| TX |
Primary tumor cannot be assessed. |
| Tis |
Carcinoma in situ. |
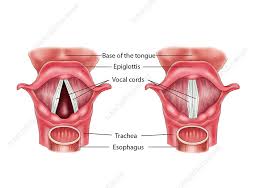
Supraglottis
|
| T1 |
Tumor limited to one subsite of supraglottis with normal vocal cord mobility. |
| T2 |
Tumor invades mucosa of more than one adjacent subsite of supraglottis or glottis or region outside the supraglottis (e.g., mucosa of the base of the tongue, vallecula, medial wall of pyriform sinus) without fixation of the larynx. |
| T3 |
Tumor limited to larynx with vocal cord fixation and/or invades any of the following: post-cricoid area, pre-epiglottic space, para-glottic space, and/or inner cortex of thyroid cartilage. |
| T4 |
Moderately advanced or very advanced. |
| T4a |
Moderately advanced local disease. Tumor invades through the outer cortex of the thyroid cartilage and/or invades tissues beyond the larynx (e.g., trachea, soft tissues of the neck including deep extrinsic muscle of the tongue, strap muscles, thyroid, or esophagus). |
| T4b |
Very advanced local disease. Tumor invades prevertebral space, encases carotid artery, or invades mediastinal structures. |
Glottis
|
| T1 |
Tumor limited to the vocal cord(s) (may involve anterior or posterior commissure) with normal mobility. |
| T1a |
Tumor limited to one vocal cord. |
| T1b |
Tumor involves both vocal cords. |
| T2 |
Tumor extends to supraglottis and/or subglottis, and/or with impaired vocal cord mobility. |
| T3 |
Tumor limited to the larynx with vocal cord fixation and/or invasion of paraglottic space and/or inner cortex of the thyroid cartilage. |
| T4 |
Moderately advanced or very advanced. |
| T4a |
Moderately advanced local disease. Tumor invades through the outer cortex of the thyroid cartilage and/or invades tissues beyond the larynx (e.g., trachea, cricoid cartilage, soft tissues of the neck including deep extrinsic muscle of the tongue, strap muscles, thyroid, or esophagus). |
| T4b |
Very advanced local disease. Tumor invades prevertebral space, encases carotid artery, or invades mediastinal structures. |
Subglottis
|
| T1 |
Tumor limited to the subglottis. |
| T2 |
Tumor extends to vocal cord(s) with normal or impaired mobility. |
| T3 |
Tumor limited to the larynx with vocal cord fixation and/or invasion of paraglottic space and/or inner cortex of the thyroid cartilage. |
| T4 |
Moderately advanced or very advanced. |
| T4a |
Moderately advanced local disease. Tumor invades cricoid or thyroid cartilage and/or invades tissues beyond the larynx (e.g., trachea, soft tissues of the neck including deep extrinsic muscles of the tongue, strap muscles, thyroid, or esophagus). |
| T4b |
Very advanced local disease. Tumor invades prevertebral space, encases carotid artery, or invades mediastinal structures. |