My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
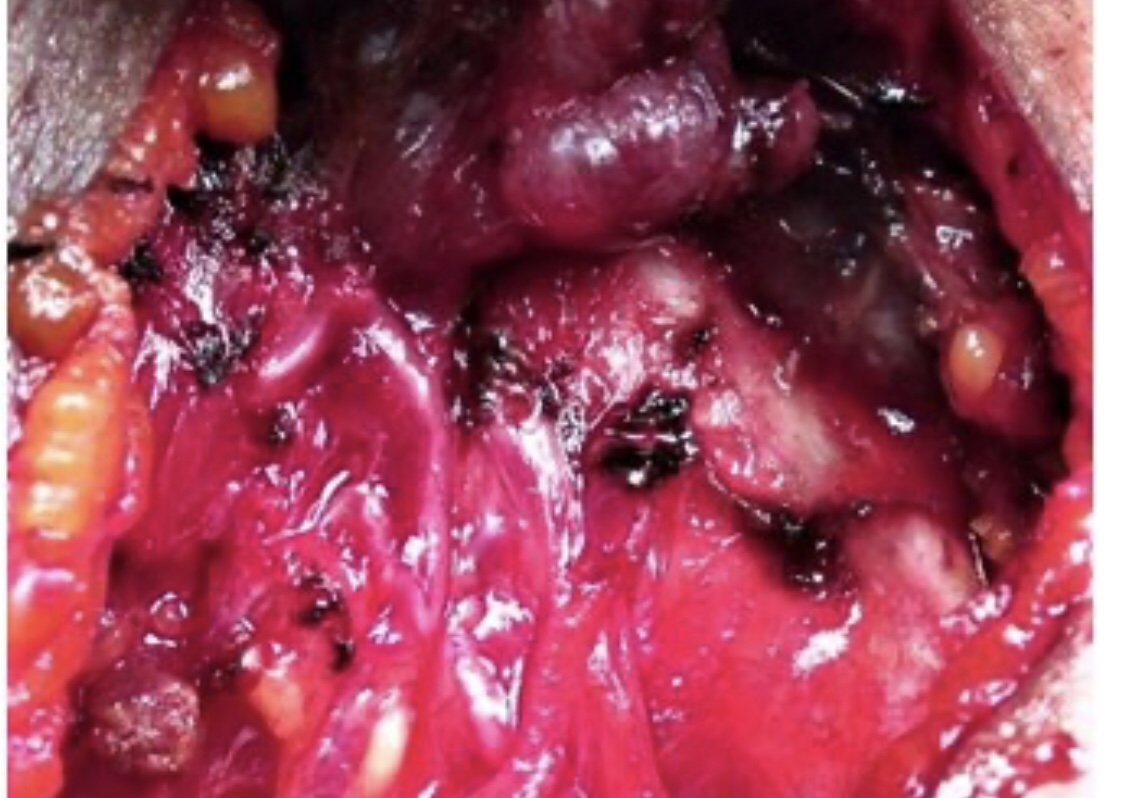
An extreme form of parathyroid bone disease termed osteitis fibrosa cystica is characterized by significant loss of bone density, development of bone cysts and brown tumors (shown below), skeletal deformity, bone pain, and a propensity for pathologic fractures. Fortunately, it is quite rarely seen these days.
Overweight or obesity (particularly in postmenopausal women)
White race or Ashkenazi Jewish descent
Medical history:
BRCA1 or BRCA2 mutation
First-degree relative with breast or ovarian cancer
History of atypical hyperplasia or lobular carcinoma in situ
One prior breast biopsy (regardless of results)
Personal history of breast or ovarian cancer
Medications and diet:
Alcohol consumption (more than one drink per day)
Current or prior use of hormone therapy or oral contraceptives
Reproductive history:
Menarche before 12 years of age Menopause after 55 years of age Nulliparity or age older than 35 years at first delivery Other High breast density on mammography Prior thoracic radiation exposure
The ACS updated its guidelines for breast cancer screening in average-risk women in October 2015. At this time, the ACS is in the process of updating the breast cancer screening guidelines for women at high risk, which were last updated in 2007.
Beginning in their early 20s, women should be told about the benefits and limitations of breast self exam (BSE).
The ACS does not recommend clinical breast examination for breast cancer screening in average-risk women at any age.
