My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
• Has been used in the management of patients with well-differentiated (papillary or follicular) thyroid cancer since the 1940s
• Thyroid tissue has a unique ability to take up iodine from blood:
• Like iodine, radioiodine is taken up and concentrated in thyroid follicular cells:
• Because they have a membrane sodium-iodide transporter
• Compared with normal thyroid follicular cells:
• Thyroid cancer cells have reduced expression of the transporter:
• Which may account for the low iodine-131 (131-I) uptake in thyroid cancer tissue
• 131-I:
• Causes acute thyroid cell death by:
• Emission of short path-length (1 to 2 mm) beta particles
• The uptake of 131-I by thyroid tissue:
• Can be visualized by scanning to detect the gamma radiation that is also emitted by the isotope
• 131-I must be taken up by thyroid tissue to be effective:
• As a result, it is of no value in patients whose thyroid cancers do not concentrate iodide:
• Patients with medullary cancer, lymphoma, or anaplastic cancer
Goals of Radioactive Iodine Treatment
• In an effort to standardize terminology:
• An inter-societal working group with representatives from the American Thyroid Association (ATA), the European Thyroid Association, the European Association of Nuclear Medicine, and the Society of Nuclear Medicine and Molecular Imaging reached the following consensus regarding the goals of iodine-131 (131-I) therapy in differentiated thyroid cancer:
• Remnant ablation:
• The primary goal of remnant ablation is:
• Destruction of presumably benign thyroid tissue after total thyroidectomy:
• To facilitate initial staging and follow-up studies. This will, in turn:
• Improve the specificity of measurements of serum thyroglobulin (Tg) as a tumor marker
• Increase the specificity of 131-I scanning for detection of recurrent or metastatic disease:
• By eliminating uptake by residual normal tissue
• Adjuvant treatment:
• The primary goal of adjuvant treatment is destruction of subclinical tumor deposits:
• That may or may not be present after surgical resection of all known primary tumor tissue and metastatic foci
• Since adjuvant treatment is given based on the risk of having persistent / recurrent diseasewithout definitive evidence of biochemical or structural evidence of disease:
• It is accepted that some patients selected for adjuvant treatment might already have been treated sufficiently by their primary surgery
• Thus, the decision to recommend adjuvant treatment requires:
• Balancing oncological risk (risk of persistent / recurrent disease and disease-specific mortality) and the risks associated with adjuvant treatment (short- and long-term risks of 131-I):
• With the potential benefit of adjuvant treatment (potential to decrease recurrence, improve progression-free survival, and/or improve disease-specific mortality)
• Thus, in properly selected patients, the potential benefits of 131-I adjuvant treatment could include:
• Destruction of subclinical, microscopic foci of disease remaining after surgery
• Decreased risk of recurrence
• Improved disease-specific survival
• Improved progression-free survival
• Treatment of known disease:
• The primary goal in the treatment of known disease is:
• Destruction of clinically apparent macroscopic disease (evidenced by either abnormal thyroglobulin values or structural findings) that is not amenable to surgical therapy
• Radioiodine treatment of residual disease and metastatic disease:
• May reduce the risk of recurrence and mortality:
• Especially in small-volume disease that is radioiodine avid
The majority of TNBCs are detected clinically as a:
Mass, either by the patient or examining clinician
Other possible presenting symptoms include:
Breast pain
Bloody nipple discharge
In the institutional review by Krizmanich-Conniff and colleagues, when compared with non-TNBCs:
TNBCs were more likely to present clinically:
68% versus 48%
The remaining 32% of TNBCs were found on screening mammography:
Whereas 52% of non-TNBCs were found by screening
