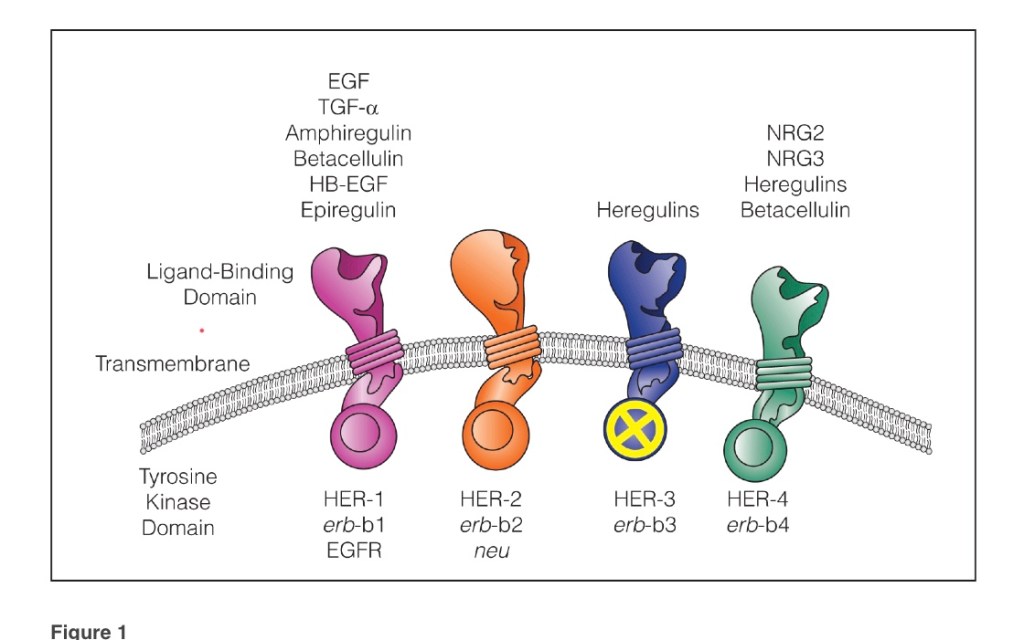
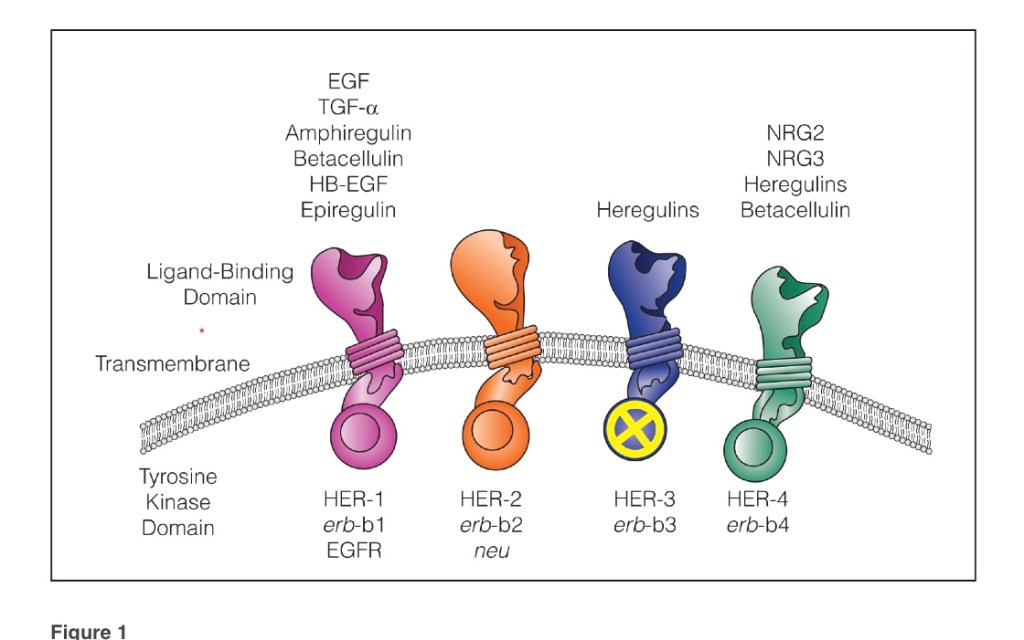
– These proteins are made up of an extracellular ligand-binding domain, a membrane-spanning region, and a cytoplasmic domain with tyrosine kinase activity
The evaluation of HER-2 is recommended in all cases of breast cancer at the time of initial diagnosis and / or at the time of recurrence to guide therapy
A number of methods are used for HER-2 testing including:
Immunohistochemistry (IHC)
Florescence in situ hybridization (FISH)
Enzyme-linked immunosorbent assay (ELISA) analysis of serum and tumor
Western blot
Southern blot
Chromogenic in situ hybridization (CISH)
Silver in situ hybridization (SISH)
Polymerase chain reaction (PCR)
IHC and FISH:
Are currently the main testing modalities for HER-2-positive breast cancer
HER-2 expression in breast cancer:
Is primarily assessed semiquantitatively by IHC
The 2013 American Society of Clinical Oncology (ASCO) and the College of American Pathologists (CAP) guidelines:
Outline an IHC scoring method based on four classes:
0, 1+, 2+, and 3+
A score of 0 is negative:
Indicating no observed staining in invasive tumor cells
A score of 1+ is negative:
Indicates:
Weak, incomplete membrane staining in any proportion of invasive tumor cells or
Weak, complete membrane staining in less than 10% of invasive tumor cells
A score of 2+ is equivocal:
Indicating:
Circumferential membrane staining that is incomplete and / or
Weak / moderate and in more than 10% of invasive tumor cells or
Complete and circumferential membrane staining that is intense and in 10% or less of invasive tumor cells
All 2+ equivocal cases undergo subsequent testing by FISH
A score of 3+ is positive:
Indicates circumferential membrane staining that is complete and intense in a homogeneous and contiguous population, present in more than 10% of invasive tumor cells, and readily appreciated using a low-power objective
FISH:
Is a sensitive and accurate method of scoring invasive breast tumor tissue for HER-2 expression
Initial gene amplification studies by FISH assessment:
Used chromosome 17 centromere (CEP17) or another gene on the same chromosome as an internal control:
With a ratio of 2.0 or greater:
Considered evidence of HER-2 amplification
These criteria were used as the cutoff for enrollment in trials evaluating HER-2 targeted therapies
