC boost trial. Radiother Oncol. 2009;90:80-85.
Wazer DE, Schmidt-Ullrich RK, Ruthazer R, et al. Factors determining outcome for breast-conserving irradiation with margin-directed dose escalation to the tumor bed. Int J Radiat Oncol Biol Phys. 1998;40:851-858.
Found that for patients undergoing breast-conserving surgery that are N0:
Radiation reduced the risk of any recurrence:
16% vs 31% and
Reduced breast cancer mortality:
17% vs 21%
The EBCTCG also found that for patients undergoing mastectomy with 1 to 3 positive nodes:
Radiotherapy was associated with a:
Reduction in locoregional recurrence (LRR):
4% vs 20% and
Reduction in breast cancer mortality:
42% vs 50%
Although many have interpreted the EBCTCG findings to mean:
All post-mastectomy patients with 1 to 3 positive nodes should have post-mastectomy radiation therapy (PMRT):
The patients enrolled in the trials in that meta-analysis were from a different era:
And it is difficult to know how relevant the findings are to patients who are diagnosed and treated by current standards
The patients were enrolled between 1964 and 1986:
And many of them did not receive systemic therapy
The 64% who received chemotherapy:
Were treated with cyclophosphamide, methotrexate, and fluorouracil:
Which is inferior to modern regimens
Only 24% of patients were treated with tamoxifen, and
No patients received an aromatase inhibitor
The benefit of PMRT:
Diminishes;
As the risk of LRR diminishes
Patients with 1 to 3 positive nodes in the EBCTCG meta-analysis who were not treated with PMRT:
Had a 20% rate of LRR:
But recurrence is significantly lower with modern systemic treatment
Sharma et al. retrospectively reviewed patients who had mastectomies between 1997 and 2002 and did not receive PMRT:
The 10-year rate of LRR in patients with 1 to 3 positive nodes:
Was only 4.3% compared to 20% in the meta-analysis
Another study of patients with 1 to 3 positive nodes compared the risk of LRR between two different eras:
Before and after the routine use of sentinel node biopsy, taxane therapy, and aromatase inhibitors:
Use of PMRT reduced the 15-year rate of LRR in the first era:
From 14.5% to 6.1%
PMRT did not appear to benefit patients treated in the second era:
With 5-year LRR rates of:;
2.8% without PMRT and 4.2% with PMRT
The NSABP B-28 study:
Randomized node-positive patients to:
Doxorubicin and cyclophosphamide versus
Doxorubicin and cyclophosphamide plus paclitaxel:
Use of PMRT was not allowed in patients who were treated with mastectomy:
So, the trial gives a good view of the risk of LRR for node-positive patients who are treated with mastectomy and relatively modern systemic therapy
For patients with 1 to 3 positive nodes:
LRR at 10 years was 6% for patients with high-risk, 4.1% with intermediate-risk, and 2.4% with low-risk Oncotype DX recurrence scores
Additionally, Lai et al. recently reviewed 293 mastectomy patients with T1 to T2 breast cancer and 1 to 3 positive lymph nodes:
All received anthracycline or taxane based chemotherapy and none received PMRT
After stratifying patients according to luminal A and B, luminal HER2, HER2, and triple-negative subtypes:
They found patients with triple-negative breast cancer:
To have the highest 5-year LRR when compared to all other subtypes:
10.6% vs 4.2%, P=0.05
Multivariate analysis found:
That patients younger than age 40 years, tumors larger than 3 cm, and the presence of extensive intraductal components significantly increased the risk of LRR
The authors concluded that administering modern systemic therapy to early breast cancer patients not receiving PMRT:
Significantly reduces the rate of LRR
In view of the fact that PMR:
Significantly increased overall mortality in node-negative patients in the EBCTCG:
47.6% vs 41.6%; rate ratio 1.23:
Caution should be taken in extrapolating the results to all patients with 1 to 3 positive nodes in the modern era
The American Society of Clinical Oncology (ASCO), the American Society for Radiation Oncology (ASTRO), and the Society of Surgical Oncology (SSO):
Released an updated consensus statement regarding the role of PMRT in women with 1 to 3 positive lymph nodes:
The consensus panel unanimously agreed that PMRT in this subset of patients:
Reduces local-regional failure
Reduces any recurrence
Reduces breast cancer mortality:
In patients with T1 to T2 breast cancer with 1 to 3 positive lymph nodes
They agreed that the decision for PMRT should be made in a multidisciplinary setting and with the involvement of the patient and her wishes after she is presented with all available data
The panel went on to acknowledge that in some subsets of patients:
The risk of local-regional failure may be so low that the absolute benefit of PMRT:
Is outweighed by its toxicities
Further, even if axillary lymph node dissection is omitted in the setting of a positive lymph node:
PMRT should only be used if there is already significant evidence justifying the benefit of PMRT without knowing the status of any additional axillary nodes
When given, PMRT should include:
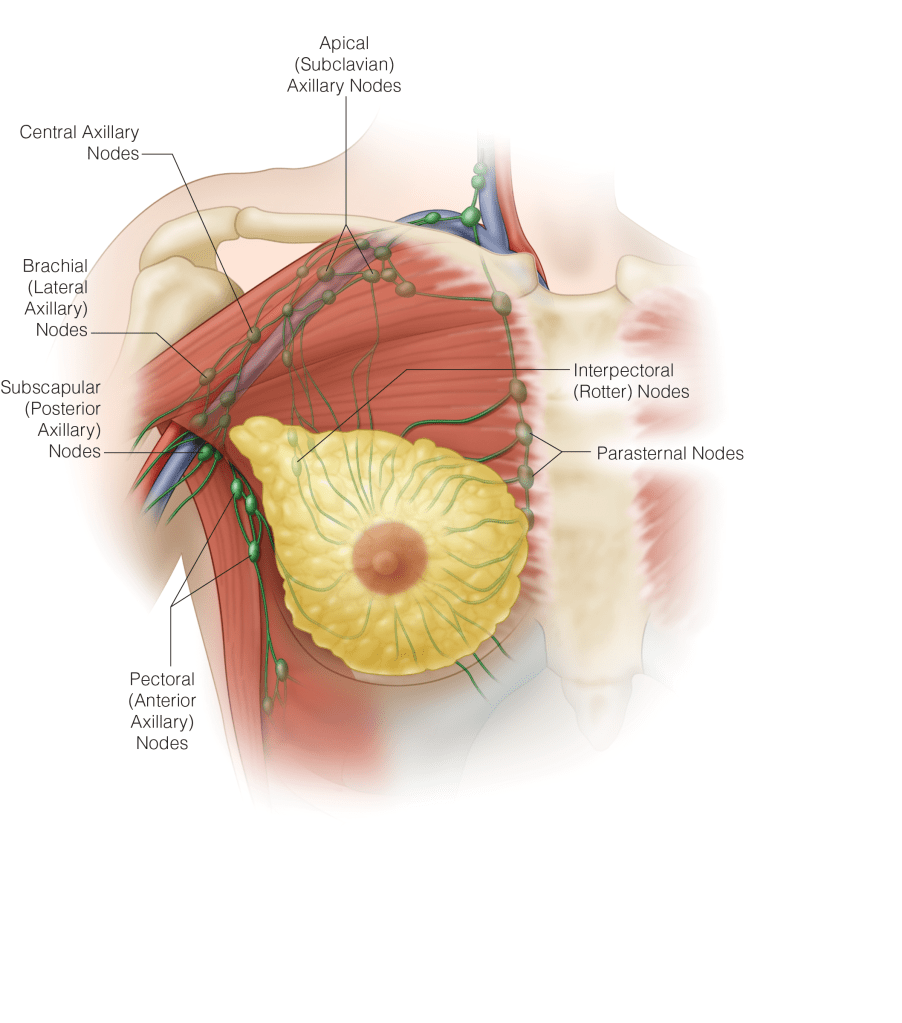
The internal mammary, supraclavicular, and apical axillary nodes and the chest wall or reconstructed breast
All patients with a positive axillary node after receipt of neoadjuvant chemotherapy:
Should receive PMRT
References:
Early Breast Cancer Trialists’ Collaborative Group, Darby S, McGale P, Correa C, et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet. 2011;378:1707-1716.
