My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
Three important conclusions are agreed upon regarding this clinical entity:
Prognosis of occult primary breast cancer is the same or slightly better than women with classic stage IIA disease (T0, N1, M0)
An exhaustive workup for the non-breast primary is usually not fruitful
Treatment of the breast in some manner decreases the risk of local failure over time
Occult primary breast cancer was first recognized by William Halsted:
Who described three patients presenting with axillary tumors that were eventually found to represent breast cancer
In modern series:
Occult breast cancer accounts for 0.1% to 0.8% of all newly diagnosed breast cancers:
The incidence has not decreased with improvements in breast imaging
Differential diagnosis:
In general:
Palpable axillary nodes are more often related to benign rather than malignant disorders:
However, when cancer is identified:
The most common tumor causing axillary lymphadenopathy is:
Breast cancer
In several series:
The incidence of breast cancer in mixed populations of men and women with metastatic axillary adenopathy:
Is 50% or higher:
The vast majority are women:
Although occult primary breast cancer has been reported in men:
It is very rare
Other neoplasms that may present with axillary nodal involvement are:
Lymphomas
Melanomas
Sarcomas
Thyroid cancers
Skin cancers
Lung cancers
Less often:
Uterine, ovarian, sweat gland, or gastric cancers
In approximately 30% of cases:
The primary site is never identified
Initial Diagnostic Workup:
Biopsy:
The first step in the diagnostic workup of a patient with unexplained axillary adenopathy is:
A biopsy
Besides standard light microscopic examination of hematoxylin and eosin-stained sections:
Other techniques such as:
Immunohistochemistry and sometimes electron microscopy can help to narrow the differential diagnosis
Immunohistochemistry:
The pathologic examination of a biopsy specimen for an isolated axillary lymph node metastatic adenocarcinoma or poorly differentiated carcinoma in a woman should include immunohistochemical staining for the following markers:
Carcinoembryonic antigen (CEA)
Cytokeratins 7 and 20
Estrogen receptor (ER) and progesterone receptor (PR)
Gross cystic disease fluid protein-15:
GCDFP-15:
Is identified by staining with the monoclonal antibody BRST2
Mammaglobin
Thyroid transcription factor (TTF-1)
CA125
Men:
Should have routine staining for prostate cancer markers as well
While none of these markers is sufficiently sensitive or specific to be used alone, certain patterns of expression favor the diagnosis of an occult breast cancer:
Positive staining for:
CEA, CK7, ER/PR, mammaglobin, CA125, and BRST2
Negative staining for:
CK20 and TTF-1
CEA is a sensitive marker for:
Adenocarcinomas of the breast, lung, and gastrointestinal tract:
But does not help to distinguish among these sites of origin
On the other hand, differential expression of cytokeratins (CKs) can assist in this differentiation:
CK20 is a low molecular weight cytokeratin:
That is normally expressed in the gastrointestinal epithelium, urothelium, and in Merkel cells
CK7 is expressed by tumors of the:
Lung, ovary, endometrium, and breast:
Not in the lower gastrointestinal tract
The pattern of CK20 and CK7 may be particularly helpful in suggesting a primary site:
The presence of CK7 and absence of CK20:
Favors a diagnosis of breast cancer
TTF-1:
Is rarely positive in breast cancers:
While it is positive in 70% to 80% of non-squamous cancers arising in the lung
CA-125:
Is commonly positive in ovarian carcinomas:
But is positive in about 10% of breast cancers
ER/PR:
Its presence in an axillary node, particularly in conjunction with other compatible IHC findings:
Lends support to a diagnosis of an occult breast primary
Although positive staining for ER and/or PR supports a possible diagnosis of breast cancer:
These markers are nonspecific and they may also be expressed in:
Ovarian, uterine, lung, stomach, thyroid, and hepatobiliary cancers:
However:
ER/PR staining of an axillary node is compelling evidence of a primary breast cancer
Other breast cancer-specific IHC stains are:;
BRST2 (for GCDFP) and mammaglobin:
BRST2 is positive in 65% to 80% of cases:
Is relatively specific for breast cancer:
Rarely, it is positive in:
Skin adnexal tumors, endometrial cancers, and salivary gland tumors
While mammaglobin is more sensitive, it is less specific for breast cancer:
Gynecologic, lung, urothelial, thyroid, colon and hepatobiliary tumors may stain positive:
Both stains are thus typically used together
HER2 immunostaining:
Is not generally useful for the differential diagnosis of a carcinoma arising in the axillary nodes as it lacks specificity:
Furthermore, only 18% to 20% of breast cancers overexpress this protein:
However, assay for HER2 overexpression by IHC or fluorescent in situ hybridization (FISH) is a routine component of the evaluation of all breast cancers:
As it permits the identification of those women who are most likely to respond to treatments targeting HER2 (eg, the therapeutic monoclonal antibody trastuzumab)
Modified radical mastectomy has been the traditional surgical treatment for many years
Previously, the primary breast cancer was found in the mastectomy specimen:
40% to 80% of the time, but with the advent of much better mammography and ultrasound along with breast MRI, this rate is much lower now
However, what was true then and still holds today:
Is that no treatment to the breast itself results in an unacceptably high local recurrence rate
An alternative to a modified radical mastectomy:
Is complete ALND followed by whole-breast irradiation
Axillary dissection:
Provides local control while also fine tuning staging
Theoretically the whole-breast radiation:
Should control any subclinical disease in the breast not detected on imaging
Primary radiation to the breast, axilla, and supraclavicular area without any surgery of the breast or axilla:
Results in higher local and regional recurrence compared to surgery and radiation combined
Axillary node dissection and whole-breast irradiation:
Has been found to have equivalent survival as a modified radical mastectomy
A recent meta-analysis of seven studies and more than 240 patients with occult primary breast cancers (0.3% to 0.8% of all breast cancers):
Found 39% were treated with ALND and radiation while 47% had modified radical mastectomy and 15% had ALND alone
With a mean follow-up of 5 years:
The study found no difference in local regional recurrence (12.7% vs 9.8%), distant metastasis (7.2% vs 12.7%), or mortality (9.5% vs 17.9%) between ALND and radiation vs modified radical mastectomy (all p>0.16)
ALND with radiation was superior to ALND alone in terms of local regional recurrence (12.7% vs 34.3%, p < 0.01) and trended towards improved survival but this was not statistically significant (P=0.09)
References:
Barton SR, Smith IE, Kirby AM, Ashley S, Walsh G, Parton M. The role of ipsilateral breast radiotherapy in management of occult primary breast cancer presenting as axillary lymphadenopathy. Eur J Cancer. 2011;47:2099-2106. PMID: 21658935. http://www.ncbi.nlm.nih.gov/pubmed/21658935
Macedo FI, Eid JJ, Flynn J, Jacobs MJ, Mittal VK. Optimal surgical management for occult breast carcinoma: a meta-analysis. Ann Surg Oncol. 2016;23:1838-1844. https://www.ncbi.nlm.nih.gov/pubmed/26832884
Rueth NM, Black DM, Limmer AR, et al. Breast conservation in the setting of contemporary multimodality treatment provides excellent outcomes for patients with occult primary breast cancer. Ann Surg Oncol. 2015;22:90-95. [epub ahead of print]. http://www.ncbi.nlm.nih.gov/pubmed/25249256
Walker GV, Smith GL, Perkins GH, et al. Population-based analysis of occult primary breast cancer with axillary lymph node metastasis. Cancer. 2010;116:4000-4006. PMID: 20564117. http://www.ncbi.nlm.nih.gov/pubmed/20564117
Woo SM, Son BH, Lee JW, et al. Survival outcomes of different treatment methods for the ipsilateral breast of occult breast cancer patients with axillary lymph node metastasis: a single center experience. J Breast Cancer. 2013;16:410-416. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3893343/
Most commonly, this tumor is a result of lymphedema induced by radical mastectomy to treat breast cancer:
Unfortunately, although the breast cancer may be cured with such radical surgery:
This second primary cancer may be responsible for the patient’s worsening course.