In 2007, the ASCO / CAP guidelines were changed to define HER-2 amplified:
As a ratio of 2.2 or greater
More recent guidelines:
Have changed the ratio cutoff back to a ratio of 2.0 or greaterwith the inclusion of criteria to account for HER-2 copy number per tumor cell
Based on the recent guidelines, HER-2 is amplified in cases where the:
HER-2 / CEP17 ratio is 2.0 or greater with an average HER-2 copy number of more than 4.0 signals/cell or
HER-2 / CEP17 ratio is less than 2.0 with an average HER-2 copy number of 6.0 or more signals / cell using a dual probe or a HER-2 copy number of 6.0 or more copies/cell using a single probe
FISH testing is negative for HER-2 amplification with a:
HER-2 / CEP17 ratio of less than 2.0 with an average HER-2 copy number of less than 4.0 signals/cell or an average HER-2 copy number of less than 4.0 signals / cell using a single probe
– Ligand binding to the HER receptors leads to their homodimerization or heterodimerization, which promotes signal transduction
– To date, no ligands have been identified for the HER-2 receptor
– However, the HER-2 receptor has been shown to be the preferred heterodimerization for other HER family members
– HER-2 has been shown to be one of the most important oncogenes in human breast cancer
– HER-2 complexes initiate intracellular signaling via the mitogen-activated protein kinase (MAPK), phosphatidylinositol 3-kinase (PI3K), and phospholipase C pathways
– Breast cancer cells and model tumor systems, have shown that over expression of the gene has been associated with increased mitogenesis, malignant transformation, increased cell motility, invasion, and metastasis
– In human breast cancer, amplification of the gene is found in around 15% to 30% of primary invasive breast tumors
– In these cases, up to 100 copies have been demonstrated per cell, which is equivalent to a 50-fold increase in gene copy number per cell
– As a result, the number of receptors per cell is increased up to 2 million
– Overexpression at the messenger RNA or protein level occurs in around 15% to 30% of patients with early-stage breast cancer
The HER gene family. The proteins are made up of an extracellular ligand-binding domain, a membrane-sparing region, and a cytoplasmic domain with tyrosine kinase activity. Note that HER-2 has no known ligands. Also note that HER-3 has no intrinsic tyrosine kinase activity.