ACS recommendations are as follows:
Women should begin regular screening mammography at age 45 years (strong recommendation)
Women aged 45 to 54 years should be screened annually (qualified recommendation)
Women 55 years and older should transition to biennial screening or have the opportunity to continue screening annually (qualified recommendation):
Women should have the opportunity to begin annual screening at 40 to 44 years of age (qualified recommendation)
Women should continue screening mammography as long as their overall health is good and they have a life expectancy of 10 years or longer (qualified recommendation)
The ACS recommends annual MRI screening along with mammography, based on evidence from non-randomized screening trials and observational studies, in women with the following risk factors:
BRCA mutation
First-degree relative of BRCA carrier, but untested
Lifetime risk ∼20–25% or greater, as defined by BRCAPRO or other models that are largely dependent on family history
The ACS recommends annual MRI screening, based on expert consensus opinion that considers evidence of lifetime risk for breast cancer, in women with the following risk factors:
Radiation to chest between age 10 and 30 years
Li-Fraumeni syndrome or first-degree relatives with the syndrome
Cowden and Bannayan-Riley-Ruvalcaba syndromes or first-degree relatives with those syndromes
#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOncologist # CASO #CenterforAdvancedSurgicalOncology
An estimated 2.1 million women were newly diagnosed with breast cancer:
Approximately one new case diagnosed every 18 seconds
Additionally, 626,679 women with breast cancer died
The global incidence of breast cancer:
Has been rising:
With annual increases of 3.1%:
Beginning with 641,000 cases in 1980 and increasing to greater than 1.6 million in 2010:
This trend is likely to continue
Indeed, the global cancer burden in women:
Is increasing in countries regardless of income level:
Owing to population growth and an aging population
The female population:
Accounts for 49.5% of the global population:
They form a larger proportion of the population > 60 years of age
Furthermore, the epidemiology of advanced breast cancer is a research priority as, in most countries:
The number of patients with advanced disease is unknown
Cancer registries mostly track diagnosis and deaths but not relapses
One study estimated that, in 2017:
~160,000 patients live with advanced-stage breast cancer in the United States alone5
The death rates also vary among subtypes of breast cancer:
With HER2-positive disease:
Associated with a higher death rate:
Followed by the TNBC, luminal A and luminal B subtypes
Incidence varies worldwide:
With higher incidence in high-income regions (92 per 100,000 in North America) than in lower income regions (27 per 100,000 in middle Africa and eastern Asia):
These patterns reflect both:
The risk factors and the availability and utility of mammography (and, therefore, detected breast cancers)
The highest breast cancer incidence is in:
North America
Australia
New Zealand
Northern and western Europe
Furthermore, in high-income countries:
Breast cancer is often diagnosed at an early stage and the prognosis is usually good
However, in low- and middle- income countries:
Breast cancer is often diagnosed at a later stage:
And is accordingly, associated with poorer survival:
A fact that is reflected in the mortality statistics
Breast cancer mortality is usually higher in many low- and middle-income countries:
Such as those in sub-Saharan Africa and developing Asian countries:
Despite their lower incidence:
Due to delayed presentation, late stage at diagnosis and limited access to treatment
Several studies have also shown that breast cancer presents:
Earlier in Asian women (typically 40 to 50 years of age) than in their western counterparts (typically 60 to 70 years of age)
In addition, patients in developing countries who are diagnosed with breast cancer:
Are roughly 10 years younger than those in developed countries:
The proportion of young patients ( less than 35 years of age) varies from:
~10% in developed countries to up to 25% in developing Asian countries
The biology of the tumor also varies by ethnicity:
Which has implications for the difference in mortality:
African and African-American women:
Have the highest rates of TNBC compared with any other ethnic group
They also had higher rates of metastatic disease
They have the highest rates of poorly differentiated or undifferentiated grade among all subtypes:
All of which are associated with lower survival
Additionally, metastatic breast cancer represents 9% of diagnoses among non-Hispanic black women:
Compared with 5% to 6% of diagnoses in other ethnic groups
Regarding the survival gains in patients with advanced disease during the years 1975 to 2013:
The 5-year cause-specific survival of non-Hispanic white women was higher than that of other ethnic groups:
Particularly non-Hispanic black women (19% to 37% com- pared with 16% to 26%):
This pattern is multifactorial and involves genetic predisposition, lifestyle and other environmental factors
References:
Bray, F. et al. Cancer Incidence in Five Continents: inclusion criteria, highlights from Volume X and the global status of cancer registration. Int. J. Cancer 137, 2060–2071 (2015).