Early Breast Cancer Trialists’ Collaborative Group, McGale P, Taylor C, Correa C, et al. Effect of radiotherapy after mastectomy on 10-year recurrence and 20-year breast cancer mortality: meta-analysis of individual patient data for 8135 women in 22 randomised trials. Lancet. 2014;383:2127-2135.
Lai SF, Chen YH, Kuo WH, et al. Locoregional recurrence risk for postmastectomy breast cancer patients with T1-2 and one to three positive lymph nodes receiving modern systemic treatment without radiotherapy. Ann Surg Oncol. 2016;23:3860-3869.
Mamounas EP, et al. The 21-gene recurrence score (RS) predicts risk of loco-regional recurrence (LRR) in node (+), ER (+) breast cancer (BC) after adjuvant chemotherapy and tamoxifen: results from NSABP B-28. Presented at: Society of Surgical Oncology Annual Meeting; March 6-9, 2013; National Harbor, MD.
Mamounas EP, Tang G, Paik S, et al. The 21-gene recurrence score (RS) predicts risk of loco-regional recurrence (LRR) in node (+), ER (+) breast cancer (BC) after adjuvant chemotherapy and tamoxifen: results from NSABP B-28. Ann Surg Oncol. 2013;20:S6 (Abstract 2).
McBride A, Allen P, Woodward W, et al. Locoregional recurrence risk for patients with T1,2 breast cancer with 1-3 positive lymph nodes treated with mastectomy and systemic treatment. Int J Radiat Oncol Biol Phys. 2014;89:392–398.
Recht A, Comen EA, Fine RE, et al. Postmastectomy radiotherapy: an American Society of Clinical Oncology, American Society for Radiation Oncology, and Society of Surgical Oncology focused guideline update. Ann Surg Oncol. 2016. [Epub ahead of print].
Sharma R, Bedrosian I, Lucci A, et al. Present-day locoregional control in patients with T1 or T2 breast cancer with 0 or 1 to 3 positive lymph nodes after mastectomy without radiotherapy. Ann Surg Oncol. 2010;17:2899-2908.
👉A mastectomy is an operation to remove all of the breast tissue from a breast as a way to treat or prevent cancer.
👉Mastectomy can be a treatment option for many types of cancer:
Ductal carcinoma in situ or non-invasive breast cancer
Stage I and II (early stage) breast cancer
Stage III (locally advanced) breast cancer, after chemotherapy
Inflammatory breast cancer, after chemotherapy
Paget’s disease of the breast
Locally recurring breast cancer
👉Breast-conserving surgery (partial mastectomy/ lumpectomy), in which only the tumor is removed with negative margins, may be another option.
👉Newer mastectomy techniques can preserve the skin of the breast and allow it to have a more natural appearance – Skin sparing mastectomy
👉Newer mastectomy techniques can preserve the nipple areolar complex of the breast allowing it to have a more natural appearance – Nipple sparing mastectomy
👉Surgery to restore the shape of the breast, called breast reconstruction, can be done at the same time as the mastectomy or during a second operation.
Hialeah, Fla. – July 22, 2020 – Rodrigo Arrangoiz, MD, MS, FACS a fellowship-trained surgical oncologist with a focus in the treatment of breast cancer, thyroid cancer, hyperparathyroidism and other types of head and neck cancers has joined the Center for Advanced Surgical Oncology, a Tenet Florida Physician Services (TFPS) medical practice located in Hialeah. Dr. Arrangoiz’s professional experience includes specialization in benign and malignant thyroid diseases (thyroid cancer), parathyroid diseases (hyperparathyroidism), benign and malignant breast diseases (breast cancer), head and neck surgery (squamous cell carcinomas, salivary gland malignancies), and skin cancers. He is certified by the American Board of General Surgery and graduated from a surgical oncology fellowship accredited by the Society of Surgical Oncology. Dr. Arrangoiz is bilingual in English and Spanish and on-staff at Palmetto General Hospital in Hialeah.
