- The treatment of NMSC requires careful evaluation of:
- Tumor size
- Pathologic characteristics
- Anatomical location
- Age
- Overall health of the patient
- Cost to the patient
- Cosmesis
- Treatment modalities can be divided into:
- Surgical and nonsurgical therapies:
- Although surgical intervention is often the mainstay of treatment
- Surgical and nonsurgical therapies:
- Surgical Techniques:
- Primary surgical excision with a margin of clinically normal tissue:
- Allows subsequent evaluation of the entire specimen for clear margins
- Complete excision with a margin of clinically normal tissue:
- Is associated with 5-year disease-free rates of:
- Over 98% for BCC
- Over 92% for SCC
- Is associated with 5-year disease-free rates of:
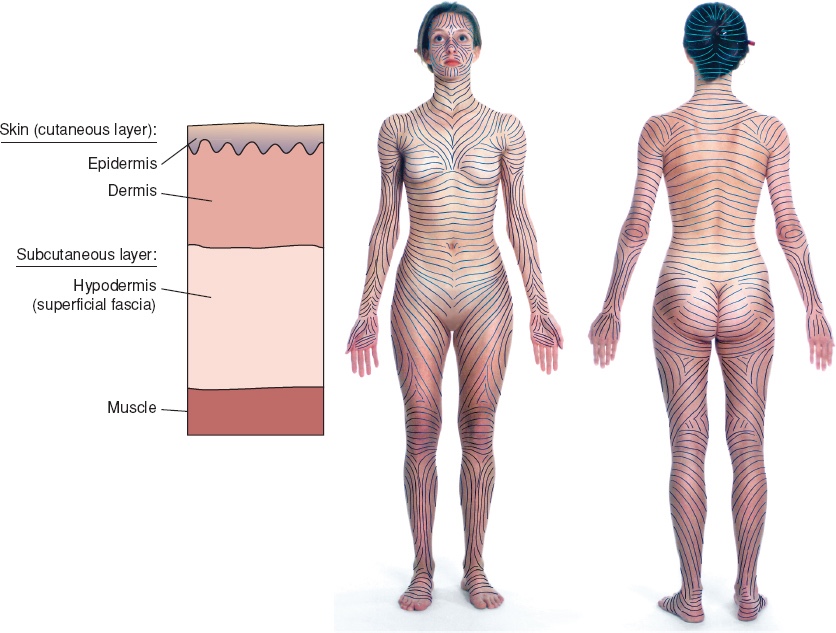
- Predetermined margins of 4 to 10 mm should be performed along Langer lines to achieve the best cosmetic result
- Primary surgical excision with a margin of clinically normal tissue:
- For well-defined, low-risk lesions less than 2 cm:
- Excision with a 4-mm margin around the tumor border:
- Is expected to definitively treat the tumor in 95% of cases
- Excision with a 4-mm margin around the tumor border:
- For high-risk tumors:
- A larger margin of at least 6 mm is indicated,
- European guidelines suggest at least 10-mm margin should be used
- Recurrent BCC:
- Is associated with a poor cure rate
- A 10-mm excision margin is recommended
- For incompletely excised lesions:
- Re excision is recommended if possible
- Mohs micrographic surgery:
- Involves removal of the clinical margins of the tumor under local anesthesia with immediate evaluation of the margins with frozen sections
- Small incremental sections are removed until the margins are clear
- This technique allows for the best cosmetic results by preserving normal tissue, while ensuring that larger lesions with subclinical extension are entirely removed
- Mohs micrographic surgery of primary and recurrent NMSC of the head and neck:
- Has a cure rate (negative histologic margin):
- Of 97%
- Has a cure rate (negative histologic margin):
- The reconstructive choices after Mohs surgery:
- Are similar to those available after traditional excision
- Although Mohs micrographic surgery is time consuming and requires skilled practitioners, the benefits of superior cosmesis and excellent cure rates make it the treatment of choice for many patients
- Indications for Mohs procedure are:
- Centrofacially located tumors
- Large tumors
- Poorly defined tumor margins
- Recurrent lesions
- Lesions with perineural or perivascular involvement
- Tumors at a site of prior radiation therapy
- Tumors in the setting of immunosuppression
- Patients with high-risk histologic subtypes of BCC
- There has been considerable interest in performing sentinel lymph node (SLN) biopsy:
- In selected patients with high-risk SCC:
- In hopes that detection and treatment of subclinical nodal metastases:
- Will lead to improved outcomes for these patients
- In hopes that detection and treatment of subclinical nodal metastases:
- In a pooled evaluation of 83 high-risk SCC patients:
- All patients with a positive SLN had lesions > 2 cm in diameter
- Among patients with tumors < 2 cm, 2.1 to 3 cm, and > 3 cm in diameter:
- The proportions of patients with a positive SLN were:
- 0%, 15.8%, and 30.4%, respectively
- The proportions of patients with a positive SLN were:
- While the available data suggest SLN biopsy can accurately identify micrometastatic nodal disease in patients with SCC:
- Studies to date are limited by small sample size, limited follow-up, and lack of uniform criteria
- Additional studies will be needed before definitive guidelines can be established with respect to SLN biopsy
- In selected patients with high-risk SCC:
- Destructive Techniques:
- Destructive techniques for superficial BCC and SCC include:
- Curettage
- Cryotherapy
- Laser ablation
- Curettage involves debulking the tumor under local anesthesia with a sharp curette until firm underlying dermis is reached
- The base is hyfrecated, and the process is repeated two or three times
- This technique is reserved for:
- Small (less than 1 cm), primary, low risk, or superficial tumors in non–hair-bearing areas:
- As such is not suitable for recurrent or ill-defined tumors
- Small (less than 1 cm), primary, low risk, or superficial tumors in non–hair-bearing areas:
- The technique is based on the ability of the sharp curette to differentiate friable tumor tissue from normal dermis
- If subcutaneous fat is reached during this technique:
- It is necessary to convert to surgical excision:
- As the curette will no longer be able to distinguish soft fat tissue from tumor
- It is necessary to convert to surgical excision:
- Destructive techniques for superficial BCC and SCC include:
- Cryotherapy:
- Is a destructive method primarily reserved for the treatment of precancerous lesions such as:
- Actinic keratosis (AKs)
- Occasionally for small, superficial, low-risk, primary BCCs or SCCs
- Liquid nitrogen:
- Is either sprayed with a cryogen or is directly applied to the lesion with cotton-tipped applicators for a period of time such that the visible thawing of the lesions takes at least 15 seconds (30 seconds for superficial SCC or BCC)
- Is a destructive method primarily reserved for the treatment of precancerous lesions such as:
- Ablation with a carbon dioxide laser:
- May be considered for precancerous lesions or low-risk BCC:
- However, follicular involvement may be difficult to treat and lead to recurrence
- May be considered for precancerous lesions or low-risk BCC:
#Arrangoiz #CancerSurgeon #Miami #SurgicalOncology #HeadandNeckSurgeon #CASO #CenterforAdvancedSurgicalOncology #BCC #SCC #NonMelonomaSkinCancer