Mariotto, A. B., Etzioni, R., Hurlbert, M., Penberthy, L. & Mayer, M. Estimation of the number of women living with metastatic breast cancer in the United States. Cancer Epidemiol. Biomark. Prev. 26, 809–815 (2017).
Ren, J.-X., Gong, Y., Ling, H., Hu, X. & Shao, Z.-M. Racial/ethnic differences in the outcomes of patients with metastatic breast cancer: contributions of demographic, socioeconomic, tumor and metastatic characteristics. Breast Cancer Res. Treat. 173, 225–237 (2019).
Torre, L. A., Siegel, R. L., Ward, E. M. & Jemal, A. Global cancer incidence and mortality rates and trends — an update. Cancer Epidemiol. Biomark. Prev. 25, 16–27 (2016).
Ginsburg, O. et al. The global burden of women’s cancers: a grand challenge in global health. Lancet 389, 847–860 (2017).
Allemani, C. et al. Global surveillance of cancer survival 1995–2009: analysis of individual data for 25 676 887 patients from 279 population-based registries in 67 countries (CONCORD-2). Lancet 385, 977–1010 (2015).
Winters, S., Martin, C., Murphy, D. & Shokar, N. K. Breast cancer epidemiology, prevention, and screening. Prog. Mol. Biol. Transl Sci. 151, 1–32 (2017).
Hossain, M. S., Ferdous, S. & Karim-Kos, H. E. Breast cancer in South. Asia: a Bangladeshi perspective. Cancer Epidemiol. 38, 465–470 (2014).
Leong, S. P. L. et al. Is breast cancer the same disease in Asian and western countries? World J. Surg. 34, 2308–2324 (2010).
Bhoo Pathy, N. et al. Breast cancer in a multi-ethnic Asian setting: results from the Singapore–Malaysia hospital-based breast cancer registry. Breast 20, S75–S80 (2011).
Raina, V. et al. Clinical features and prognostic factors of early breast cancer at a major cancer center in North India. Indian J. Cancer 42, 40 (2005).
Agarwal, G., Pradeep, P. V., Aggarwal, V., Yip, C.-H. & Cheung, P. S. Y. Spectrum of breast cancer in Asian women. World J. Surg. 31, 1031–1040 (2007).
Li, C. I., Malone, K. E. & Daling, J. R. Differences in breast cancer hormone receptor status and histology by race and ethnicity among women 50 years of age and older. Cancer Epidemiol. Biomark. Prev. 11, 601–607 (2002).
Wong, F. Y., Tham, W. Y., Nei, W. L., Lim, C. & Miao, H. Age exerts a continuous effect in the outcomes of Asian breast cancer patients treated with breast- conserving therapy. Cancer Commun. 38, 39 (2018).
Kohler, B. A. et al. Annual report to the nation on the status of cancer, 1975–2011, featuring incidence of breast cancer subtypes by race/ethnicity, poverty, and state. J. Natl Cancer Inst. 107, https://doi.org/ 10.1093/jnci/djv048 (2015).
DeSantis, C. E. et al. Breast cancer statistics, 2015: Convergence of incidence rates between black and white women: Breast Cancer Statistics, 2015.
CA Cancer J. Clin. 66, 31–42 (2016).
DeSantis, C. E., Ma, J., Goding Sauer, A., Newman, L. A. & Jemal, A. Breast cancer statistics, 2017, racial disparity in mortality by state: Breast Cancer Statistics, 2017. CA Cancer J. Clin. 67, 439–448 (2017).
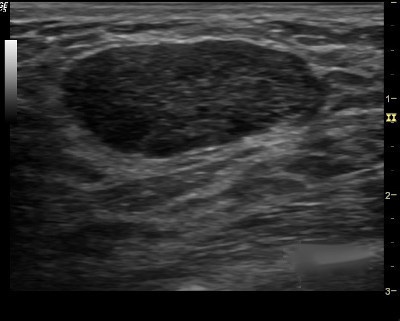
1. You first evaluate the lesion for any of the 10 malignant signs:
Shadowing
Hypoechoic echotexture
Spiculation
Angular margins
Thick echogenic capsule
Taller than wider
Microlobulation
Duct extension
Branching pattern
Calcifications
2. Finding none, you move on to the second step in the evaluation process and specifically look for one of the three strictly defined benign signs, and if any of them is found, the lesion can be considered BI-RADS 3.
