- The incidence of invasive cutaneous melanoma continues to be a major public health concern in the United States:
- Of concern, the rate of melanoma has risen about 3% per year in the United States over the past few decades
- Estimated incidence rates of new melanomas in 2021:
- 106,110:
- Men 62,260
- Women 43,850
- 106,110:
- Estimated mortality rate for melanoma in the year 2021:
- 7,180 people are expected to die of melanoma:
- Men 4,600 men
- Women 2,580 women
- 7,180 people are expected to die of melanoma:
- Melanoma remains more than 20 times more common in:
- Whites than in African Americans
- Overall, the lifetime risk of being diagnosed with melanoma is about:
- 2.5% (1 in 40) for whites
- 0.1%(1 in 1,000) for blacks
- 0.5% (1 in 200) for Hispanics
- The incidence of melanoma has been increasing faster than that of nearly any other cancer over the last 30 years
- The major environmental risk factor:
- Exposure to ultraviolet (UV) radiation:
- Is reflected in geographic and ethnic patterns of melanoma rates
- Exposure to ultraviolet (UV) radiation:
- There have also been changes in the distribution and stage of melanoma at diagnosis:
- With an overall trend toward thinner tumors:
- Particularly among any patients with T1 / T2 melanomas:
- While the opposite trend is seen among patients with thick, T4 lesions
- Particularly among any patients with T1 / T2 melanomas:
- With an overall trend toward thinner tumors:
- Etiology and Epidemiology of Cutaneous Melanoma:
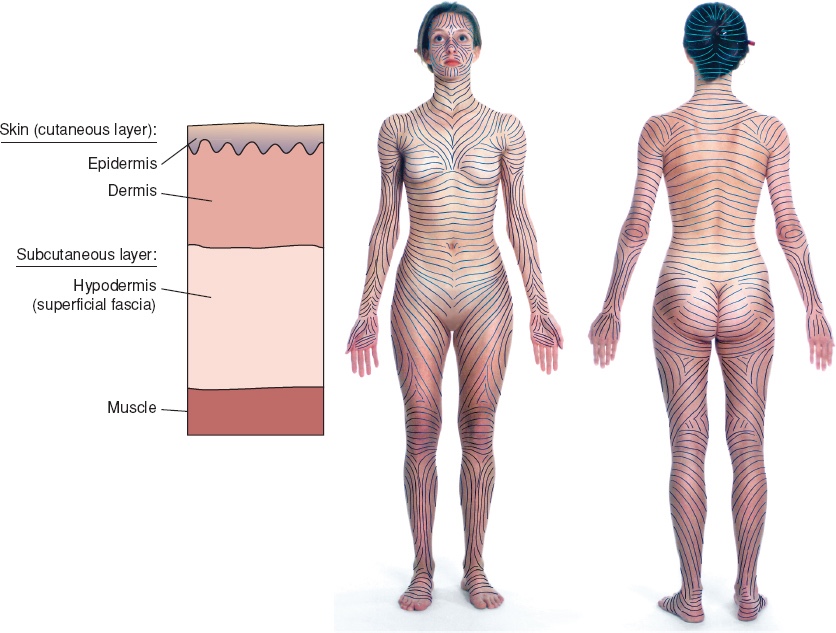
- Cutaneous melanoma originates from melanocytes within the epidermal layer of the skin
- Although these melanocytes represent a heterogeneous group of cells within the body:
- They all share a common place of origin:
- The neural crest, and the ability to produce melanin
- They all share a common place of origin:
- In humans:
- Melanin acts as the primary determinant of skin color and provides a layer of protection from ultraviolet (UV) radiation
- Risk factors for the development of cutaneous melanoma include:
- Sun exposure
- Blistering sunburns
- Fair complexion
- Family history
- Increasing age
- Previous melanoma
- Dysplastic nevi
- Although UV radiation is a critical factor in the development of most melanoma:
- It can occur in unexposed areas of the skin:
- Such as the perineum, palms of the hands, and soles of the feet
- It can occur in unexposed areas of the skin:
- However, most melanomas start on the:
- Trunk in men and on the legs in women
- Cutaneous melanoma is not the most common form of skin cancer:
- But presents a considerable health burden as the incidence of disease continues to increase rapidly for both sexes
- In the United States:
- There is a higher rate of melanoma in men than in women:
- But this tends to vary by age:
- With men more at risk after the age of 50 years
- But this tends to vary by age:
- There is a higher rate of melanoma in men than in women:
- Despite the rising rates of melanoma:
- The prognosis remains excellent for those diagnosed and treated early:
- With surgery providing the best form of cure for those with early-stage disease
- The prognosis remains excellent for those diagnosed and treated early:
- Cutaneous malignancies constitute the most commonly diagnosed cancers in the United States of America (USA):
- More than half of all cancers diagnosed each year
- In the USA, approximately 1.2 million to 1.4 million cases of skin cancer are diagnosed annually
- The most common skin cancer types are:
- Basal cell carcinoma (BCC)
- Squamous cell carcinoma (SCC)
- Melanoma:
- The incidence is increasing dramatically:
- At an overall rate of 33% for men and 23% for women from 2002 to 2006:
- About 2.6% per year
- At an overall rate of 33% for men and 23% for women from 2002 to 2006:
- These estimates for new cases may represent a substantial underestimation because many superficial and in-situ melanomas treated in the outpatient setting are not reported
- Approximately 8000 patients will be found to have metastatic melanoma at the time of diagnosis
- Cutaneous melanoma accounts for 4% of all skin cancer diagnosis:
- But accounts for 75% of skin cancer deaths
- The age-adjusted incidence of invasive melanoma in the USA:
- Increased from approximately 4 per 100,000 to 18 per 100,000 in white males between 1973 and 1998