Dr. Arrangoiz joins an established surgical oncology office under the direction of Adrian Legaspi, MD, FACS, Medical Director of the Center for Advanced Surgical Oncology (CASO). Prior to joining the CASO practice, Dr. Arrangoiz worked as a breast, thyroid, parathyroid, and head and neck surgeon and served as Assistant Professor of Surgery, at the American British Cowdray Medical Center located in Mexico City, Mexico. For his education and training, Dr. Arrangoiz participated in an advanced two-year fellowship in head and neck surgery, and oncology from the International Federation of Head and Neck Oncology Societies and Memorial Sloan Kettering Cancer Center. Dr. Arrangoiz completed his complex surgical oncology/head and neck training at the Fox Chase Cancer Center (FCCC) located in Philadelphia, PA.
In addition to his fellowships, Dr. Arrangoiz finished a general surgery internship and residency where he was appointed chief resident at the Michigan State University Department of Surgery in Lansing, MI.
Dr. Arrangoiz received a grant from FCCC in order for him to complete his Master’s of Science in clinical research for health care professionals from Drexel University in Philadelphia. He graduated Summa Cum Laude from Anahuac University Medical School in Mexico City. Additionally, Dr. Arrangoiz completed his medical school internships with the National Institute of Perinatology, National Institute of Pediatrics’ in Mexico and at Jackson Memorial Hospital in Miami, FL.
Dr. Arrangoiz has published numerous scientific publications relating to oncology and surgery in peer-reviewed journals. He has written numerous abstracts on his surgical oncology research and presented his findings at surgical society meetings. Dr. Arrangoiz has presented as an invited lecturer at numerous international conferences and hospital grand rounds meetings on the topics of cancer and surgical treatments of cancer diseases.
Dr. Arrangoiz is a member of the American College of Surgeons, American Society of Breast Surgeons, American Society of Clinical Oncology, American Thyroid Association, American Head and Neck Society, the Society of Surgical Oncology, and the Association for Academic Surgery. He has been practicing medicine since 2002.
Mastalgia refers to breast pain and is a common presenting complaint among female patients:
Mastalgia is the most common symptom:
In patients undergoing breast imaging
It affects approximately:
70% of women
It is usually mild and self-limited but in:
Approximately 15% of affected women will require treatment
One study of almost 1700 women (mean age 34 years) surveyed by online questionnaire:
Found that over one-half (51.5%) had experienced breast pain:
Pain was more commonly reported among:
Older women
Those with larger breast sizes
Those less fit and / or physically active
In addition, of those who reported symptoms:
41% and 35% reported negative impacts from breast pain on their sexual health and sleep, respectively
10% of those symptomatic had reported breast pain as an issue for over half of their lives
It is classified in three categories:
Cyclic:
The level of pain can:
Vary according to the menstrual cycle:
Cyclical pain is associated with:
Hormonal fluctuations of the menstrual cycle
Cyclic breast pain:
Is the most common type:
Affecting two-thirds of patients with true mastalgia
Is more common in:
Premenopausal women in the 30s
It is usually:
Bilateral
It is more often felt:
In the upper outer quadrant
Its intensity increasesjust before menstruation and decreases after menstruation
It is thought to be caused by hormonal changes:
Therefore, most cases come in those actively menstruating or using HRT
Minor cyclical breast discomfort is normal:
It begins during the late luteal phase and dissipates with the onset of menses
This is usually bilateral and diffuse pain
Cyclical breast discomfort is caused by normal hormonal changes associated with ovulation:
That stimulate the proliferation of normal glandular breast tissue and result in pain
The stimulation of:
Ductal elements by estrogen
Stroma by progesterone
Stimulation of ductal secretion by prolactin:
All contribute to cyclical pain during the menstrual cycle
Cyclical breast pain can also be associated with pharmacologic hormonal agents:
Postmenopausal hormone therapy
Oral contraceptive pills
Non-cyclic:
It is not associated with the menstrual cycle
Noncyclical pain affects one-third of women with true mastalgia:
The pain does not follow the usual menstrual pattern:
May be constant or intermittent
Is more likely to be unilateral and variable in its location in the breast
Noncyclical breast pain is more likely to be related to:
A breast or chest wall lesion
Possible etiologies include:
Large pendulous breasts:
Large pendulous breasts may cause pain due to stretching of Cooper’s ligaments
Neck, back, and shoulder pain and headache may be present, as well as a rash under the pendulous breast in the inframammary fold
Diet, lifestyle:
The role of diet and lifestyle in causing breast pain is uncertain
Although a high-fat diet, smoking, and caffeine intake have been associated with breast pain:
It is difficult to conduct randomized trials with appropriate blinding that will negate the placebo effect:
Hence, there is currently no high-quality evidence to suggest that:
A low-fat diet, smoking cessation, or caffeine avoidance reduces breast pain
Hormone replacement therapy:
Up to one-third of menopausal women receiving postmenopausal hormone therapy experience some degree of noncyclical breast pain:
Which may spontaneously resolve over time
Breast cysts:
Solitary cysts:
Particularly when the presentation is abrupt:
Are frequently painful
Ductal ectasia:
Is characterized by distention of subareolar ducts due to inflammation unrelated to infection
Ductal ectasia may be associated with fever and acute local pain and tendernesscaused by:
Penetration of the duct wall by lipid material, which may resolve to leave a subareolar nodule:
In one study, the site and degree of duct dilatation correlated with the intensity of noncyclical breast pain
Mastitis:
Mastitis or breast abscess typically presents as:
A painful, swollen, and red breast in a febrile woman
Mastitis is more prevalent during lactation but can also occur in nonlactating women:
Idiopathic granulomatous mastitis [IGM]) or smokers
Inflammatory breast cancer:
Women with de novo inflammatory breast cancer (primary disease) may present with pain and a rapidly progressing tender, firm, enlarged breast
The skin over the breast is warm and thickened, with a “peau d’orange” (orange skin) appearance, but there is often no fever or leukocytosis
Hidradenitis suppurativa:
Although primarily confined to the axilla>
Can involve the breast and present as breast nodules and pain
Other:
Other etiologies of breast pain include:
Pregnancy
Thrombophlebitis (Mondor’s disease)
Trauma
Macrocysts
Prior breast surgery
Medications, including:
Oral contraceptives
Anti-depressants:
Such as sertraline
Antipsychotic drugs:
Such as haloperidol
Cardiovascular agents
Antibiotics
Is felt as pain related to the chest wall:
Rather than the breast itself
It is not associated with the menstrual cycle
It may be felt either:
Continuously or intermittently
It is rare as compared to the cyclic type:
Around a third of mastalgia is non-cyclical pain not unrelated to the menstrual cycle
It is found in women who are in their 40s
It is usually localized to one side and felt at a single area
Extramammary:
Some women who present with breast pain actually have referred pain from sources other than the breasts
The breast is innervated by the anterolateral and anteromedial branches of the intercostal nerves (T3 to T5):
Irritation of these nerves anywhere along their course can lead to pain that is felt in the breast or nipple
Women presenting with breast pain more often have extramammary painrather than true mastalgia
Extramammary pain may be from:
Musculoskeletal sources such as:
The chest wall, spinal or paraspinal disorders, trauma, or scarring from prior biopsy
It may also be related to medical problems such as:
Biliary, pulmonary, esophageal, or cardiac disease
Chest wall pain:
Is frequently due to pectoralis major muscle injury, related to repetitive activities such as water skiing, raking, rowing, or shoveling
Chest wall pain that presents as bilateral parasternal discomfort can also arise from costochondritis (typically the second through fifth costochondral junctions) or Tietze syndrome (typically the second and third costochondral junctions)
Other etiologies of chest wall pain include slipping and clicking ribs and arthritis
Spinal and paraspinal disorders:
Radicular chest wall pain may be due to cervical arthritis:
This pain typically occurs in older women in whom vertebral, spinal, and paraspinal problems in the neck and upper thorax accumulate with age