3. The three benign findings defined by Stavros are:
A purely hyperechoic lesion with no hypoechoic area larger than a normal duct or lobule.
Elliptical, wider than tall, well-circumscribed and thin echogenic capsule.
Gently lobulated, wider than tall, well-circumscribed and thin echogenic capsule.
– Combining the elliptical or gently lobulated shapes with the presence of a complete, thin echogenic capsule is necessary because many circumscribed carcinomas and most ductal carcinoma in situ are encompassed in a thin, echogenic capsule.
Ultrasound is safe and painless. It produces pictures of the inside of the body using sound waves. Ultrasound imaging is also called ultrasound scanning or sonography. It uses a small probe called a transducer and gel placed directly on the skin. High-frequency sound waves travel from the probe through the gel into the body. The probe collects the sounds that bounce back. A computer uses those sound waves to create an image. Ultrasound exams do not use radiation (as used in x-rays). Because images are captured in real-time, they can show the structure and movement of the body’s internal organs. They can also show blood flowing through blood vessels.
Ultrasound imaging is a noninvasive medical test that helps physicians diagnose and treat medical conditions.
Doppler ultrasound is a special ultrasound technique that evaluates movement of materials in the body. It allows the doctor to see and evaluate blood flow through arteries and veins in the body.
Ultrasound imaging of the breast produces a picture of the internal structures of the breast.
During a breast ultrasound examination, the sonographer or physician performing the test may use Doppler techniques to evaluate blood flow or lack of flow in any breast mass. In some cases, this may provide additional information as to the cause of the mass.
What are some common uses of the procedure?
Determining the Nature of a Breast Abnormality The primary use of breast ultrasound is to help diagnose breast abnormalities detected by a physician during a physical exam (such as a lump) and to characterize potential abnormalities seen on mammography or breast magnetic resonance imaging (MRI).
Ultrasound imaging can help to determine if an abnormality is solid (which may be a non-cancerous lump of tissue or a cancerous tumor), fluid-filled (such as a benign cyst) or both cystic and solid.
Doppler ultrasound is used to assess blood supply in breast lesions.
Supplemental Breast Cancer Screening Mammography is the only screening tool for breast cancer that is known to reduce deaths due to breast cancer through early detection. Even so, mammograms do not detect all breast cancers. Some breast lesions and abnormalities are not visible or are difficult to interpret on mammograms. Breasts that are considered dense have a lot of glandular and connective tissues and not much fatty tissue, and that makes cancer harder to detect.
Many studies have shown that ultrasound and magnetic resonance imaging (MRI) can help supplement mammography by detecting breast cancers that may not be visible with mammography. Your doctor can help you determine if either of these tests is appropriate for you. MRI is more sensitive than ultrasound in depicting breast cancer, but MRI may not be available to all women. If screening MRI is performed, then screening ultrasound is not needed, though ultrasound may be used to characterize and biopsy abnormalities seen on MRI. When ultrasound is used for screening, abnormalities not visible with mammography may be identified, including some that may require biopsy. Many of the abnormalities found with screening breast ultrasound are not cancer (false positives).
Ultrasound can be offered as a screening tool for women who:
are at high risk for breast cancer and unable to undergo an MRI examination.
are pregnant or should not be exposed to x-rays (which are necessary for a mammogram).
have increased breast density — when the breasts have a lot of glandular and connective tissue and not much fatty tissue (see the Dense Breasts page for more information).
Ultrasound-guided Breast Biopsy When an ultrasound examination reveals a suspicious breast abnormality, a physician may choose to perform an ultrasound-guided biopsy. Because ultrasound provides real-time images, it is often used to guide biopsy procedures. An ultrasound exam will usually need to be performed before the biopsy in order to plan the procedure and to determine if this method of biopsy can be used
👉We define dense breasts as an indicator of the amount of glandular and connective tissue, meaning the tissue responsible for making milk and holding the breast in place and up, for lack of a better description.
👉It’s not determined by how firm the breasts feel. A lot of times patients will come in and say, “My breasts feels so dense.” That is not density.