More than one-third of patients whose TNBC was detected clinically had no prior mammography:
Of those detected by mammography:
One-third had developed within 12 months of the last mammography:
The high incidence of interval cancers is attributed to the aggressive growth rate of TNBC
Imaging:
Mammographic characteristics of TNBC included:
A round mass (59.3%) or an oval or lobulated mass (65%), with circumscribed (15%), microlobulated (12.5%), or indistinct margins (55%)
Spiculated margins were much less common (15%)
On mammography, TNBCs are most likely seen as:
A noncalcified mass:
58%
Dogan and Turnbull caution that TNBC may lack the typical mammographic features of breast cancer, and although ultrasonography adds to the sensitivity of diagnosis:
21% to 41% of TNBCs can have benign characteristics on breast imaging
On MRI, the most common enhancement pattern seen with TNBC is rim enhancement:
MRI findings following neoadjuvant chemotherapy (NAC):
Correlate well with the extent of residual tumor
MRI provides a reliable baseline prior to NAC and can predict response more sensitively than other imaging methods
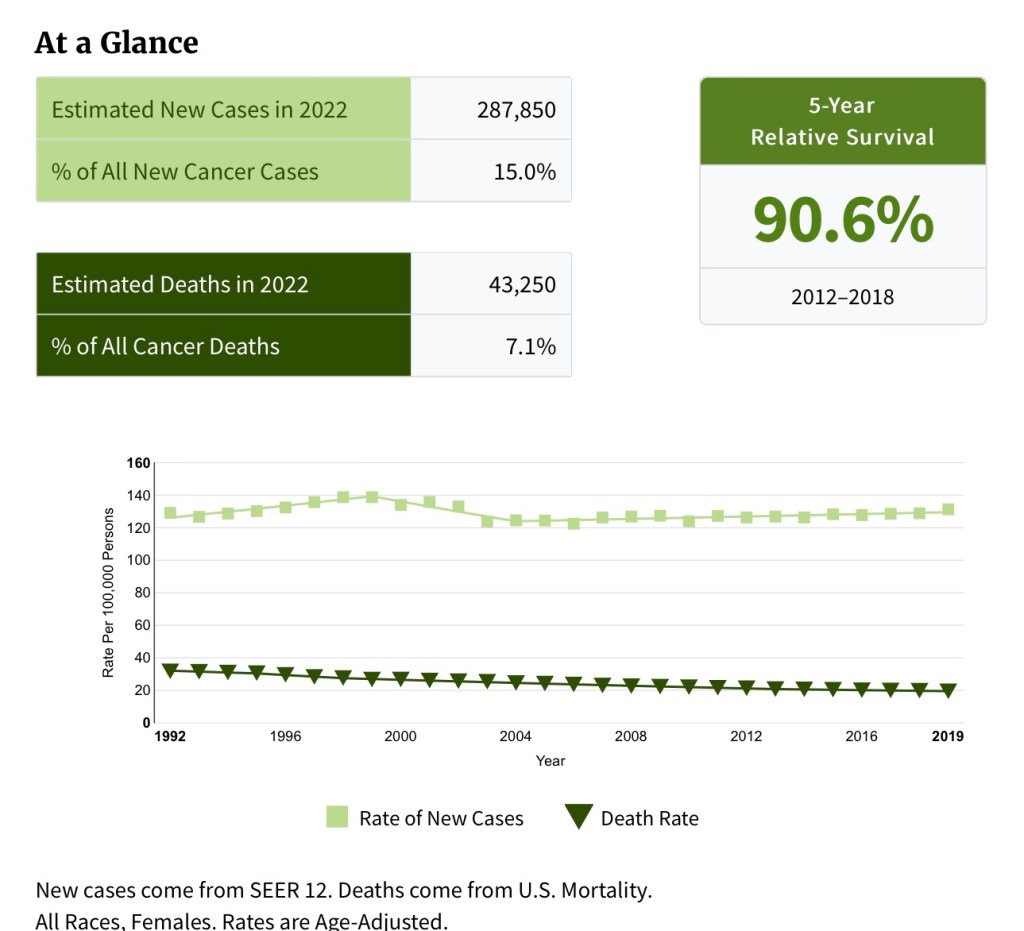
Breast cancer is the most common cancer in women in the United States and worldwide:
It is estimated that there will be 287, 850 cases of breast cancer in women in the United States in 2022:
15% of all new cancer cases
It is estimated that there will be 43, 250 deaths from breast cancer in the United States in 2022:
7.1% of all cancer deaths
Globally, breast cancer accounts for:
At least 1.6 million new cases annually
Triple-negative breast cancers (TNBCs) are defined as:
Those that lack expression of the estrogen receptor (ER) and progesterone receptor (PR) and do not overexpresshuman epidermal growth factor 2 receptor (HER2) protein
If staining for ER receptor by immunohistochemistry (IHC):
Is less than 1%:
The tumor is ER negative
The same applies for PR
HER2 negativity is reported if:
Staining by IHC is 0 or 1+ or if IHC is 2+ (equivocal), HER2/CEP17 ratio is less than 2.0, and the HER2 copy number is less than 4 by in situ hybridization