The term Stewart-Treves syndrome is broadly applied to an angiosarcoma that arises in a chronically lymphedematous region due to any cause, including:
Congenital lymphedema and other causes of secondary lymphedema unassociated with mastectomy
As reported by Durr et al in 2004, this lymphangiosarcoma occurs as a rare complication:
Lymphangiosarcoma is a misnomer because this malignancy seems to arise from blood vessels instead of lymphatic vessels:
A more appropriate name is hemangiosarcoma
In 1906, Lowenstein first described angiosarcoma:
In a patient’s arm that had been affected by severe posttraumatic lymphedema for 5 years
In 1948, Stewart and Treves reported this rare secondary malignancy in six cases of angiosarcoma in postmastectomy lymphedema:
They recognized that an edematous arm after radical mastectomy for breast cancer may suggest recurrent breast cancer:
But that long-standing chronic edema without recurrent cancer may occasionally produce “a heretofore unrecognized and unreported sequel … long after the malignant breast neoplasm has apparently been arrested … a new specific tumor”
Stewart and Treves suggested that these angiosarcomas were probably not observed previously because they were mistaken for recurrent, inoperable, cutaneous manifestations of breast cancer
Clinical suspicion should be high:
As this syndrome is easily misdiagnosed and treatment is advertently delayed
Pathophysiology:
The pathogenic mechanism by which lymphedema may induce angiosarcoma has been the subject of controversy
Stewart and Treves found a high incidence of third malignancies in patients with postmastectomy angiosarcoma:
Thus, they speculated that a systemic carcinogenic factor was the main causative factor in the pathogenesis of lymphangiosarcomas.
In 1979, Schreiber and others postulated the concept of local immunodeficiency in the presence of lymphedema:
This theory is supported by experimental evidence:
In 1960, Stark and associates demonstrated that homograft skin transplanted to lymphedematous arms survive much longer than those transplanted to healthy arms:
Therefore, lymphedema may cause some degree of local immunodeficiency and lead to oncogenesis
The possibility that radiation therapy has an important role in the induction of lymphangiosarcoma is also postulated:
Sternby et al reported that in their study:
The patient with the shortest interval between radical mastectomy and the onset of the tumor (8 months) received both preoperative radiation therapy of the breast and involved axillary lymph nodes followed by fractionated radiation
Others suggest that irradiation is not an essential factor in the pathogenesis of this tumor
Finally, irradiation may be an indirect cause of lymphangiosarcomas because it may cause axillary node sclerosis and thereby accelerate and aggravate the edema
Clinical data from Swedish women with previous breast cancer who developed angiosarcomas / lymphangiosarcomas on the thoracic wall / upper extremity between 1958 and 2008:
Showed 31 angiosarcomas developed at a median age of 71 years
The 14 women treated for breast cancer with radical mastectomy and radiotherapy from 1949 to 1988 developed angiosarcomas in edematous arms after a median 11 years
Whereas 17 females treated by segmental resection, antihormonal treatment, and radiotherapy from 1980 to 2005 developed angiosarcomas in the irradiated field on the thoracic wall after a median 7.3 years
Epidemiology:
Frequency:
Currently, approximately 400 cases of Stewart-Treves syndrome are reported in the world literature
In 1962, Schirger calculated that the incidence of this disease is 0.45% in patients who survive at least 5 years after radical mastectomy
Another analysis calculated it as occurring in 0.03% of patients surviving 10 or more years after radical mastectomy:
As a result of the increase in conservative treatment for breast carcinoma and improvement of operative and radiation therapy techniques:
The prevalence of Stewart-Treves syndrome has decreased
Race:
No racial predominance exists for Stewart-Treves syndrome
Gender:
Most patients with Stewart-Treves syndrome are women with a history of breast cancer that has been treated with radical mastectomy:
Which causes chronic lymphedema
Age:
Stewart-Treves syndrome usually occurs in middle-aged or elderly women, a few years or many years after mastectomy:
In 1981, Sordillo and associates reported a peak incidence in persons aged 65 to 70 years
In 1972, Woodward et al described a series of 23 patients in a review of 163 cases of Stewart-Treves syndrome from the literature:
They recorded an average patient age of 68.8 years at the onset of lymphangiosarcoma:
The youngest patient was aged 44 years and the oldest, 84 years
Once diagnosed:
Surgical excision is the treatment of choice, sometimes requiring forequarter amputation
Early amputation or wide local excision provides the best chance of long-term survival in patients with Stewart-Treves syndrome
Some authorities favor radical ablative surgery with an early diagnosis, in order to confer a reasonable prognosis with this rare but aggressive disease
A nihilistic approach is undesirable
The most common approach in patients with lymphangiosarcoma is amputation of the limb or forequarter rather than wide local surgical excision
Even in cases with early surgical treatment, the prognosis is disappointing, with a high rate of local recurrence and metastasis
Metastatic disease should exclude surgical treatment unless surgery is useful for symptomatic improvement
Chemotherapy may have some role:
However its benefit is unclear
Chemotherapy and irradiation continue to be evaluated as adjuvants to surgery for the treatment of Stewart-Treves syndrome:
Currently, these treatment options offer little benefit
Multiple studies have shown the 5-year survival to be very poor:
At less than 10%
The mean survival is 20 months
Multimodal therapy including:
Hyperthermic isolated limb perfusion with tumor necrosis factor-alpha and melphalan, combined with radical resection of the affected skin and subcutaneous tissue including the fascia, with large safety margins, may provide enhanced survival
In 2000, Grobmyer and associates found no statistical significant difference in the survival rates of patients treated with chemotherapy compared with those treated with irradiation:
Although long-term survivors after either radiation therapy or systemic chemotherapy have been reported:
The overall results have been discouraging
A questionable response to weekly paclitaxel has been described:
As a result of these findings, these treatment options are reserved for patients with inoperable, advanced disease or those who refuse surgery
Intra-arterial mitoxantrone / paclitaxel was used for angiosarcoma of the lower limb associated with chronic lymphedema (Stewart-Treves syndrome) in a patient with cervical cancer
In 1994, Furue et al demonstrated that immunotherapy may be beneficial as palliative treatment for pleural effusions caused by metastatic angiosarcoma:
Expression of VEGF-C makes this angiosarcoma a good potential candidate for targeted antilymphangiogenic therapy
Stewart-Treves syndrome occurring in the abdominal wall was successfully treated with eribulin mesylate:
A structurally modified analog of halichondrin B, originally isolated from the marine sponge Halichondria okadai
References
Cui L, Zhang J, Zhang X, et al. Angiosarcoma (Stewart-Treves syndrome) in postmastectomy patients: report of 10 cases and review of literature. Int J Clin Exp Pathol. 2015;8(9):11108-11115.