Paraspinal muscle spasm and other impingements on the free course of the sensory nerves from the neck and upper thorax can cause a radiculopathy leading to pain or hyperesthesia
Burning pain, which is typical of nerve root pressure, is a common feature
Imaging studies of the neck may reveal the etiology of the pain
Trauma:
Breast pain can be caused by local trauma, such as seat belt injury, child or pet kicking, or intimate partner violence, to the breasts or anterior chest wall
Pain can also be caused by intercostal neuralgia due to a respiratory infection or underlying pleuritic lesions:
Additionally, gallbladder disease or ischemic heart disease may present as intermittent chest pain attributed to the breast
Post-thoracotomy syndrome:
Is an unusual disorder in which a healing chest woundsimulates the effect of a suckling infant
It can be associated with an elevated prolactin concentration, breast pain, and milk production
A similar effect can be seen with other forms of chest wall irritation, including burns and chafing from clothing overlying the nipple
Pathophysiology of breast pain is not fully elucidated:
Etiologic factors:
High levels of serum fatty acid levels
Increase in basal prolactin levels
Excessive fatty diet
Psychological factors:
Are also shown to play a role in the etiology in some studies
A primary concern for patients with mastalgia:
Is that it is related to breast cancer:
However, the incidence of a breast malignancy associated with a presenting complaint of mastalgia is low:
A thorough assessment is required to determine the cause of the pain:
Explore any potential associated symptoms, and hopefully to reassure and manage their symptoms
It is rare for men to experience mastalgia:
However, it can occur in those who have developed:
Gynaecomastia
Clinical Features:
During the history and physical one should ask about specific features that could indicate a pathological cause of mastalgia, such as:
Lumps (breast nodules)
Skin changes:
Skin erythema
Skin dimpling (retraction)
Peu de orange
Nipple retraction
Nipple discharge
Fevers
Work-up:
Breast pain in isolation with no other relevant features on history or examination:
Is not an indication for imaging
All patients within reproductive age should have a pregnancy test
The American College of Radiology Appropriateness Criteria guidelines recommend the following approach to selecting an imaging modality:
Women with cyclical or bilateral non-focal breast pain usually do not require imaging:
The yield of finding a specific cause with imaging is low
Women with noncyclical, unilateral, or focal breast pain that is not extramammary (eg, chest wall pain), as determined by physical exam:
Should undergo breast imaging to elucidate the underlying etiology and exclude breast cancer
The choice of imaging modality is based on age:
Women under 30 years of age should undergo ultrasound because it is more accurate than mammography for that age group:
Mammography is added if abnormality is found on the ultrasound and / or if a patient’s history or risk status justifies the radiation exposure (eg, family history of premenopausal breast cancer)
Women between 30 and 39 years of age should also undergo ultrasound, and unilateral or bilateral mammography should also be performed because in this age group some small cancers are found on mammography but not ultrasound.
Women age 40 and older should undergo both mammography and ultrasound
Management:
Any underlying cause suspected should be investigated and managed as appropriate
However, in most cases the mastalgia pain will be idiopathic in nature and therefore reassurance and pain control, is the primary form of management
NICE guidelines states:
The management for cyclical breast pain should include:
Wearing a better fitting bra or soft-support bra during the night
The use of oral ibuprofen or paracetamol or topical NSAIDs can help alleviate pain
Non-cyclical pain does not usually respond well to treatment but in idiopathic cases will often resolve spontaneously
If first line management options are unsuccessful, a referral to a specialist may be warranted (breast surgeon)
Second line treatment for breast pain include:
The use of Danazol:
An anti-gonadotrophin agent:
Yet these can be accompanied with unpleasant side-effects:
Such as nausea, dizziness, and weight gain
References:
Mansel RE. Clinical Assessment of mastalgia. Br J Clin Pract Suppl 1989; 43: 17-9. Gateley CA, Holland PA. Drug therapy of mastalgia. What are the options? Drugs 1994; 48: 709-16.