All patients with HER-2 positive breast cancer patients:
Who require systemic therapy should complete one year of HER2-targeted therapy:
Including those who achieve pathologic complete response after neoadjuvant chemotherapy
One could also consider continuing adjuvant pertuzumab in addition to trastuzumab:
Based on results from the phase III Aphinity trial:
Although patients who received neoadjuvant chemotherapy were not included in this trial
For patients who have residual disease and do not achieve complete pathologic response at the time of surgery:
Completion of one year of T-DM1 decreased the risk of recurrence of invasive breast cancer or death by 50% than with trastuzumab alone:
Based on results from KATHERINE trial:
The estimated percentage of patients who were free of invasive disease at 3 years was:
88.3% in the T-DM1 group and 77.0% in the trastuzumab group
References:
von Minckwitz G, Procter M, de Azambuja E, Zardavas D, Benyunes M, Viale G, et al. Adjuvant Pertuzumab and Trastuzumab in early HER2-positive breast cancer N Engl J Med. 2017;377(2):122-131.
von Minckwitz G, Huang CS, Mano MS, Loibl S, Mamounas EP, Untch M, et al. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N Engl J Med. 2019;380(7):617-628.
– Breast cancer is mainly hormonally driven, with around 70% of cancers expressing the estrogen receptor (ER)
– A number of other peptide growth factors and their receptors, namely members of the receptor tyrosine kinase family, have been implicated in normal breast development and in carcinogenesis
– Amplification of the human epidermal growth factor receptor2 (HER-2) gene is found in approximately 15% to 30% of breast cancers
– Historically, HER-2 overexpression has been associated with aggressive disease and poor prognosis
-However, the use of targeted anti-HER-2 therapy has revolutionized the treatment of HER-2-positive disease, and use of the monoclonal antibody trastuzumab in combination with chemotherapy is now standard of care for tumors greater than 1 cm in size and in node-positive disease
– More recently, the value of dual-agent anti-HER-2 therapy has been demonstrated in large clinical trials
Who require systemic therapy should complete one year of HER2-targeted therapy:
Including those who achieve pathologic complete response after neoadjuvant chemotherapy
One could also consider continuing adjuvant pertuzumab in addition to trastuzumab:
Based on results from the phase III Aphinity trial:
Although patients who received neoadjuvant chemotherapy were not included in this trial
For patients who have residual disease and do not achieve complete pathologic response at the time of surgery:
Completion of one year of T-DM 1(ado trastuzumab-emtansine) decreased the risk of recurrence of invasive breast cancer or death:
By 50% than with trastuzumab alone:
Based on results from KATHERINE trial:
The estimated percentage of patients who were free of invasive disease at 3 years was:
88.3% in the T-DM1 group
77.0% in the trastuzumab group
Metastatic hormone receptor negative, HER positive breast cancer:
The CLEOPATRA study:
Showed that the combination of docetaxel, trastuzumab, and pertuzumab led to improved progression free survival (PFS) compared to docetaxel, trastuzumab, and placebo:
18.5 months vs. 12.4 months
Neoadjuvant chemotherapy (NAC):
Is appropriate for many patients with locally advanced breast cancer regardless of subtype:
Because a response may allow both:
Less extensive surgery and improved surgical outcomes
Locally advanced disease is defined as stage III cancers, as well as the subset of IIB cancers with T3 disease
In addition, patients with earlier stage, HER2+ disease (stage I or II):
May also be candidates for neoadjuvant therapy, if one or more of the following criteria apply:
The patient desires breast-conserving surgery (BCS) but is not a candidate for BCS or is likely to have a suboptimal cosmetic outcome with BCS due to tumor location or size relative to the size of the patient’s breast, and may be a better candidate if neoadjuvant therapy decreases the extent of her tumor
The patient has limited axillary nodal involvement (N1), for which axillary lymph node dissection would be standard surgical management, but could be a candidate for sentinel lymph node sampling alone if converted to node-negative disease with neoadjuvant therapy
Surgery must be postponed awaiting:
consultation with plastic surgery regarding breast reconstruction
Results of genetic testing
Resolution of an intercurrent illness, including pregnancy, and the patient and treating clinicians do not wish to delay initiation of treatment