Penel N, Bui BN, Bay JO, et al. Phase II trial of weekly paclitaxel for unresectable angiosarcoma: the ANGIOTAX Study. J Clin Oncol. 2008;26(32):5269-5274.
Stewart FW, Treves N. Lymphangiosarcoma in postmastectomy lymphedema: A report of six cases in elephantiasis chirurgica. Cancer. 1948. 1:64-81.
Hallel-Halevy D, Yerushalmi J, Grunwald MH, Avinoach I, Halevy S. Stewart-Treves syndrome in a patient with elephantiasis. J Am Acad Dermatol. 1999 Aug. 41(2 Pt 2):349-50.
Offori TW, Platt CC, Stephens M, Hopkinson GB. Angiosarcoma in congenital hereditary lymphoedema (Milroy’s disease)–diagnostic beacons and a review of the literature. Clin Exp Dermatol. 1993 Mar. 18(2):174-7.
Farhat MM, Le Guern A, Peugniez C, Dabouz F, Quinchon JF, Modiano P. [Angiosarcoma in primary lymphoedema: A rare complication]. Ann Dermatol Venereol. 2018 Apr. 145 (4):266-269.
Schreiber H, Barry FM, Russell WC, Macon WL 4th, Ponsky JL, Pories WJ. Stewart-Treves syndrome. A lethal complication of postmastectomy lymphedema and regional immune deficiency. Arch Surg. 1979 Jan. 114(1):82-5.
Stark RB, Dwyer EM, De Forest M. Effect of surgical ablation of regional lymph nodes on survival of homografts. Ann NY Acad Sci. 1960. 87:140-148.
Cabral ANF, Rocha RH, Amaral ACVD, Medeiros KB, Nogueira PSE, Diniz LM. Cutaneous angiosarcoma: report of three different and typical cases admitted in a unique dermatology clinic. An Bras Dermatol. 2017 Mar-Apr. 92 (2):235-238.
Styring E, Fernebro J, Jonsson PE, et al. Changing clinical presentation of angiosarcomas after breast cancer: from late tumors in edematous arms to earlier tumors on the thoracic wall. Breast Cancer Res Treat. 2010 Jan 20.
Stanczyk M, Gewartowska M, Swierkowski M, Grala B, Maruszynski M. Stewart-Treves syndrome angiosarcoma expresses phenotypes of both blood and lymphatic capillaries. Chin Med J (Engl). 2013 Jan. 126(2):231-7.
Schirger A. Postoperative lymphedema: etiologic and diagnostic factors. Med Clin North Am. 1962 Jul. 46:1045-50.
Wierzbicka-Hainaut E, Guillet G. [Stewart-Treves syndrome (angiosarcoma on lyphoedema): A rare complication of lymphoedema]. Presse Med. 2010 Dec. 39(12):1305-8.
Risk‐reducing bilateral salpingo‐oophorectomy (RRBSO) – or the removal of fallopian tubes and ovaries:
Is the advised surgical prophylaxis for hereditary breast and ovarian cancer (HBOC) mutation carriers
Other preventive and cancer screening measures available for these women:
Bilateral Salpingo‐Oophorectomy
Risk‐reducing bilateral salpingo‐oophorectomy (RRBSO) – or the removal of fallopian tubes and ovaries:
Is the advised surgical prophylaxis for hereditary breast and ovarian cancer (HBOC) mutation carriers
Other preventive and cancer screening measures available for these women:
Such as serial CA125 levels and pelvic ultrasounds:
Have not been shown to reduce cancer mortality in this high‐risk population
RRBSO has been associated with significantly improved cancer‐specific mortality:
For ovarian, fallopian tube, peritoneal and breast cancers, as well as improved all‐cause mortality in BRCA carriers
In a multicenter, prospective study of 2482 women with a known BRCA1 or BRCA2 mutation:
Women treated with RRBSO had a:
Decreased ovarian cancer risk (1% vs 6%)
Decreased breast cancer risk (2% vs 6%)
Improved all‐cause mortality (3% vs 10%)
Retrospective data supports the relative risk of gynecologic cancer:
After RRBSO to be 0.04 (95% CI, 0.01‐0.16)
In that study, only 2 of 253 women who underwent RRBSO were later diagnosed with peritoneal carcinoma:
58 women out of 292 matched controls received a diagnosis of the ovarian, fallopian tube, or peritoneal cancer after a mean follow up of 8.8 years
In a prospective study which controlled for history of prophylactic mastectomy:
The hazard ratio for the diagnosis of breast cancer or gynecologic cancer in a patient with BRCA after RRBSO was 0.25 (95% CI, 0.08‐0.74)
As more recent data have supported that many ovarian cancers may originate within the fallopian tube:
There are currently ongoing studies exploring whether bilateral salpingectomy alone is an effective risk‐reducing procedure
Generally, BRCA‐positive women elect to defer RRBSO:
Until they complete their childbearing
Age‐related risk, however, differs between BRCA1 and BRCA2 carriers:
BRCA1 carriers are at an elevated lifetime risk for ovarian cancer compared to BRCA2 carriers and are also more likely to develop it earlier in life:
Specifically, women with BRCA1 mutations have an:
Average age at ovarian cancer diagnosis of 50 years
A significantly increased ovarian cancer risk starting at 35 years:
Which continues to increase with age