- The age-adjusted incidence of invasive melanoma in the USA increased to 21.1 per 100,000 in white males between 2011 and 2015
- The incidence of melanoma continues to increase dramatically:
- Melanoma is increasing in men more rapidly than any other malignancy and, in women more rapidly than any other malignancy except lung cancer:
- This disturbing increase can be ascribed to prevailing social attitudes toward sun exposure
- Melanoma is increasing in men more rapidly than any other malignancy and, in women more rapidly than any other malignancy except lung cancer:
- The incidence is increasing dramatically:
- Recently, The Cancer Genome Atlas (TCGA) program performed DNA-, RNA-, and protein-based analysis of 333 primary and / or metastatic melanomas to catalog the most frequently encountered somatic alterations in cutaneous melanoma:
- Using these data, cutaneous melanoma was then divided into four genomic subtypes:
- BRAF
- RAS
- NF1
- Triple-WT
- The BRAF subtype is the largest genomic subtype:
- Whereas RAS and NF1 are described as the second and third major subtypes, respectively
- Although these first three subtypes are defined by their name-specific mutations:
- Triple-WT subtype is defined as a:
- Heterogeneous subgroup characterized by:
- A lack of BRAF, RAS, or NF1 mutations
- Heterogeneous subgroup characterized by:
- Triple-WT subtype is defined as a:
- Clinically, BRAF subtypes were:
- Younger than patients in the other subtypes:
- Whereas those in the NF1 subtype were older
- Younger than patients in the other subtypes:
- BRAF, RAS, and NF1 subtypes were noted to harbor a UV signature:
- Defined as a high fraction of cytosine to thymine transitions at dipyrimidine sites:
- In over 90% of the samples:
- Compared with only 30% of the Triple-WT samples
- In over 90% of the samples:
- Defined as a high fraction of cytosine to thymine transitions at dipyrimidine sites:
- These distinct genomic classifications provide a framework for identification of potential therapeutic targets and predictive biomarkers
- Using these data, cutaneous melanoma was then divided into four genomic subtypes:
- Risk Factors for developmenting melanoma:
- Pigment characteristics are important determinants of melanoma susceptibility:
- There is an inverse correlation between melanoma risk and skin color that goes from lightest skin to darkest skin:
- Melanoma occurs infrequently in skin of color:
- Suggesting that skin pigment plays a protective role
- Melanoma is 10 to 20 times more common in whites, and 6 to 7 times more common in Hispanics than in African Americans (AA)
- Melanoma occurs infrequently in skin of color:
- There is an inverse correlation between melanoma risk and skin color that goes from lightest skin to darkest skin:
- Fair complexion:
- Fitzpatrick skin photo-type I and II
- Blue or green eyes
- Blond or red hair
- Freckling
- Pigment characteristics are important determinants of melanoma susceptibility:
- A recent meta-analysis reported, that in contrast with people with Fitzpatrick skin photo-type IV:
- Those with Fitzpatrick skin photo-type I are at more than double (2.27 times) the risk, photo-type II at double (1.99 times) the risk, and photo-type IIIa 35% increased risk for developing malignant melanoma
- People with red / red – blonde hair:
- Have triple the malignant melanoma risk compared to dark-haired people
- People with blond hair:
- Are at double the risk
- People with light brown hair:
- Are at 46% increased risk
- Individuals with freckles:
- Have double (1.99 times) the risk of malignant melanoma, as opposed to people without freckles:
- These individuals with freckles have increased malignant melanoma risk:
- Irrespective of the number of moles they have
- These individuals with freckles have increased malignant melanoma risk:
- Have double (1.99 times) the risk of malignant melanoma, as opposed to people without freckles:
- Individuals with blue / green-blue / green-grey eyes:
- Are at increased risk of basal cell carcinoma (BCC):
- The risk for melanoma is less well known
- Are at increased risk of basal cell carcinoma (BCC):
#Arrangoiz #CancerSurgeon #SurgicalOncologist #HeadandNeckSurgeon #Melanoma #SkinCancer #CASO #CenterforAdvancedSurgicalOncology