Of all breast cancers:
15% to 20% are of TNBC variety
The prevalence of TNBC is highest in:
Premenopausal African American women:
39% of all African Americanwomen diagnosed with breast cancer have TNBC:
Compared with 15% of the same age group of non–African American women
It is estimated that African American women are threefold more likely to have TNBC than Caucasian women
Analysis of the US Surveillance, Epidemiology, and End Results database in 2010 showed that:
African American and Hispanic women were more likely to be diagnosed with TNBC than Caucasian women
Overall, TNBC is associated with a:
Poor prognosis and higher risk of distant recurrence and death:
Within the first 5 years after diagnosis compared with other subtypes
The peak risk of recurrence in TNBC:
Occurs within 3 years of diagnosis
TNBC is associated with a:
Shortened disease-free survival (DFS) and in the metastatic setting, a more aggressive clinical course
Visceral metastases are more common with TNBC than hormone receptor–positive tumors:
Common sites of metastasis include the:
Lung, liver, and brain
15% of patients with TNBC develop brain metastases
The median survival of metastatic TNBC (mTNBC):
Is only 13 months
Radosa and colleagues:
Did not find young age to be an independent prognostic factor for outcome in TNBC
When comparing patients aged less than 40 years with those aged 40 years or older:
Age was not found to be independently associated with local recurrence, distant recurrence, DFS, or breast cancer–specific survival
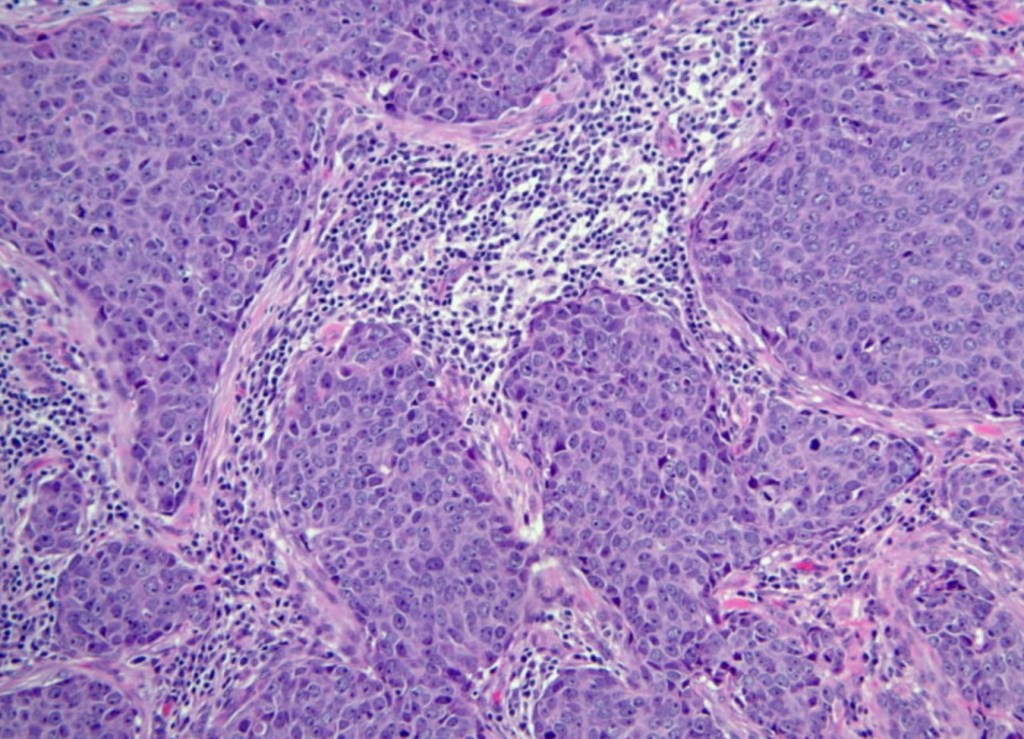
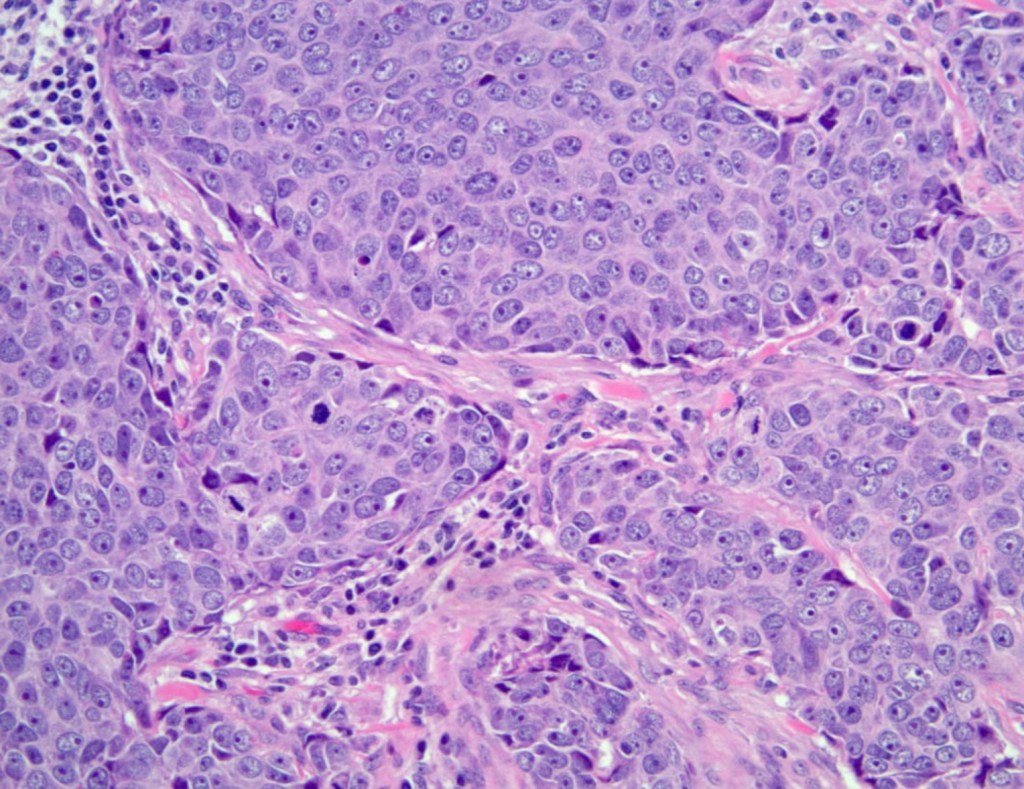
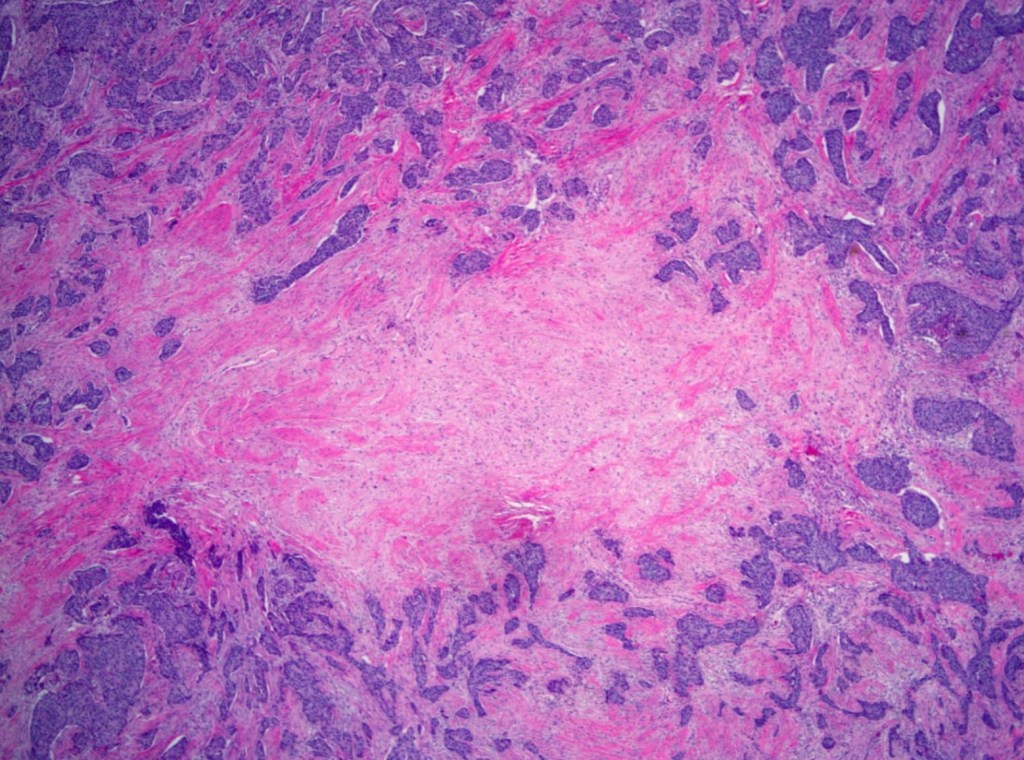
Histologically, TNBCs are most often of:
Higher grade
Exhibit tumor necrosis
Have more frequent nodal metastases
The majority of TNBCs are of:
Invasive ductal breast cancer, no special type:
Characterized by:
High mitotic indices
Presence of central necrotic or fibrotic zones
Pushing borders
Conspicuous lymphatic infiltrate
Typical or atypical medullary features