Women with BRCA2 mutations:
Have an average age of ovarian cancer diagnosis of 60 years
A significantly increased ovarian cancer risk starting at 50 years:
Which then plateaus at a 14% risk
Therefore, BRCA2 carriers may elect to defer RRBSO to a later age compared with BRCA1 carriers:
However, if they choose to do so, they must be counseled that they may not receive the benefit of decreased breast cancer risk after RRBSO
Nevertheless, the society of Gynecologic Oncology (SGO):
Continues to recommend that BRCA1 and BRCA2 mutation carriers:
Undergo RRBSO after completing childbearing or by age 35 to 40 years
Thorough preoperative counseling is critical in helping patients decide whether to proceed with RRBSO:
RRBSO is generally performed laparoscopically and is a low‐risk procedure:
The reported complication rate (both major and minor) of RRBSO:
Has been quoted as 4% but is even lower at high volume institutions
In addition, patients must be advised that there is a 4% to 8% risk of discovering an occult malignancyeither at the time of RRBSO or on final pathology
Preoperative serum CA125 should be obtained and patients should undergo a pelvic ultrasound
Patients should be consented for ovarian cancer staging surgery in case visible disease is seen and counseled that an occult malignancy may be detected on final pathology, thus requiring additional surgery
Women should also be counseled that at the time of RRBSO they will undergo surgical menopause and may begin to experience hot flashes, mood changes, vaginal dryness, dyspareunia, decreased libido, osteoporosis, cardiovascular disease, and possible impaired cognitive function:
Although surgical menopause before age 45:
Has been associated with increased overall mortality in the general population, this risk must be balanced with the substantially decreased all‐cause mortality after risk‐reducing surgery for the high‐risk HBOC population
Nonhormonal agents should be used as a first‐line therapy for these symptoms:
But hormonal replacement therapy (HRT) is also likely safe on the basis of a recent study of almost 900 postoophorectomy BRCA1 mutation carriers:
In that prospective longitudinal study, investigators found that HRT use was not associated with an increased risk of breast cancer (HR 0.97, 95% CI, 0.62‐1.52, P = .89)
However, when analyzing only women who used HRT:
The incidence of breast cancer was lower with estrogen‐only HRTcompared with combination estrogen and progesterone (12% vs 22%, log‐rank P = .04)
Estrogen‐only HRT is only recommended for women who have undergone a hysterectomy, as without progesterone support, it significantly increases the risk for endometrial cancer in the general population
A recent meta‐analysis including three trials with 1100 patients also demonstrated there was not a significantly higher breast cancer risk associated with HRT after RRBSO in BRCA1 and BRCA2 mutation carriers (HR 0.98, 95% CI, 0.63‐1.52)
Nevertheless, the relationship between HRT and individual all‐cancer risk is complex and imperfectly understood at this time
The results of long‐term, prospective studies are necessary to draw more definitive conclusions in this high‐risk population
References:
Domchek SM, Friebel TM, Singer CF, et al. Association of risk‐ reducing surgery in BRCA1 or BRCA2 mutation carriers with cancer risk and mortality. JAMA. 2010;304(9):967‐975.
Rebbeck TR, Lynch HT, Neuhausen SL, et al. Prophylactic oophor- ectomy in carriers of BRCA1 or BRCA2 mutations. N Engl J Med. 2002;346(21):1616‐1622.
Kauff ND, Satagopan JM, Robson ME, et al. Risk‐reducing salpingo‐ oophorectomy in women with a BRCA1 or BRCA2 mutation. N Engl J Med. 2002;346(21):1609‐1615.
Antoniou A, Pharoah PDP, Narod S, et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case Series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet. 2003;72(5):1117‐1130.
Manchanda R, Abdelraheim, Johnson M, et al. Outcome of risk‐ reducing salpingo‐oophorectomy in BRCA carriers and women of unknown mutation status. BJOG. 2011;118(7):814‐824.
Rocca WA, Grossardt BR, de Andrade M, Malkasian GD, Melton LJ. Survival patterns after oophorectomy in premenopausal women: a population‐based cohort study. Lancet Oncol. 2006;7(10):821‐828.
Kotsopoulos J, Gronwald J, Karlan BY, et al. Hormone replacement therapy after oophorectomy and breast cancer risk among BRCA1 mutation carriers. JAMA Oncology. 2018;4(8):1059.
Marchetti C, De Felice F, Boccia S, et al. Hormone replacement therapy after prophylactic risk‐reducing salpingo‐oophorectomy and breast cancer risk in BRCA1 and BRCA2 mutation carriers: a meta‐ analysis. Crit Rev Oncol Hematol. 2018;132:111‐115.