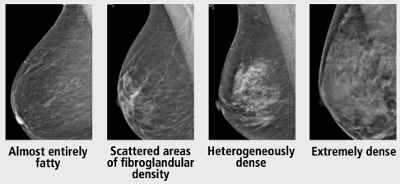
👉Density is categorized using a standardized system that was developed by the American College of Radiology that’s called the BI-RADS system.
👉We categorize breast density in four ways. One, breast can be completely fatty. That means it’s all fat. We don’t have any glandular tissue in the breast. Or scattered, meaning 25% to 50% density. Heterogeneously dense is 50% to 75% density, and extremely dense means there’s way more glandular tissue than there is fat.
👉Dense breasts are common. About 40% to 45% of US women between the ages of 40 and 74 have dense breast tissue. So it’s important because the risk of breast cancer increases with increasing breast density.
👉Women with dense breast tissue have a one and a half to two fold increase in risk compared to those with less dense breast tissue.
👉The other problem with it is dense breast tissue is white on a mammogram, and breast cancer is white on a mammogram, and so a lot of times the denser tissue can obscure or hide a cancer on the mammogram and making it harder for a radiologist to pick that up.
👉In 2019, the FDA issued a rule requiring all mammogram reports to include information about breast density so that women can have that conversation with their doctors about whether or not additional screening modalities or screening tests should be performed for that particular patient.
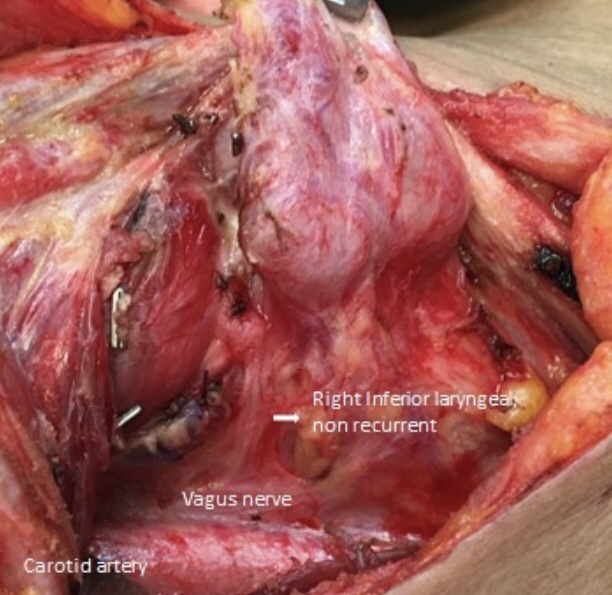
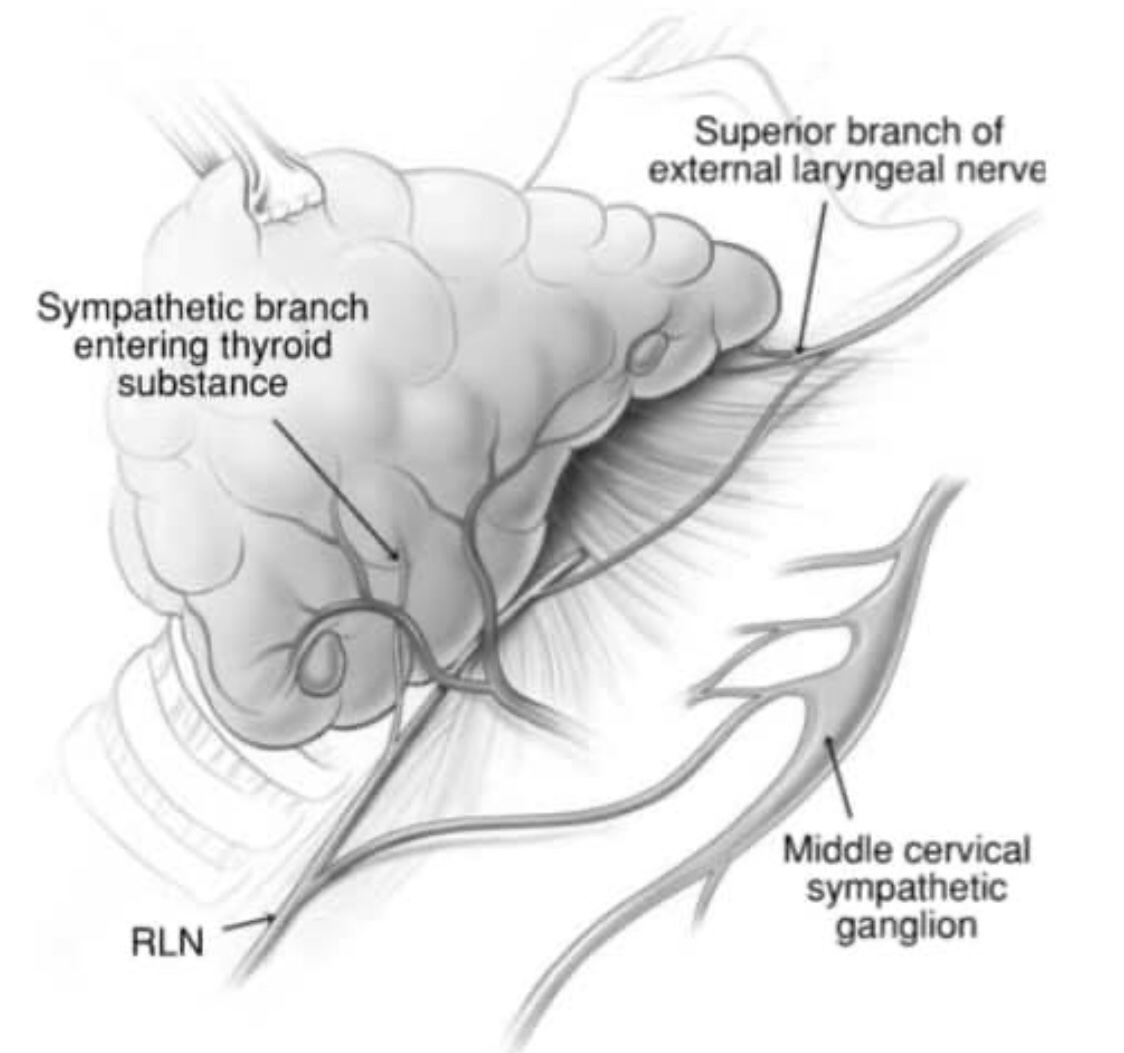
👉Although occasional direct connections between cervical sympathetic ganglia and the RLN (sympathetic-inferior laryngeal nerve anastomotic branch or SILAB) have been well described, it is now appreciated that very fine direct anastomoses from the sympathetic ganglia to both the RLN as well as the external branch of the superior laryngeal nerve (EBSLN), and then on to the substance of the thyroid gland, are very common if not universal.
👉It has been reported that up to 2% of SILAB are larger than the RLN and may thus be mistaken for a non-recurrent laryngeal nerve, thus placing the true RLN at risk of division.