However, TNBC can be heterogeneous, with a subset of TNBCs of lower grade, including those of the:
Secretory
Adenoid cystic
Acinic cell
Apocrine varieties
Photomicrograph of TNBC showing tumor infiltrating lymphocytesPhotomicrograph of TNBC showing high-grade nuclei, mitotic activity, basaloid morphologyPhotomicrograph of TNBC showing central fibrotic focus
Perou and colleagues divided breast cancers into distinct subtypes by microarray analysis:
ER+ or luminal-like
Basal-like
Erb-B2+
Normal breast
The commercially available prediction analysis of microarray 50 (PAM50) assay by Prosigna® NanoString Technologies can be used to classify tumors into one of four subtypes:
Luminal A
Luminal B
HER2-enriched
Basal-like
TNBCs share many characteristics with basal-like cancers:
However, the terms are not synonymous
About 75% of TNBCs are classified as:
Basal-like based on PAM50 profiling
A recent analysis of 868 TNBCs showed that:
86.1% basal-like
9.1% HER2-enriched
3.2% luminal B
1.6% luminal A
Among TNBC patients:
Intrinsic subtype identified by PAM50 testing:
Has not been correlated with differences in clinical outcome
There is increasing evidence that not all TNBCs have the same behavior, and in fact:
TNBCs comprise a very heterogeneous group of tumors
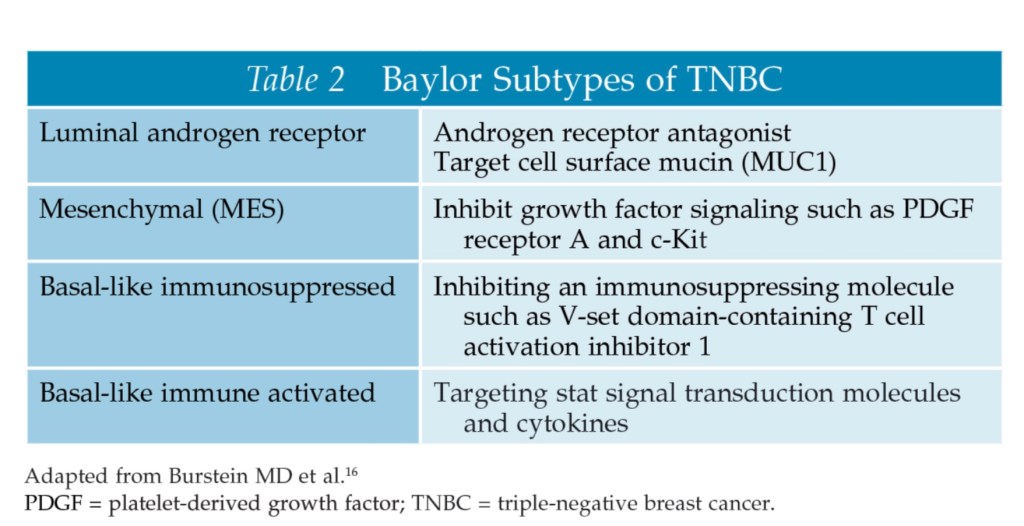
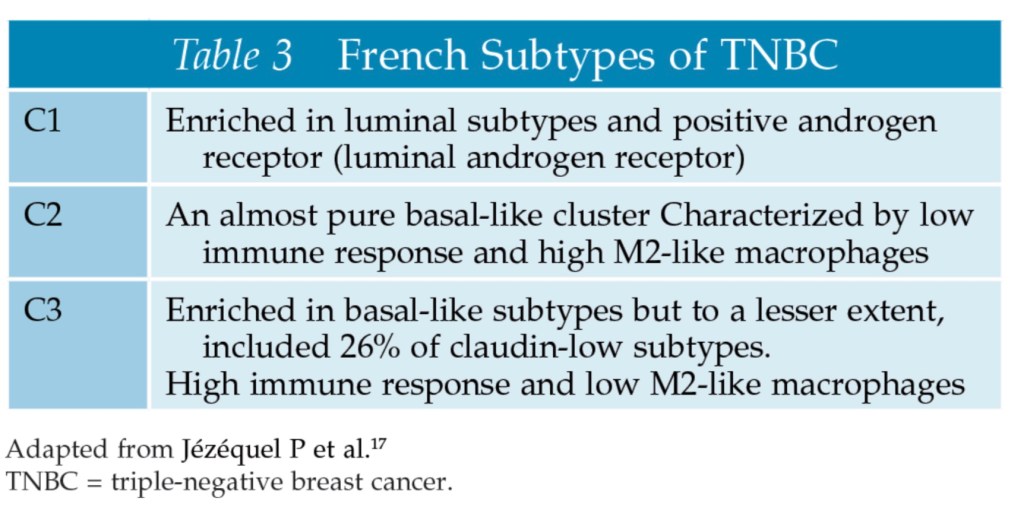
Several emerging paradigms have attempted to define TNBC heterogeneity:
Groups from Vanderbilt, Baylor, and France have divided TNBC into subtypes based on K means clustering, non-negative matrix factorization, and fuzzy clustering, respectively
The subtypes identified by the Vanderbilt group (K means clustering) and possible mechanism of action of effective chemotherapy regimens based on subtype are shown in Table:
Researchers from Baylor (non-negative matrix factorization) and France (fuzzy clustering) also recognized the heterogeneity of TNBC; however, the subtypes they described differed from the Vanderbilt group as shown in Tables:
The Vanderbilt researchers have further refined their six original subtypes into four:
BL1
BL2
M
LAR
They recognized that the:
IM subtype reflected a high percentage of tumor-infiltrating lymphocytes
The MSL subtype higher tumor-associated stromal cell content
The value of identification of subtypes with differing behavior is in the potential for targeted therapy:
For example, 10% to 35% of TNBCs are androgen receptor (AR) positive
At the American Society of Clinical Oncology (ASCO) Annual Meeting in 2017, Quist and colleagues presented another classification schema for TNBC based on transcriptomic and genomic data – CONEXIC:
The CONEXIC four-gene decision tree classified TNBC into six subtypes:
The MC6 subtype was genomically unstable and immune activated:
This subtype appeared responsive to platinum chemotherapy
Other CONEXIC subtypes require further characterization
Although all the classification systems mentioned above provide an intriguing insight into the biology of TNBC, they have not yet transitioned from the research realm into practice to guide clinical decision-making
TNBCs that are AR negative have been termed quadruple-negative breast cancer (QNBC):
The presence or absence of luminal AR varies according to race:
With QNBC being more likely to be found in African American women than in Caucasian women
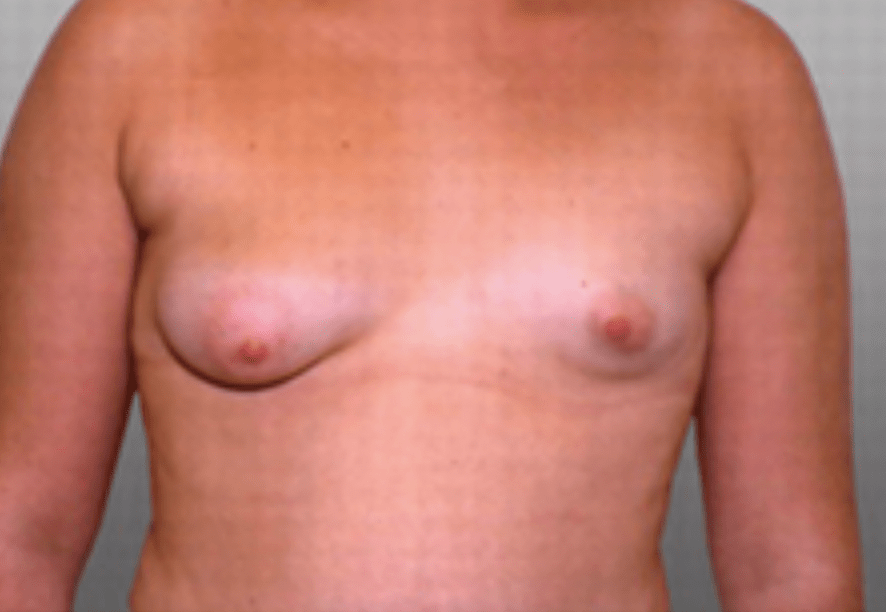
And is associated with thoracic and upper extremity anomalies
Is a rare chest wall deformity consisting of:
Unilateral chest wall hypoplasia and unilateral upper limb deformity
There can be:
Absence or hypoplasia of the breast
Absent pectoralis major or minor muscle
Absent nipple
Absent costal cartilages
Rib abnormalities
Upper limb deformities including:
Syndactyly
Micromelia
Brachydactyly
This rare disease affects men three times more commonly than women
There is no increased risk of breast cancer with Poland syndrome:
Although there is an association with:
Hodgkins lymphoma and leukemia
Most cases are sporadic:
There is no inheritance pattern or known genetic cause:
Genetic testing or high-risk screening for breast cancer is not warranted