Such as serial CA125 levels and pelvic ultrasounds:
Have not been shown to reduce cancer mortality in this high‐risk population
RRBSO has been associated with significantly improved cancer‐specific mortality:
For ovarian, fallopian tube, peritoneal and breast cancers, as well as improved all‐cause mortality in BRCA carriers
In a multicenter, prospective study of 2482 women with a known BRCA1 or BRCA2 mutation:
Women treated with RRBSO had a:
Decreased ovarian cancer risk (1% vs 6%)
Decreased breast cancer risk (2% vs 6%)
Improved all‐cause mortality (3% vs 10%)
Retrospective data supports the relative risk of gynecologic cancer:
After RRBSO to be 0.04 (95% CI, 0.01‐0.16)
In that study, only 2 of 253 women who underwent RRBSO were later diagnosed with peritoneal carcinoma:
58 women out of 292 matched controls received a diagnosis of the ovarian, fallopian tube, or peritoneal cancer after a mean follow up of 8.8 years
In a prospective study which controlled for history of prophylactic mastectomy:
The hazard ratio for the diagnosis of breast cancer or gynecologic cancer in a patient with BRCA after RRBSO was 0.25 (95% CI, 0.08‐0.74)
As more recent data have supported that many ovarian cancers may originate within the fallopian tube:
There are currently ongoing studies exploring whether bilateral salpingectomy alone is an effective risk‐reducing procedure
Generally, BRCA‐positive women elect to defer RRBSO:
Until they complete their childbearing
Age‐related risk, however, differs between BRCA1 and BRCA2 carriers:
BRCA1 carriers are at an elevated lifetime risk for ovarian cancer compared to BRCA2 carriers and are also more likely to develop it earlier in life:
Specifically, women with BRCA1 mutations have an:
Average age at ovarian cancer diagnosis of 50 years
A significantly increased ovarian cancer risk starting at 35 years:
Which continues to increase with age
Women with BRCA2 mutations:
Have an average age of ovarian cancer diagnosis of 60 years
A significantly increased ovarian cancer risk starting at 50 years:
Which then plateaus at a 14% risk
Therefore, BRCA2 carriers may elect to defer RRBSO to a later age compared with BRCA1 carriers:
However, if they choose to do so, they must be counseled that they may not receive the benefit of decreased breast cancer risk after RRBSO
Nevertheless, the society of Gynecologic Oncology (SGO):
Continues to recommend that BRCA1 and BRCA2 mutation carriers:
Undergo RRBSO after completing childbearing or by age 35 to 40 years
Thorough preoperative counseling is critical in helping patients decide whether to proceed with RRBSO:
RRBSO is generally performed laparoscopically and is a low‐risk procedure:
The reported complication rate (both major and minor) of RRBSO:
Has been quoted as 4% but is even lower at high volume institutions
In addition, patients must be advised that there is a 4% to 8% risk of discovering an occult malignancyeither at the time of RRBSO or on final pathology
Preoperative serum CA125 should be obtained and patients should undergo a pelvic ultrasound
Patients should be consented for ovarian cancer staging surgery in case visible disease is seen and counseled that an occult malignancy may be detected on final pathology, thus requiring additional surgery
Women should also be counseled that at the time of RRBSO they will undergo surgical menopause and may begin to experience hot flashes, mood changes, vaginal dryness, dyspareunia, decreased libido, osteoporosis, cardiovascular disease, and possible impaired cognitive function:
Although surgical menopause before age 45:
Has been associated with increased overall mortality in the general population, this risk must be balanced with the substantially decreased all‐cause mortality after risk‐reducing surgery for the high‐risk HBOC population
Nonhormonal agents should be used as a first‐line therapy for these symptoms:
But hormonal replacement therapy (HRT) is also likely safe on the basis of a recent study of almost 900 postoophorectomy BRCA1 mutation carriers:
In that prospective longitudinal study, investigators found that HRT use was not associated with an increased risk of breast cancer (HR 0.97, 95% CI, 0.62‐1.52, P = .89)
However, when analyzing only women who used HRT:
The incidence of breast cancer was lower with estrogen‐only HRTcompared with combination estrogen and progesterone (12% vs 22%, log‐rank P = .04)
Estrogen‐only HRT is only recommended for women who have undergone a hysterectomy, as without progesterone support, it significantly increases the risk for endometrial cancer in the general population
A recent meta‐analysis including three trials with 1100 patients also demonstrated there was not a significantly higher breast cancer risk associated with HRT after RRBSO in BRCA1 and BRCA2 mutation carriers (HR 0.98, 95% CI, 0.63‐1.52)
Nevertheless, the relationship between HRT and individual all‐cancer risk is complex and imperfectly understood at this time
The results of long‐term, prospective studies are necessary to draw more definitive conclusions in this high‐risk population
References:
Domchek SM, Friebel TM, Singer CF, et al. Association of risk‐ reducing surgery in BRCA1 or BRCA2 mutation carriers with cancer risk and mortality. JAMA. 2010;304(9):967‐975.
Rebbeck TR, Lynch HT, Neuhausen SL, et al. Prophylactic oophor- ectomy in carriers of BRCA1 or BRCA2 mutations. N Engl J Med. 2002;346(21):1616‐1622.
Kauff ND, Satagopan JM, Robson ME, et al. Risk‐reducing salpingo‐ oophorectomy in women with a BRCA1 or BRCA2 mutation. N Engl J Med. 2002;346(21):1609‐1615.
Antoniou A, Pharoah PDP, Narod S, et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case Series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet. 2003;72(5):1117‐1130.
Manchanda R, Abdelraheim, Johnson M, et al. Outcome of risk‐ reducing salpingo‐oophorectomy in BRCA carriers and women of unknown mutation status. BJOG. 2011;118(7):814‐824.
Rocca WA, Grossardt BR, de Andrade M, Malkasian GD, Melton LJ. Survival patterns after oophorectomy in premenopausal women: a population‐based cohort study. Lancet Oncol. 2006;7(10):821‐828.
Kotsopoulos J, Gronwald J, Karlan BY, et al. Hormone replacement therapy after oophorectomy and breast cancer risk among BRCA1 mutation carriers. JAMA Oncology. 2018;4(8):1059.
Marchetti C, De Felice F, Boccia S, et al. Hormone replacement therapy after prophylactic risk‐reducing salpingo‐oophorectomy and breast cancer risk in BRCA1 and BRCA2 mutation carriers: a meta‐ analysis. Crit Rev Oncol Hematol. 2018;132:111‐115.
Bilateral mastectomy is advised to reduce the risk of breast cancer
Mastectomy has been shown to reduce the risk of breast cancer:
In patients with hereditary cancer by 90%, according to both retrospective and prospective studies
In many of the seminal studies investigating surgical prophylaxis of breast cancer:
The type of surgery performed was a total (or simple) mastectomy:
Which consists of removing all breast tissue, including overlying skin, as well as the nipple‐areolar complex while sparing the pectoral muscles and axillary content
In the PROSE study:
The only two women diagnosed with breast cancer after surgical prophylaxis:
Had undergone skin‐sparing instead of total mastectomies:
One of these patients was diagnosed with metastatic breast cancer at the time of surgery
The other woman went on to develop breast cancer within the residual breast epithelium
Therefore, total mastectomy:
Is still the recommended risk‐reducing surgery in BRCA carriers
Nipple‐sparing (NSM) and skin‐sparing (SSM) mastectomies:
Require a less extensive reconstruction and often a better cosmetic result
Since the PROSE study in 2004:
A piece of mounting evidence demonstrates that NSM, as well as SSM:
May be effective forms of surgical prophylaxis in BRCA carriers
In a recent retrospective study, patients with BRCA who underwent prophylactic NSM at nine institutions from 1968 to 2013 were reviewed
In this cohort, all 346 BRCA mutation carriers who did not have incidental cancer on final pathology:
Did not develop breast cancer after 36 months of follow up
Using risk models for BRCA carriers:
The authors approximated that 22 primary breast cancers were expected in this cohort without prophylactic NSM
Nevertheless, this was a retrospective study and more evidence is needed for NSM to replace the currently recommended total mastectomy for surgical prophylaxis of breast cancer in BRCA patients
References:
Rebbeck TR, Friebel T, Lynch HT, et al. Bilateral prophylactic mastectomy reduces breast cancer risk in BRCA1 and BRCA2 mutation carriers: the PROSE Study Group. J Clin Oncol. 2004;22(6): 1055‐1062.