Postoperative treatment with ado-trastuzumab emtansine (T-DM1) would be considered if the patient were found to have residual invasive disease in the breast or axillary nodes following NAC with single or dual HER2-targeted therapy
Pertuzumab:
Is a monoclonal antibody that binds to a different epitope on HER2 than trastuzumab:
Blocking the formation of HER2 : HER3 heterodimers:
Which is believed to be an important mechanism of resistance to trastuzumab
While single-agent pertuzumab has demonstrated antitumor activity in patients with HER2-positive metastatic disease who progressed on trastuzumab:
It is typically given in combination with trastuzumab to maintain suppression of signaling initiated by HER2 homodimers
In 2013, the FDA granted accelerated approval for the addition of pertuzumab to NACT and trastuzumab for patients with:
HER2+ locally advanced, inflammatory, or early-stage (either greater than 2 cm in diameter or node positive) breast cancer
I routinely recommend adding pertuzumab in patients receiving NACT and trastuzumab:
Given evidence that pertuzumab enhances locoregional responses:
Even though it increases the incidence and severity of treatment-related diarrhea as well as modestly increasing the frequency of hematologic toxicities
NeoSphere trial:
In the phase II NeoSphere trial, 417 HER2+ patients received 12 weeks of neoadjuvant therapy:
Composed of either:
Four cycles of single-agent docetaxel with trastuzumab, pertuzumab, or both, or
The combination of trastuzumab and pertuzumab without concurrent docetaxel
After surgery, all patients received anthracycline-based adjuvant chemotherapy:
Those randomized to trastuzumab and pertuzumab alone also received adjuvant docetaxel)
Completed a year of treatment with trastuzumab
Those randomly assigned to docetaxel with pertuzumab and trastuzumab had a higher pathologic complete response (pCR) rate (46%)compared with those receiving docetaxel with just trastuzumab (29%)or just pertuzumab (24%)
Patients receiving pertuzumab and trastuzumab without docetaxel had a pCR rate of 17%
References:
Hayes DF. HER2 and breast cancer — a phenomenal success story. N Engl J Med. 2019;381(13):1284-1286.
Gianni L, Pienkowski T, Im Y-H, Tseng LM, Liu MC, Lluch A, et al. 5-Year analysis of neoadjuvant pertuzumab and trastuzumab in patients with locally advanced, inflammatory, or early-stage HER2-positive breast cancer (NeoSphere): a multicentre, open-label, phase 2 randomised trial. Lancet Oncol. 2016;17(6):791-800.
von Minckwitz G, Procter M, de Azambuja E, Zardavas D, Benyunes M, Viale G, et al. Adjuvant Pertuzumab and Trastuzumab in early HER2-positive breast cancer N Engl J Med. 2017;377(2):122-131.
von Minckwitz G, Huang CS, Mano MS, Loibl S, Mamounas EP, Untch M, et al. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N Engl J Med. 2019;380(7):617-628.
Baselga J, Cortés J, Kim SB, Im SA, Hegg R, Im YH, et al. Pertuzumab plus trastuzumab plus docetaxel for metastatic breast cancer. New Engl J Med. 2012;366(2):109-119.
Swain SM, Baselga J, Kim SB, Ro J, Semiglazov V, Campone M, et al. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N Engl J Med. 2015;372(8):724-734.
Special attention should be given to sampling and pathologic review of the ovaries and fallopian tubes
Typically between 35 and 40 years, and upon completion of child bearing
Because ovarian cancer onset in patients with BRCA2 pathogenic / likely pathogenic variants is an average of 8 to 10 years later than in patients with BRCA1 pathogenic / likely pathogenic variants:
It is reasonable to delay RRSO for management of ovarian cancer risk:
Until age 40 to 45 years in patients with BRCA2 pathogenic / likely pathogenic variants unless age at diagnosis in the family warrants earlier age for consideration of prophylactic surgery.
Counseling includes a discussion of:
Reproductive desires
Extent of cancer risk
Degree of protection for breast and ovarian cancer
Management of menopausal symptoms
Hormone replacement therapy, and related medical issues
Salpingectomy alone is not the standard of care for risk reduction, although clinical trials of interval salpingectomy and delayed oophorectomy are ongoing:
The concern for risk-reducing salpingectomy alone is that women are still at risk for developing ovarian cancer
In addition, in premenopausal women, oophorectomy likely reduces the risk of developing breast cancer but the magnitude is uncertain and may be gene-specific
Limited data suggest that there may be a slightly increased risk of serous uterine cancer among women with a BRCA1 pathogenic / likely pathogenic variant.