👉If there is any doubt about the nature of apparent anastamotic branches they should be traced back laterally.
👉A non- recurrent laryngeal nerve will arise from the vagus whereas a SILAB will usually arise from the middle cervical ganglion, or occasionally from the inferior or superior ganglia.
👉Occasionally a sympathetic branch from the superior cervical ganglion, hitch-hikes along the EBLN and then communicates via a further branch to the RLN along with the ‘nerve of Galen’, although this nerve itself is thought to contain primarily sensory and some motor fibers.
👉Branches also leave the RLN passing directly into the substance of the thyroid gland.
👉While any such branch appearing to pass into the thyroid should be carefully examined in order to avoid dividing a small true anterior branch of the RLN, recognition of the existence of sympathetic anastamoses is vital during thyroid dissection.
👉Malignant neoplasm of the tongue are by far more common in men than in women (66-95% of cases), this is similar to the rest of the oral cavity .
👉The incidence by gender varies depending on the anatomic location and has been changing due to the increase in the number of women who smoke. The male to female ratio is currently 3:1.
👉The incidence of oral cavity and tongue cancer increases with age, especially after age 50. Most patients are between 50 and 70 years but can also occur in younger patients.
👉There are large differences in the incidence of oral cavity cancer among different geographical regions.
👉The highest incidence of this disease is found in Asia and is believed to reflect the prevalence of certain risk factors, such as chewing betel nut and the use of smokeless tobacco (snuff).
👉In the United States, in urban areas the high incidence among men is thought to reflect exposure to snuff and alcohol. Among women in rural areas in the United States the increase risk of oral cavity cancer is associated with the use of smokeless tobacco (snuff)