Ludwig KK, Neuner J, Butler A, Geurts JL, Kong AL. Risk reduction and survival benefit of prophylactic surgery in BRCA mutation carriers, a systematic review. Am J Surg. 2016;212(4):660‐669.
Jakub JW, Peled AW, Gray RJ, et al. Oncologic safety of prophylactic nipple‐sparing mastectomy in a population with BRCA mutations: a multi‐institutional study. JAMA Surg. 2018;153(2):123‐129.
Yao K, Liederbach E, Tang R, et al. Nipple‐sparing mastectomy in BRCA1/2 mutation carriers: an interim analysis and review of the literature. Ann Surg Oncol. 2015;22(2):370‐376.
Domchek SM, Friebel TM, Singer CF, et al. Association of risk‐ reducing surgery in BRCA1 or BRCA2 mutation carriers with cancer risk and mortality. JAMA. 2010;304(9):967‐975.
Women who present with a significant family history of breast and / or ovarian cancer:
Should be referred to a genetic counselor for formal risk assessment:
Before undergoing BRCA testing
Many organizations, such as the United States Preventative Services Task Force, the American College of Medical Genetics and Genomics, and the National Comprehensive Cancer Network have published guidelines for whom to refer to genetic counselors:
These guidelines are on the basis of:
The numberof affected family members
Their degree of relation to the individual in question
The age at diagnosis
More than one primary cancer
Ethnicity
Indications For Screening of Genetic Mutations Associated with Ovarian Cancer
Women who present with a significant family history of breast and / or ovarian cancer:
Should be referred to a genetic counselor for formal risk assessment:
Before undergoing BRCA testing
Many organizations, such as the United States Preventative Services Task Force, the American College of Medical Genetics and Genomics, and the National Comprehensive Cancer Network have published guidelines for whom to refer to genetic counselors:
These guidelines are on the basis of:
The numberof affected family members
Their degree of relation to the individual in question
The age at diagnosis
More than one primary cancer
Ethnicity
There are also formal risk assessment calculators for patients who do not have a personal history of cancer:
Such as the BRCAPRO and Tyrer‐Cuzick models:
These calculators can aid in determining whether a patient:
Should be referred to a genetic counselor (ie, have a high risk of carrying a BRCA1 or BRCA2 mutation)
As well as screening modalities and time intervals on the basis of their calculated risk of breast cancer:
However, these models do not provide probabilities of testing positive for moderate‐risk (ie, BRIP1, RAD51C, PALB2) or non‐BRCA high‐risk gene mutations
There is much debate about whether all Ashkenazi Jews:
Should be routinely offered BRCA testing:
Regardless of personal or family history of cancer given the high frequency of BRCA mutations in that population:
Several studies have found that genetic testing of Ashkenazi Jews on the basis of family history criteria:
Would miss a number of BRCA carriers
In one study, over 8000 Ashkenazi Jewish men were tested:
175 were found to be BRCA‐positive:
Half of those BRCA mutation carriers had no family history of breast or ovarian cancer
Population‐based BRCA testing has also been shown to be cost‐effective compared with family history‐based testing of Ashkenazi Jewish women
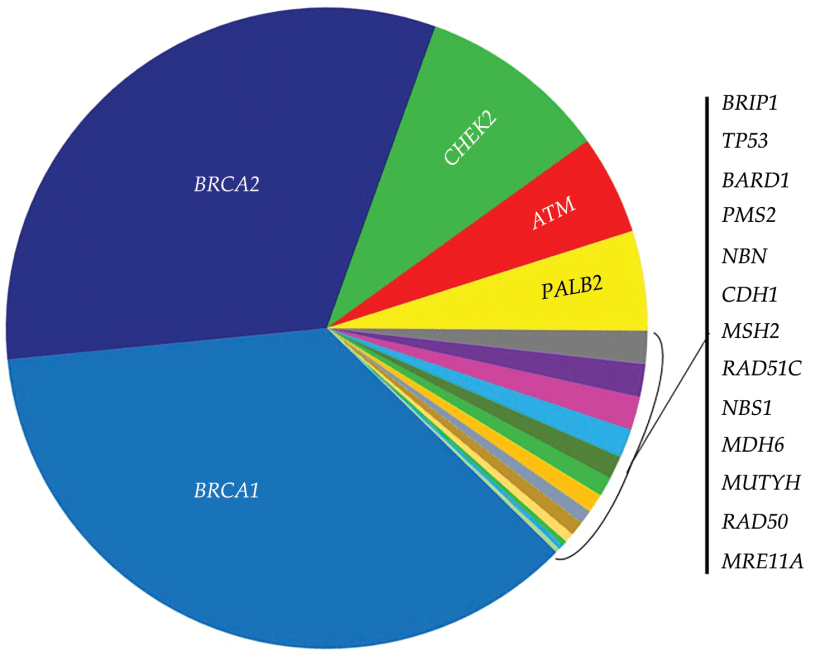
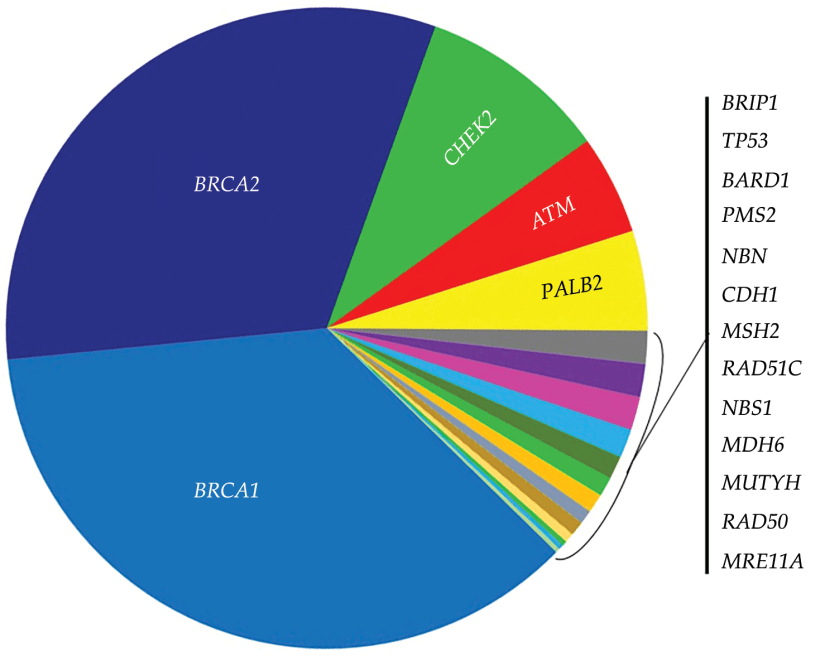
For patients who meet criteria for HBOC genetic testing:
The current recommended test is a next‐generation multigene panel:
Which includes BRCA 1 and BRCA2 as well as several moderate‐risk genes (eg, CHEK2, ATM, PALB2, RAD51C)
Many organizations, such as the National Comprehensive Cancer Network (NCCN), American College of Obstetricians and Gynecologists (ACOG), Society for Gynecologic Oncology (SGO), and American Society of Clinical Oncology (ASCO):
Recommend germline testing for all patients diagnosed with EOC:
Regardless of age, family history, or ethnicity
Despite this unanimity from these institutions:
Estimated U.S. germline testing rates for women with EOC remains low:
At 20% to 30%, and even lower for minority women
References:
Hampel H, Bennett RL, Buchanan A, Pearlman A, Wiesner GL. American College of Medical Genetics and Genomics Professional Practice and Guidelines Committee and National Society of Genetic Counselors Practice Guidelines Committee, “A practice guideline from the American College of Medical Genetics and Genomics and the National Society of Genetic Counselors: referral indications for cancer predisposition assessment. Genet Med. 2015;17(1):70‐87. and Guideline Development Group.