The clinical significance of these findings is unclear
Further evaluation of the risk of serous uterine cancer in the BRCA population needs to be undertaken
The provider and patient should discuss the risks and benefits of concurrent hysterectomy at the time of RRSO for women with a BRCA1 pathogenic / likely pathogenic variant prior to surgery
Women who undergo hysterectomy at the time of RRSO are candidates for estrogen alone hormone replacement therapy, which is associated with a decreased risk of breast cancer compared to combined estrogen and progesterone, which is required when the uterus is left in situ (Chlebowski R, et al. JAMA Oncol 2015;1:296-305)
Address psychosocial and quality-of-life aspects of undergoing risk-reducing mastectomy and /or salpingo-oophorectomy
For those patients who have not elected RRSO:
Transvaginal ultrasound combined with serum CA-125 for ovarian cancer screening:
Although of uncertain benefit, may be considered at the clinician’s discretion starting at age 30 to 35 years
Consider risk reduction agents as options for breast and ovarian cancer, including discussion of risks and benefits
Per American Society of Clinical Oncology / College of American Pathologists (ASCO / CAP) guidelines:
Tumors with an immunohistochemical result of 2+ (equivocal):
HER2 / CEP 17 ratio of > 2.0 and copy number of > 4.0:
Are considered positive
References:
Wolff AC, Hammond MEH, Allison KH, Harvey BE, Mangu PB, Bartlett JMS, et al. Human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline focused update. J Clin Oncol. 2018;142(11):1364-1382.
Lin L, Sirohi D, Coleman JF, Gulbahce HE. American Society of Clinical Oncology/College of American Pathologists 2018 focused update of breast cancer HER2 FISH testing guidelines. results from a National Reference Laboratory. Am J Clin Pathol. 2019;152(4):479-485.
If you’re having thyroid surgery, it’s important to know how to best prepare for your procedure and what to expect while you recover. This includes any tests you’ll need before surgery, as well as what to avoid after surgery to help ensure its success.
How should I prepare for thyroid surgery?
After your thyroidectomy or thyroid lobectomy is scheduled, you’ll have a pre-operative evaluation with members of your thyroid surgery care team. That evaluation may include blood tests, an electrocardiogram (EKG), X-rays or other imaging studies.
We’ll give you specific instructions on when to stop eating, drinking and taking medications prior to surgery. It’s very important that you follow these guidelines for your own safety, and you’ll need to have an empty stomach before any surgical procedure that requires anesthesia. If you don’t follow the instructions, your thyroid surgery might be cancelled. Please contact us with any specific questions.
What is recovery like after thyroid surgery?
After your thyroidectomy or thyroid lobectomy, you may have a temporary sore throat, neck pain, difficulty swallowing or a weak voice.
Your diet will be restricted for the evening of your surgery, but in most cases, it can return to normal the next day.
Before you leave the hospital, we’ll schedule a follow-up appointment, give instructions for your at-home recovery and go over any prescribed medications.
Most people are ready to return home within one day of surgery, but take off about two weeks from work to recover. You’ll need to refrain from heavy lifting or other tasks that can strain your neck for up to three weeks after your surgery. Soaking or scrubbing the site of your incision is also discouraged for at least one week to allow it time to properly heal. Showering is generally allowed after about one day.
Pain at the site of your incision will improve after a few days but may continue for a week or so. If you notice sudden swelling in your neck, which could signify an infection, contact our office.
Due to disturbance of the parathyroid glands, which regulate calcium balance, your calcium level may drop after surgery. If it drops, you may notice numbness and tingling of your fingers or around your mouth. We’ll monitor your calcium levels through blood tests, and give you instructions about taking calcium replacements if needed.
What are the side effects of thyroid surgery?
After a total thyroidectomy, you will take lifelong thyroid hormone replacements. Because your entire thyroid gland is removed, it will no longer supply you with the hormone you need to control your body’s metabolic processes. You might also have to take supplements after thyroidectomy to balance your calcium levels.
After a thyroid lobectomy, you’ll need to have your thyroid hormone levels checked and will be prescribed a thyroid hormone replacement, if needed.
In the weeks after your thyroid surgery, you may have neck pain, soreness of your vocal chords or a weak voice. These symptoms are usually temporary.
Will I need to follow a special diet after thyroid surgery?
For most people, a special diet after a thyroidectomy or thyroid lobectomy isn’t necessary. You’ll likely be able to eat and drink normally the morning after your surgery, but you may prefer softer foods at first. We’ll let you know if and for how long you need to restrict your eating and drinking.
Decrease in ejection fraction in up to 20% of patients:
Although this is often reversible
Trastuzumab:
Can less commonly cause pneumonitis
Pertuzumab:
Can cause rash and diarrhea
References:
Gianni L, Pienkowski T, Im YH, Roman L, Tseng LM, Liu MC, et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, phase 2 trial. Lancet Oncol. 2012;13(1):25-32.
Schneeweiss A, Chia S, Hickish T, Harvey V, Eniu A, Hegg R, et al. Pertuzumab plus trastuzumab in combination with standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer: a randomized phase II cardiac safety study (TRYPHAENA). Ann Oncol. 2013;24(9):2278-2284.