- Breast cancer is the most common cancer in women in the United States and worldwide:
- It is estimated that there will be 287, 850 cases of breast cancer in women in the United States in 2022:
- 15% of all new cancer cases
- It is estimated that there will be 43, 250 deaths from breast cancer in the United States in 2022:
- 7.1% of all cancer deaths
- Globally, breast cancer accounts for:
- At least 1.6 million new cases annually
- It is estimated that there will be 287, 850 cases of breast cancer in women in the United States in 2022:
- Triple-negative breast cancers (TNBCs) are defined as:
- Those that lack expression of the estrogen receptor (ER) and progesterone receptor (PR) and do not overexpress human epidermal growth factor 2 receptor (HER2) protein
- If staining for ER receptor by immunohistochemistry (IHC):
- Is less than 1%:
- The tumor is ER negative
- Is less than 1%:
- The same applies for PR
- If staining for ER receptor by immunohistochemistry (IHC):
- HER2 negativity is reported if:
- Staining by IHC is 0 or 1+ or if IHC is 2+ (equivocal), HER2/CEP17 ratio is less than 2.0, and the HER2 copy number is less than 4 by in situ hybridization
- Those that lack expression of the estrogen receptor (ER) and progesterone receptor (PR) and do not overexpress human epidermal growth factor 2 receptor (HER2) protein
- Of all breast cancers:
- 15% to 20% are of TNBC variety
- The prevalence of TNBC is highest in:
- Premenopausal African American women:
- 39% of all African American women diagnosed with breast cancer have TNBC:
- Compared with 15% of the same age group of non–African American women
- It is estimated that African American women are threefold more likely to have TNBC than Caucasian women
- Analysis of the US Surveillance, Epidemiology, and End Results database in 2010 showed that:
- African American and Hispanic women were more likely to be diagnosed with TNBC than Caucasian women
- 39% of all African American women diagnosed with breast cancer have TNBC:
- Premenopausal African American women:
- Overall, TNBC is associated with a:
- Poor prognosis and higher risk of distant recurrence and death:
- Within the first 5 years after diagnosis compared with other subtypes
- The peak risk of recurrence in TNBC:
- Occurs within 3 years of diagnosis
- Poor prognosis and higher risk of distant recurrence and death:
- TNBC is associated with a:
- Shortened disease-free survival (DFS) and in the metastatic setting, a more aggressive clinical course
- Visceral metastases are more common with TNBC than hormone receptor–positive tumors:
- Common sites of metastasis include the:
- Lung, liver, and brain
- 15% of patients with TNBC develop brain metastases
- Lung, liver, and brain
- Common sites of metastasis include the:
- The median survival of metastatic TNBC (mTNBC):
- Is only 13 months
- Radosa and colleagues:
- Did not find young age to be an independent prognostic factor for outcome in TNBC
- When comparing patients aged less than 40 years with those aged 40 years or older:
- Age was not found to be independently associated with local recurrence, distant recurrence, DFS, or breast cancer–specific survival
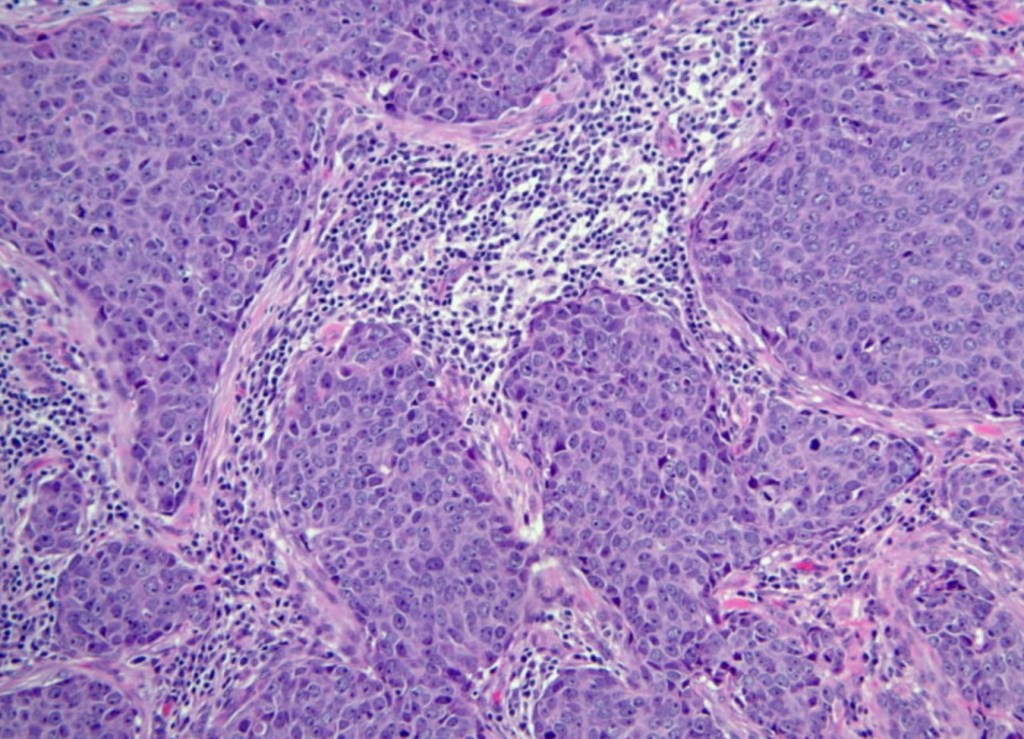
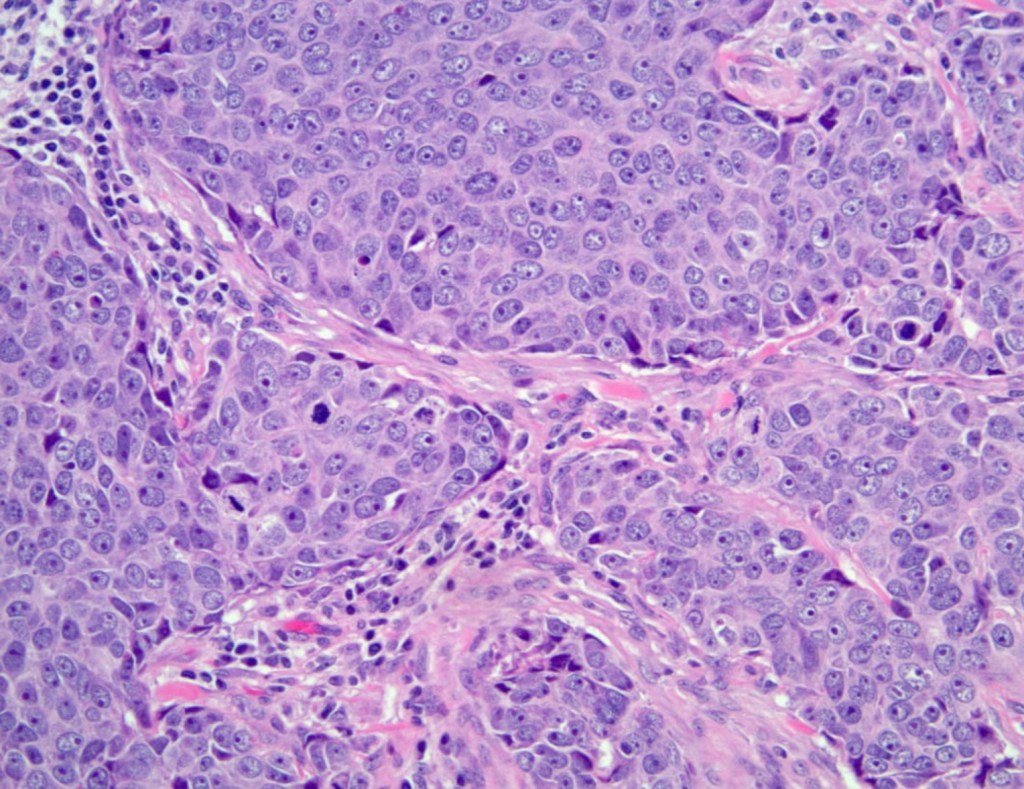
- Histologically, TNBCs are most often of:
- Higher grade
- Exhibit tumor necrosis
- Have more frequent nodal metastases
- The majority of TNBCs are of:
- Invasive ductal breast cancer, no special type:
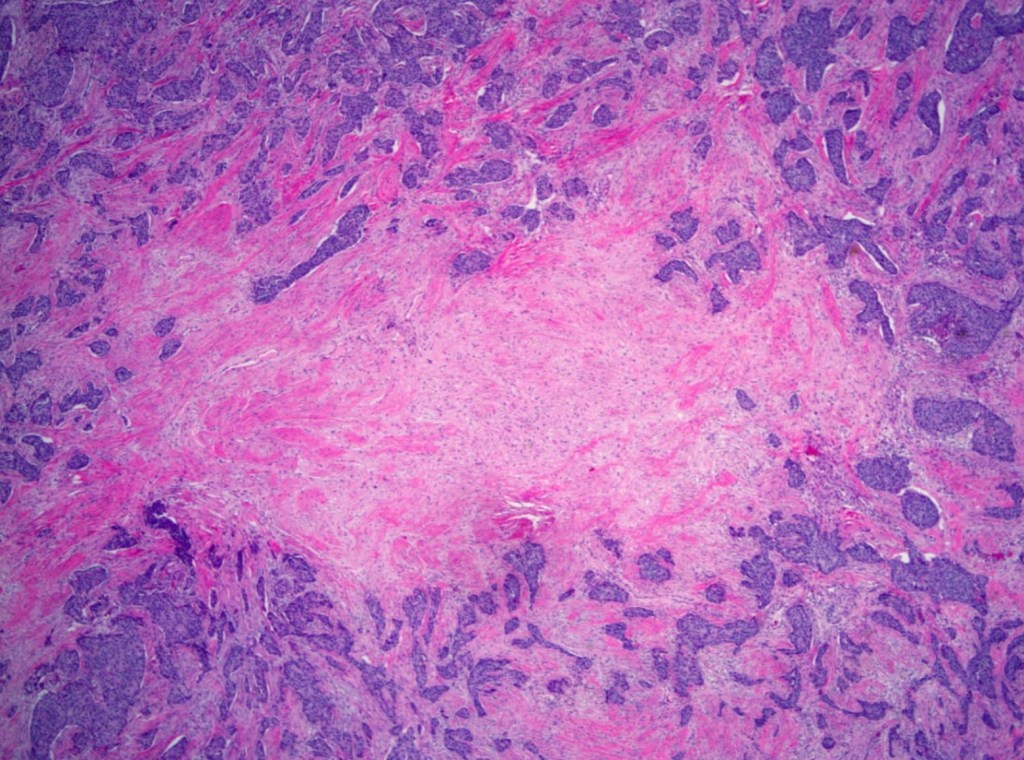
- Characterized by:
- High mitotic indices
- Presence of central necrotic or fibrotic zones
- Pushing borders
- Conspicuous lymphatic infiltrate
- Typical or atypical medullary features
- Characterized by:
- However, TNBC can be heterogeneous, with a subset of TNBCs of lower grade, including those of the:
- Secretory
- Adenoid cystic
- Acinic cell
- Apocrine varieties
- Invasive ductal breast cancer, no special type:
- Perou and colleagues divided breast cancers into distinct subtypes by microarray analysis:
- ER+ or luminal-like
- Basal-like
- Erb-B2+
- Normal breast
- The commercially available prediction analysis of microarray 50 (PAM50) assay by Prosigna® NanoString Technologies can be used to classify tumors into one of four subtypes:
- Luminal A
- Luminal B
- HER2-enriched
- Basal-like
- TNBCs share many characteristics with basal-like cancers:
- However, the terms are not synonymous
- About 75% of TNBCs are classified as:
- Basal-like based on PAM50 profiling
- A recent analysis of 868 TNBCs showed that:
- 86.1% basal-like
- 9.1% HER2-enriched
- 3.2% luminal B
- 1.6% luminal A
- Among TNBC patients:
- Intrinsic subtype identified by PAM50 testing:
- Has not been correlated with differences in clinical outcome
- Intrinsic subtype identified by PAM50 testing:
- There is increasing evidence that not all TNBCs have the same behavior, and in fact:
- TNBCs comprise a very heterogeneous group of tumors
- Several emerging paradigms have attempted to define TNBC heterogeneity:
- Groups from Vanderbilt, Baylor, and France have divided TNBC into subtypes based on K means clustering, non-negative matrix factorization, and fuzzy clustering, respectively
- The subtypes identified by the Vanderbilt group (K means clustering) and possible mechanism of action of effective chemotherapy regimens based on subtype are shown in Table:

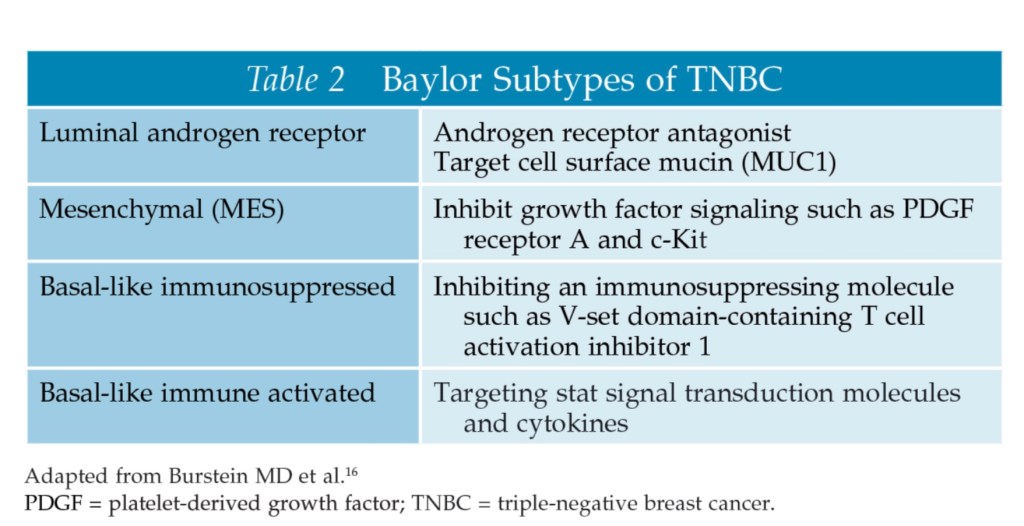
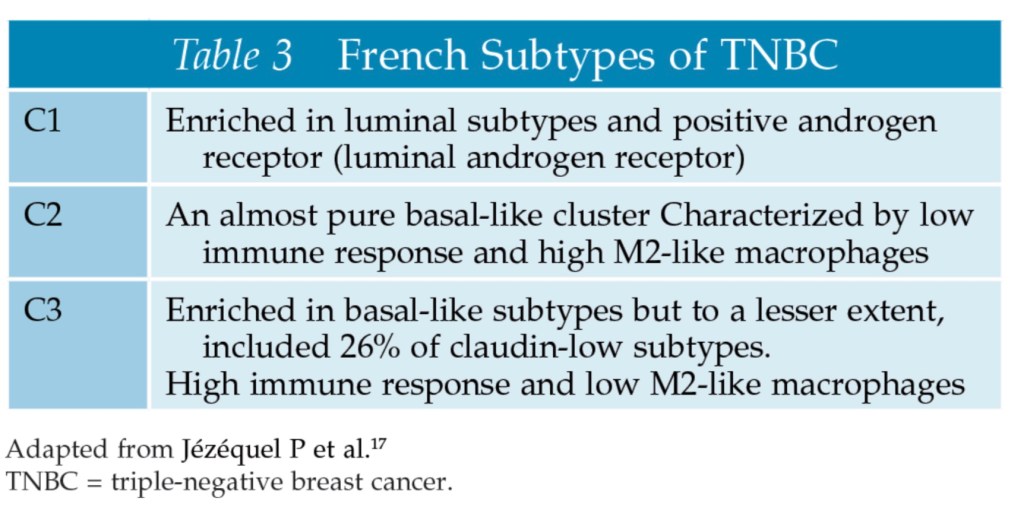
- Researchers from Baylor (non-negative matrix factorization) and France (fuzzy clustering) also recognized the heterogeneity of TNBC; however, the subtypes they described differed from the Vanderbilt group as shown in Tables:
- The Vanderbilt researchers have further refined their six original subtypes into four:
- BL1
- BL2
- M
- LAR
- They recognized that the:
- IM subtype reflected a high percentage of tumor-infiltrating lymphocytes
- The MSL subtype higher tumor-associated stromal cell content
- The value of identification of subtypes with differing behavior is in the potential for targeted therapy:
- For example, 10% to 35% of TNBCs are androgen receptor (AR) positive
- At the American Society of Clinical Oncology (ASCO) Annual Meeting in 2017, Quist and colleagues presented another classification schema for TNBC based on transcriptomic and genomic data – CONEXIC:
- The CONEXIC four-gene decision tree classified TNBC into six subtypes:
- The MC6 subtype was genomically unstable and immune activated:
- This subtype appeared responsive to platinum chemotherapy
- Other CONEXIC subtypes require further characterization
- The MC6 subtype was genomically unstable and immune activated:
- The CONEXIC four-gene decision tree classified TNBC into six subtypes:
- Although all the classification systems mentioned above provide an intriguing insight into the biology of TNBC, they have not yet transitioned from the research realm into practice to guide clinical decision-making
- TNBCs that are AR negative have been termed quadruple-negative breast cancer (QNBC):
- The presence or absence of luminal AR varies according to race:
- With QNBC being more likely to be found in African American women than in Caucasian women
- The presence or absence of luminal AR varies according to race:
- TNBCs that are AR negative have been termed quadruple-negative breast cancer (QNBC):
#Arrangoiz #CancerSurgeon #BreastSurgeon #SurgicalOncologist #ComplexSurgicalOncology #BreastCancer #TripleNegativeBreastCancer #TNBC #Miami #Mexico #Teacher #Surgeon #MountSinaiMedicalCenter #MSMC