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines), “Genetic/Familial High‐risk Assessment: Breast and Ovarian,” National Comprehensive Cancer Network, Version 3.2019, Jan. 2019.
“Final Recommendation Statement: BRCA‐Related Cancer: Risk Assess- ment, Genetic Counseling, and Genetic Testing. U.S. Preventive Services Task Force. December 2013. https://www.uspreventiveservicestaskforce. org/Page/Document/RecommendationStatementFinal/brca‐related‐cancer‐risk assessment‐genetic‐counseling‐and‐genetic‐testing.”
Committee on Practice Bulletins–Gynecology. Committee on Genet- ics, Society of Gynecologic Oncology, “Practice bulletin No 182: hereditary breast and ovarian cancer syndrome. Obstet Gynecol. 2017;130(3):e110‐e126.
Lu KH, Wood ME, Daniels M, et al American Society of Clinical Oncology Expert Statement: collection and use of a cancer family history for oncology providers. J Clin Oncol. 2014;32(8):833‐840.
Gabai‐Kapara E, Lahad A, Kaufman B, et al Population‐based screening for breast and ovarian cancer risk due to BRCA1 and 132.
Proc Natl Acad Sci USA. 2014;111(39):14205‐14210. Manchanda R, Legood R, Burnell M, et al. Cost‐effectiveness of population screening for BRCA mutations in Ashkenazi jewish women compared with family history‐based testing. J Natl Cancer
Inst. 2015;107(1):380.
Tung N, Battelli C, Allen B, et al Frequency of mutations in individuals
with breast cancer referred for BRCA1 and BRCA2 testing using next‐generation sequencing with a 25‐gene panel. Cancer. 2015;121(1):25‐33.
Levy DE, Byfield SD, Comstock CB, et al. Underutilization of BRCA1/ 2 testing to guide breast cancer treatment: black and Hispanic women particularly at risk. Genet Med. 2011;13(4):349‐355.
Partner and localizer of BRCA2 (PALB2) germline mutation:
Is associated with an – albeit small – increased risk of ovarian cancer compared with the general population
In a recent study of 1421 patients with epithelial and ovarian cancer (EOC):
Three (0.21%) had a germline PALB2 mutation compared with 0.05% of the control cohort of 4300 subjects
Similarly, BRIP1 germline mutations:
Were found in 0.41% to 0.9% of patients with EOC compared with 0.09% in the general population
In a study of 1100 German pedigrees, families with a history of gynecologic or breast cancers without BRCA1 or BRCA2 mutations:
Had a higher incidence of RAD51C mutations compared to the 3000 control families with no mutation carriers
The exact penetrance of this mutation is not known:
But the approximate cumulative risk of ovarian cancer in RAD51C carriers is:
1% by age 49
6% by age 80
Although these genes only confer a moderate risk for EOC, given the poor survival estimates for ovarian cancer:
The clinical implications for families with carriers of these mutations is great
Other genetic syndromes can confer increased susceptibility to breast and / or ovarian cancers:
Peutz‐Jeghers syndrome (PJS):
Which is a result of mutations in the serine / threonine kinase 11 gene (STK11, also called LKB1):
Is associated with the increased risk of gastrointestinal cancers
However, it has also been shown to confer an:
Increased lifetime risk of breast:
32%
Increased lifetime risk of ovarian cancers:
21%
Patients with PJS are at risk for:
Ovarian sex‐cord stromal tumors:
Not epithelial ovarian cancers, and they are usually diagnosed in childhood or young adulthood
When an identifiable mutation cannot be found in a patient with a strong family history of ovarian and / or breast cancer:
Our practice is to counsel women that their risk may be elevated compared with the general population but continue to discourage serial Ca‐125 levels, serial ultrasounds, and rrBSO
We also recommend retesting when new multigene panels are produce
References:
Konstantinopoulos PA, Ceccaldi R, Shapiro GI, D’Andrea AD. Homologous recombination deficiency: exploiting the fundamental vulnerability of ovarian cancer. Cancer Discov. 2015;5(11):1137‐1154.
Kotsopoulos J, Sopik V, Rosen B, et al. Frequency of germline PALB2 mutations among women with epithelial ovarian cancer. Fam Cancer. 2017;16(1):29‐34.
Ramus SJ, Song H, Dicks Ed, et al Germline mutations in the BRIP1, BARD1, PALB2, and NBN genes in women with ovarian cancer. J Natl Cancer Inst. 2015;107(11).
Tung N, Domchek SM, Stadler Z, et al. Counselling framework for moderate‐penetrance cancer‐susceptibility mutations. Nat Rev Clin Oncol. 2016;13(9):581‐588.
vanLierMGF,WagnerA,Mathus‐VliegenEMH,etalHighcancerrisk in Peutz‐Jeghers syndrome: a systematic review and surveillance recommendations. Am J Gastroenterol. 2010;105(6):1258‐1264.