Poland syndrome is thought to occur due to:
A vascular malformation resulting in reduced blood flow during embryogenesis:
An interruption of the embryonic blood supply to the subclavian artery:
At the 6th week of embryonic development
The defects can be corrected surgically:
Repair can include:
Reconstruction of anaplastic ribs:
Using bone grafts or prosthetic mesh
Muscle flaps such as latissimus dorsi flap to correct muscle hypoplasia
Breast implants or autologous fat grafting for breast hypoplasia
References:
Kulkarni D, Dixon JM. Congenital abnormalities of the breast. Women’s Health. 2012;8(1):75–88.
Baldelli I, Santi P, Dova L, Cardoni G, Ciliberti R, Franchelli S, Merlo DF, et al. Body image disorders and surgical timing in patients affected by Poland Syndrome: data analysis of 58 case studies. Plast Reconstr Surg. 2016;137(4):1273-1282.
Fokin AA, Robicsek F. Poland’s syndrome revisited. Ann Thorac Surg. 2002:74(6),2218–2225.
Mojallal A, La Marca S, Shipkov C, Sinna R, Braye F. Poland Syndrome and breast tumor: a case report and review of the literature. Aesthet Surg J. 2012;32(1):77–83.
National Human Genome Research Institute website. About Poland anomaly. 2012. http://www.genome.gov/14514230. Accessed January 10, 2020.
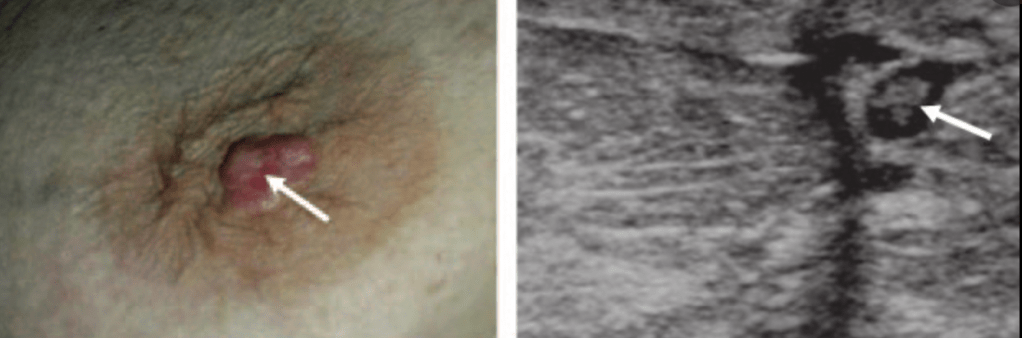
But usually present as a mass visualized on the nipple:
It can become ulcerated and caused bleeding
Nipple adenomas also can be associated with:
Nipple discharge
Pain
Loss of nipple tissue
Often confusing the diagnosis with Paget’s Disease or eczema
Topical steroids:
Are not recommended for the treatment of a nipple adenoma
Despite their benignity:
Complete surgical resection to a negative margin is recommended:
Because they can be associated with atypia or ductal carcinoma in situ
Nipple resection is not necessary:
If the adenoma can be removed with a negative surgical margin
Breast MRI is not indicated for the diagnosis of a nipple adenoma
References:
Stone K, Wheeler A. A review of anatomy, physiology, and benign pathology of the nipple. Ann SurgOncol. 2015;22(10):3236-3240.