Watt-Boolsen S, Eskildsen PC, Blaehr H. Release of prolactin, thyro- tropin and growth hormone in women with cyclical mastalgia and fibrocystic disease of the breast. Cancer 1985; 56: 500-2. Seema A. Khan, A. Vania Apkarian. Mastalgia and breast cancer: a protective association? Cancer Detection and Prevention 2002; 26: 192-6.
Fox H, Walker LG, Heys SD, Ah-See AK, Eremin O. Are patients with mastalgia anxious, and does relaxation therapy help? The Breast 1997; 6: 138-42. Preece PE, Baum M, Mansel RE, Webster DJ, Fortt RW, Gravelle IH, et al. Importance of mastalgia in operable breast cancer. Br Med J (Clin Res Ed) 1982; 284: 1299-300.
Plu-Bureau G, Thalabard JC, Sitruk-Ware R, Asselain B, Mauvais-Jar- vis P. Cyclical mastalgia as a marker of breast cancer susceptibility: results of a case-control study among French women. Br J Cancer 1992; 65: 945-9.
Aksu G, Hocaoğlu Ç. Evaluation of Anxiety, Alexytimia and Depres- sion levels in patients undergoing Radiologic Evaluation for Mas- talgia. Klinik Psikiyatri 2004; 7: 95-102
If you’re having thyroid surgery, it’s important to know how to best prepare for your procedure and what to expect while you recover. This includes any tests you’ll need before surgery, as well as what to avoid after surgery to help ensure its success.
How should I prepare for thyroid surgery?
After your thyroidectomy or thyroid lobectomy is scheduled, you’ll have a pre-operative evaluation with members of your thyroid surgery care team. That evaluation may include blood tests, an electrocardiogram (EKG), X-rays or other imaging studies.
We’ll give you specific instructions on when to stop eating, drinking and taking medications prior to surgery. It’s very important that you follow these guidelines for your own safety, and you’ll need to have an empty stomach before any surgical procedure that requires anesthesia. If you don’t follow the instructions, your thyroid surgery might be cancelled. Please contact us with any specific questions.
What is recovery like after thyroid surgery?
After your thyroidectomy or thyroid lobectomy, you may have a temporary sore throat, neck pain, difficulty swallowing or a weak voice.
Your diet will be restricted for the evening of your surgery, but in most cases, it can return to normal the next day.
Before you leave the hospital, we’ll schedule a follow-up appointment, give instructions for your at-home recovery and go over any prescribed medications.
Most people are ready to return home within one day of surgery, but take off about two weeks from work to recover. You’ll need to refrain from heavy lifting or other tasks that can strain your neck for up to three weeks after your surgery. Soaking or scrubbing the site of your incision is also discouraged for at least one week to allow it time to properly heal. Showering is generally allowed after about one day.
Pain at the site of your incision will improve after a few days but may continue for a week or so. If you notice sudden swelling in your neck, which could signify an infection, contact our office.
Due to disturbance of the parathyroid glands, which regulate calcium balance, your calcium level may drop after surgery. If it drops, you may notice numbness and tingling of your fingers or around your mouth. We’ll monitor your calcium levels through blood tests, and give you instructions about taking calcium replacements if needed.
What are the side effects of thyroid surgery?
After a total thyroidectomy, you will take lifelong thyroid hormone replacements. Because your entire thyroid gland is removed, it will no longer supply you with the hormone you need to control your body’s metabolic processes. You might also have to take supplements after thyroidectomy to balance your calcium levels.
After a thyroid lobectomy, you’ll need to have your thyroid hormone levels checked and will be prescribed a thyroid hormone replacement, if needed.
In the weeks after your thyroid surgery, you may have neck pain, soreness of your vocal chords or a weak voice. These symptoms are usually temporary.
Will I need to follow a special diet after thyroid surgery?
For most people, a special diet after a thyroidectomy or thyroid lobectomy isn’t necessary. You’ll likely be able to eat and drink normally the morning after your surgery, but you may prefer softer foods at first. We’ll let you know if and for how long you need to restrict your eating and drinking.