Approximately 22 000 women received a new diagnosis of ovarian cancer, and there were 14 000 ovarian cancer deaths
Inherited germline mutations:
That increase the risk for ovarian cancer:
Are present in approximately 7% to 25% of these women
Hereditary breast and ovarian cancer syndrome (HBOC):
Is the most common genetic syndrome:
Linked to ovarian cancer:
Is associated with mutations in the BRCA genes
BRCA1 and BRCA2 are:
Tumor suppressor genes:
Involved in the repair of double‐strandedDNA breaks
Certain populations are at significantly higher risk forBRCA mutations than the general population including:
AshkenaziJewish, French Canadian, and Icelandic populations:
This is because of the founder effect:
Which causes a decrease in genetic diversity in a population that is geographically or reproductively isolated
For example, in the general United States non‐Jewish population:
The risk of inheriting a BRCA mutation is 1 in 400 compared with theAshkenazi Jewish population, who carry an increased risk of 1 in 40
The inheritance pattern of the BRCA mutations is:
Autosomaldominant:
However, tumor suppressor genes are known to be recessive, requiring both copies of the gene to be affected
Therefore, a germline BRCA mutation is inherited in one copy of the gene, the second copy then undergoes a somatic mutation:
The second hit and the carrier is phenotypically affected
The most recently estimated cumulative cancer risk by age 80 for:
BRCA1 carriers is:
72%
BRCA2 carriers is:
69%
By comparison, the lifetime risk of ovarian and breast cancer in the general population is:
1.3% and 12.4%, respectively
Furthermore, the lifetime risk for ovarian cancer in:
BRCA1 carriers is:
44%
BRCA2 carriers is:
17%
BRCA carriers are also at risk for other cancers including:
Pancreatic, prostate, melanoma, and colon cancer
Recently, findings by Shu et al8 suggest that BRCA1 carriers:
Have an increased risk for uterine papillary serous carcinoma:
A rare but aggressive type of uterine cancer
In a prospective cohort of 627 BRCA1 carriers:
Four women developed serious uterine cancer:
Which was double the expected incidence in the general population
References:
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7‐34.
Noone AM, Howlader N, Krapcho M, et al. “SEER Cancer Statistics Review, 1975‐2015,” National Cancer Institute, Bethesda, MD, 2018.
Morgan RD, Burghel GJ, Flaum N, et al Prevalence of germline pathogenic BRCA1/2 variants in sequential epithelial ovarian cancer cases. J Med Genet. 2019;56:301‐307.
McClainMR,PalomakiGE,NathansonKL,etalAdjustingtheestimated proportion of breast cancer cases associated with BRCA1 and BRCA2 mutations: public health implications. Genet Med. 2005;7(1):28‐33.
Gudmundsson J, Johannesdottir G, Bergthorsson JT, et al Different tumor types from BRCA2 carriers show wild‐type chromosome deletions on 13q12‐q13. Cancer Res. 1995;55(21):4830‐4832.
Kuchenbaecker KB, Hopper JL, Barnes DR, et al Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA. 2017;317(23):2402‐2416.
Mersch J, Jackson MA, Park M, et al Cancers associated with BRCA1 and BRCA2 mutations other than breast and ovarian. Cancer. 2015;121(2):269‐275.
Axillary sentinel node biopsy has been shown to be feasible for axillary staging:
In patients with in-breast recurrence or ipsilateral breast second primary tumors
Limited prior axillary sampling (less than nine nodes) has been shown to have greater success in localization
Preoperative lymphoscintigraphy should be considered:
Given the possibility of aberrant lymphatic drainage due to alterations secondary to prior surgery and radiation
References
Tokmak H, Kaban K, Muslumanoglu M, Demirel M, Aktan S. Management of sentinel node re-mapping in patients who have second or recurrent breast cancer and had previous axillary procedures. World J Surg Oncol. 2014;12:205.
Kothari MS, Rusby JE, Agusti AA, MacNeill FA. Sentinel lymph node biopsy after previous axillary surgery: a review. Eur J Surg Oncol. 2012;38(1):8-15.
There has been a significant focus on the role of contralateral prophylactic mastectomy and the risk of contralateral breast cancer
Single-institution studies and Surveillance, Epidemiology, and End Results program (SEER) data:
Have found contralateral prophylactic mastectomy rates:
To be as high as 25%, which continue to increase
Further, this trend seems to be limited to the United States
Nichols et al. reviewed rates of contralateral breast cancer between 1976 and 2006 using the SEER database:
Overall, they found the rate of contralateral breast cancer:
To be declining approximately 3% per year since 1985
From 1990 forward:
They found this benefit to be restricted to those presenting with an ER+ breast cancer:
With annual incidence rates of contralateral breast cancer of 0.25% to 0.37% when the index cancer was diagnosed after age 30 years
The rates of contralateral breast cancer were higher in patients with ER negative breast cancers:
But still remained reasonably low with annual incidence rates of contralateral breast cancer of 0.45% to 0.65% when the index cancer was diagnosed after age 40 years
The use of adjuvant endocrine therapy has contributed to this decline in contralateral breast cancer rates:
As it reduces the risk of contralateral breast cancer by approximately 50%
Contralateral prophylactic mastectomy:
Is attributed with approximately a 90% to 94% overall reduction in the risk of contralateral breast cancer, not 100%
Contralateral prophylactic mastectomy:
Does not improve overall survival
Recent modeling suggests the added absolute benefit of contralateral prophylactic mastectomy to overall survival is less than 1.45%
The American Society of Breast Surgeons published a consensus statement with indications and suggestions for patient management and decision making with regard to contralateral prophylactic mastectomy:
Discouraging the procedure for women with unilateral breast cancer at average risk for contralateral cancer
References
Nichols HB, Berrington de Gonzalez A, Lacey JV, Rosenberg PS, Anderson WF. Declining incidence of contralateral breast cancer in the United States from 1975 to 2006. J Clin Oncol. 2011;29(12):1564-1569.
Early Breast Cancer Trialists’ Collaborative Group, Davies C, Godwin J, et al. Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: patient-level meta-analysis of randomised trials. Lancet. 2011;378(9793):771-784.
King TA, Sakr R, Patil S, et al. Clinical management factors contribute to the decision for contralateral prophylactic mastectomy. J Clin Oncol. 2011;29(16):2158-2164.
Metcalfe K, Lynch HT, Ghadirian P, et al. Contralateral breast cancer in BRCA1 and BRCA2 mutation carriers. J Clin Oncol. 2004;22(12):2328-2335.
Portschy PR, Kuntz KM, Tuttle TM. Survival outcomes after contralateral prophylactic mastectomy: a decision analysis. J Natl Cancer Inst. 2014;106(8).
Boughey JC, Attai DJ, Chen SL, et. al.. Contralateral prophylactic mastectomy consensus statement from the American Society of Breast Surgeons: additional considerations and a framework for shared decision making. Ann Surg Oncol. 2016 Oct;23(10):3106-3111.