- Women who present with a significant family history of breast and / or ovarian cancer:
- Should be referred to a genetic counselor for formal risk assessment:
- Before undergoing BRCA testing
- Should be referred to a genetic counselor for formal risk assessment:
- Many organizations, such as the United States Preventative Services Task Force, the American College of Medical Genetics and Genomics, and the National Comprehensive Cancer Network have published guidelines for whom to refer to genetic counselors:
- These guidelines are on the basis of:
- The number of affected family members
- Their degree of relation to the individual in question
- The age at diagnosis
- More than one primary cancer
- Ethnicity
- These guidelines are on the basis of:
Indications For Screening of Genetic Mutations Associated with Ovarian Cancer
- Women who present with a significant family history of breast and / or ovarian cancer:
- Should be referred to a genetic counselor for formal risk assessment:
- Before undergoing BRCA testing
- Should be referred to a genetic counselor for formal risk assessment:
- Many organizations, such as the United States Preventative Services Task Force, the American College of Medical Genetics and Genomics, and the National Comprehensive Cancer Network have published guidelines for whom to refer to genetic counselors:
- These guidelines are on the basis of:
- The number of affected family members
- Their degree of relation to the individual in question
- The age at diagnosis
- More than one primary cancer
- Ethnicity
- These guidelines are on the basis of:
- There are also formal risk assessment calculators for patients who do not have a personal history of cancer:
- Such as the BRCAPRO and Tyrer‐Cuzick models:
- These calculators can aid in determining whether a patient:
- Should be referred to a genetic counselor (ie, have a high risk of carrying a BRCA1 or BRCA2 mutation)
- As well as screening modalities and time intervals on the basis of their calculated risk of breast cancer:
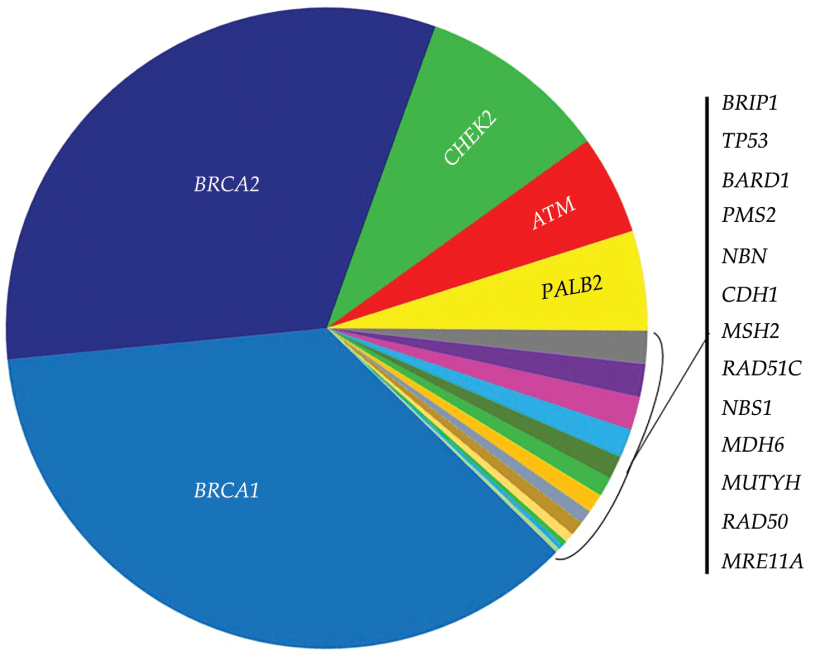
- However, these models do not provide probabilities of testing positive for moderate‐risk (ie, BRIP1, RAD51C, PALB2) or non‐BRCA high‐risk gene mutations
- These calculators can aid in determining whether a patient:
- Such as the BRCAPRO and Tyrer‐Cuzick models:
- There is much debate about whether all Ashkenazi Jews:
- Should be routinely offered BRCA testing:
- Regardless of personal or family history of cancer given the high frequency of BRCA mutations in that population:
- Several studies have found that genetic testing of Ashkenazi Jews on the basis of family history criteria:
- Would miss a number of BRCA carriers
- Several studies have found that genetic testing of Ashkenazi Jews on the basis of family history criteria:
- Regardless of personal or family history of cancer given the high frequency of BRCA mutations in that population:
- In one study, over 8000 Ashkenazi Jewish men were tested:
- 175 were found to be BRCA‐positive:
- Half of those BRCA mutation carriers had no family history of breast or ovarian cancer
- 175 were found to be BRCA‐positive:
- Population‐based BRCA testing has also been shown to be cost‐effective compared with family history‐based testing of Ashkenazi Jewish women
- Should be routinely offered BRCA testing:
- For patients who meet criteria for HBOC genetic testing:
- The current recommended test is a next‐generation multigene panel:
- Which includes BRCA 1 and BRCA2 as well as several moderate‐risk genes (eg, CHEK2, ATM, PALB2, RAD51C)
- The current recommended test is a next‐generation multigene panel:
- Many organizations, such as the National Comprehensive Cancer Network (NCCN), American College of Obstetricians and Gynecologists (ACOG), Society for Gynecologic Oncology (SGO), and American Society of Clinical Oncology (ASCO):
- Recommend germline testing for all patients diagnosed with EOC:
- Regardless of age, family history, or ethnicity
- Recommend germline testing for all patients diagnosed with EOC:
- Despite this unanimity from these institutions:
- Estimated U.S. germline testing rates for women with EOC remains low:
- At 20% to 30%, and even lower for minority women
- Estimated U.S. germline testing rates for women with EOC remains low:
- References:
- Hampel H, Bennett RL, Buchanan A, Pearlman A, Wiesner GL. American College of Medical Genetics and Genomics Professional Practice and Guidelines Committee and National Society of Genetic Counselors Practice Guidelines Committee, “A practice guideline from the American College of Medical Genetics and Genomics and the National Society of Genetic Counselors: referral indications for cancer predisposition assessment. Genet Med. 2015;17(1):70‐87. and Guideline Development Group.
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines), “Genetic/Familial High‐risk Assessment: Breast and Ovarian,” National Comprehensive Cancer Network, Version 3.2019, Jan. 2019.
- “Final Recommendation Statement: BRCA‐Related Cancer: Risk Assess- ment, Genetic Counseling, and Genetic Testing. U.S. Preventive Services Task Force. December 2013. https://www.uspreventiveservicestaskforce. org/Page/Document/RecommendationStatementFinal/brca‐related‐cancer‐risk assessment‐genetic‐counseling‐and‐genetic‐testing.”
- Committee on Practice Bulletins–Gynecology. Committee on Genet- ics, Society of Gynecologic Oncology, “Practice bulletin No 182: hereditary breast and ovarian cancer syndrome. Obstet Gynecol. 2017;130(3):e110‐e126.
- Lu KH, Wood ME, Daniels M, et al American Society of Clinical Oncology Expert Statement: collection and use of a cancer family history for oncology providers. J Clin Oncol. 2014;32(8):833‐840.
- Gabai‐Kapara E, Lahad A, Kaufman B, et al Population‐based
screening for breast and ovarian cancer risk due to BRCA1 and 132.
- Proc Natl Acad Sci USA. 2014;111(39):14205‐14210. Manchanda R, Legood R, Burnell M, et al. Cost‐effectiveness of population screening for BRCA mutations in Ashkenazi jewish women compared with family history‐based testing. J Natl Cancer
- Inst. 2015;107(1):380.
- Tung N, Battelli C, Allen B, et al Frequency of mutations in individuals
- with breast cancer referred for BRCA1 and BRCA2 testing using next‐generation sequencing with a 25‐gene panel. Cancer. 2015;121(1):25‐33.
- Levy DE, Byfield SD, Comstock CB, et al. Underutilization of BRCA1/ 2 testing to guide breast cancer treatment: black and Hispanic women particularly at risk. Genet Med. 2011;13(4):349‐355.
#Arrangoiz #CASO #BreastSurgeon #BreastCancer #HereditaryBreastCancer #CancerSurgeon #Miami #CenterforAdvancedSurgicalOncology