Wang C, Wang X, Ma R. Diagnosis and surgical treatment of nipple adenoma. ANZ J Surg.2015;85(6):444-447.
Jones MW, Tavassoli FA. Coexistence of nipple duct adenoma and breast carcinoma: a clinicopathologic study of five cases and review of the literature. Mod Pathol. 1995;8(6):633–636.
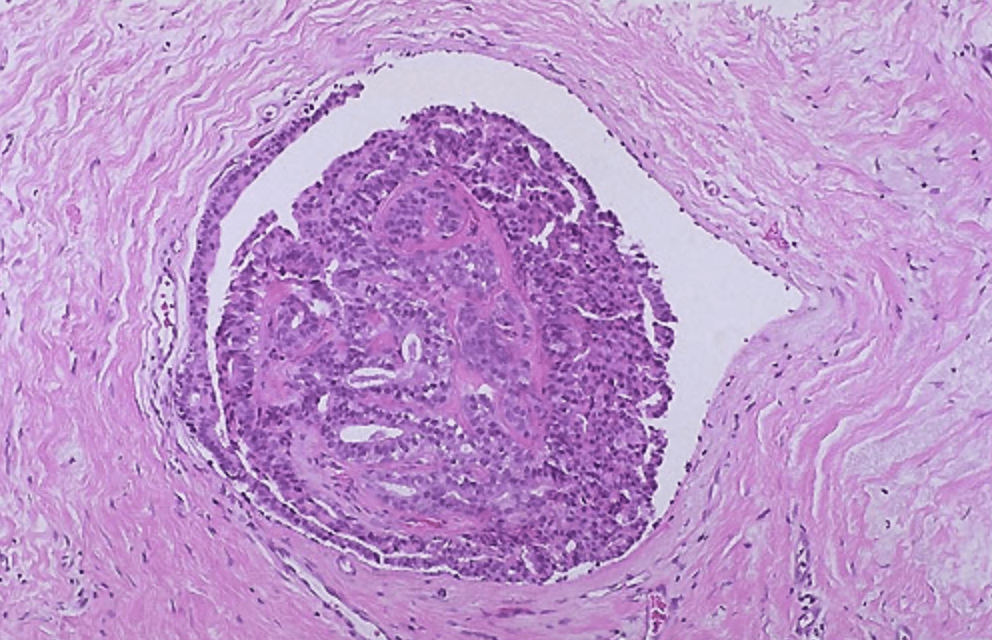
Although a solitary intraductal papilloma is benign:
When a papillary lesion with atypia is identified on core biopsy:
Surgical excisional biopsy is recommended to rule out an associated in situ or invasive cancer:
Studies have demonstrated an upstage rate of 22% to 67% when atypia is present:
But only 3%to 9% in the absence of atypia
MRI is available as an additional diagnostic tool:
A negative MRI would not obviate the need for excisional biopsy to exclude malignancy since it cannot reliably distinguish benign from malignant papillomas
A short-term follow-up could be considered appropriate:
For an intraductal papilloma without atypia on core biopsy if these findings are considered concordant with the clinical presentation
References:
Ahmadiyeh N, Stoleru MA, Raza S, Vester SC, Golshan M. Management of intraductal papilloma of the breast: an analysis of 129 cases and their outcome. Ann Surg Oncol. 2009;16(8):2264-2269.
Jaffer S, Nagi C, Bleiweiss IJ. Excision is indicated for intraductal papilloma of the breast diagnosed on core needle biopsy. Cancer. 2009;115(13):2837-2843.
Syndnor MK, Wilson JD, Hijaz TA, Massey HD, Shaw de Paredes ES. Underestimation of the presence of breast carcinoma in papillary lesions initially diagnosed at core-needle biopsy. Radiology. 2007;242(1):58-62.
McGhan LJ, Pockaj BA, Wasif N, Giurescu ME, McCullough AE, Gray RJ. Papillary lesions on core breast biopsy: excisional biopsy for all patients? Am Surg. 2013;79(12):1238-1242.
Holley SO, Appleton CM, Farria DM, Reichert VC, Warrick J, Allred DC, Monsees BS. Pathologic outcomes of nonmalignant papillary breast lesions diagnosed at imaging-guided core needle biopsy. Radiology. 2012;265(2):379-384.