#Arrangoiz #ThyroidSurgeon #CancerSurgeon #ThryoidExpert #ThyroidNodules #ThyroidCancer #Miami
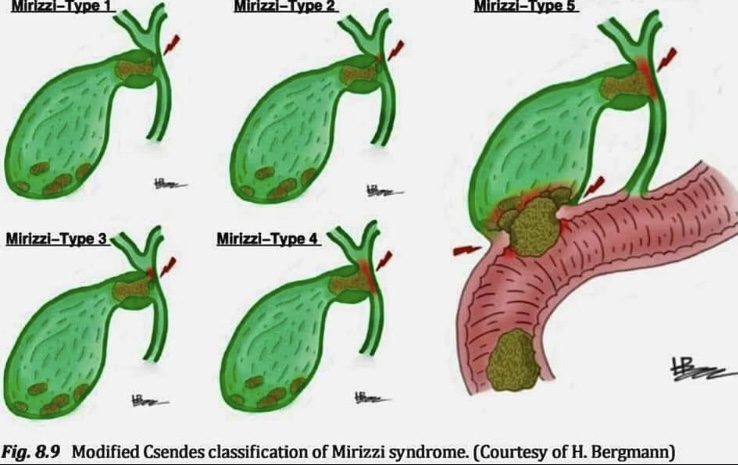
-Mirizzi syndrome is subclassified in to 5 types :
🔴𝗜: Is obstruction of the extrahepatic bile duct stone/s in the Hartmann’s pouch or cystic duct.
🔴𝗜𝗜: Is with a cholecystocholedochal fistula (diameter < 1/3 or the common hepatic duct wall).
🔴𝗜𝗜𝗜: Is with a cholecystocholedochal fistula (diameter < 2/3 of the common hepatic duct wall).
🔴𝗜𝗩: Is with a cholecystocholedochal fistula (involving the whole common hepatic duct wall).
🔴𝗩: Any type associated with a cholecystoenteral fistula (i.e,fistula to stomach, duodenum or hepatic flexure or transverse colon). This is sometimes sub-classiied depending on whether gallstone ileus is present or not.
𝙍𝙚𝙛:Difficult Acute Cholecystitis Treatment and Technical Issues,1st ed. 2021© Springer.
#Arrangoiz #Surgeon #CASO #Miami #CenterforAdvancedSurgicalOncology
#Arrangoiz #HeadandNeckSurgeon #CancerSurgeon #ThyroidSurgeon #ThyroidExpert #CASO #Miami #CenterforAdvancedSurgicalOncology
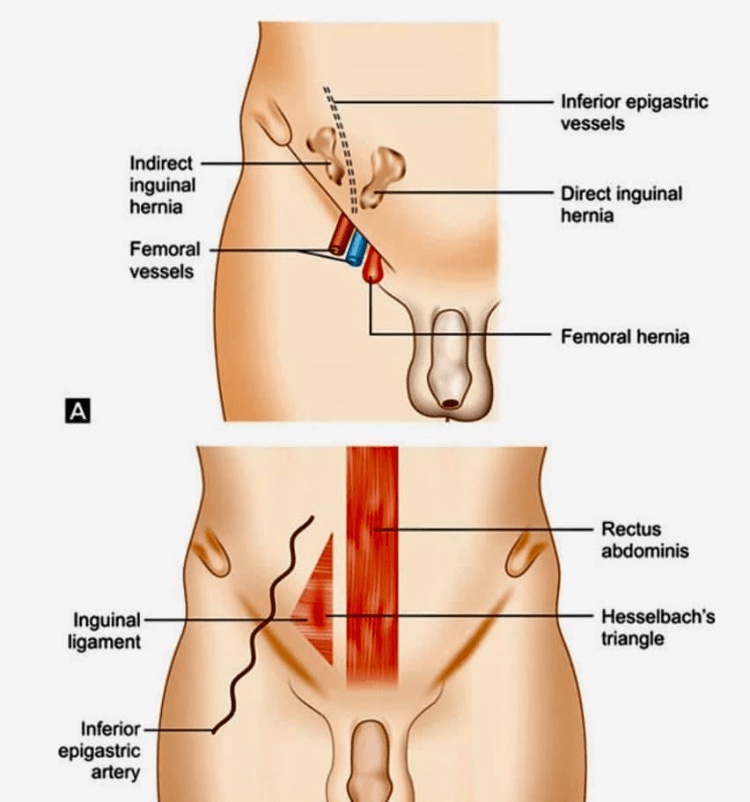
Busoga hernias, also known as Gill-Ogilvie hernias
🔴They are a variant of the direct inguinal hernia involving the conjoint tendon.
🔴Busoga herniae have been noted to occur most commonly in young, athletic men with a well-developed abdominal musculature. There is an increased incidence of Busoga hernia in Uganda.
🔴The conjoint tendon medially reinforces the posterior wall of the inguinal canal. It is protrusion here, at the medial aspect of the posterior aspect of the inguinal canal were weakening can result in herniation. Weakening in the conjoint tendon is thought to be secondary to rigorous training, with kicking, running, and sharp turns
#Arrangoiz #Miami #Surgeon #CASO #CenterforAdvancedSurgicalOncology
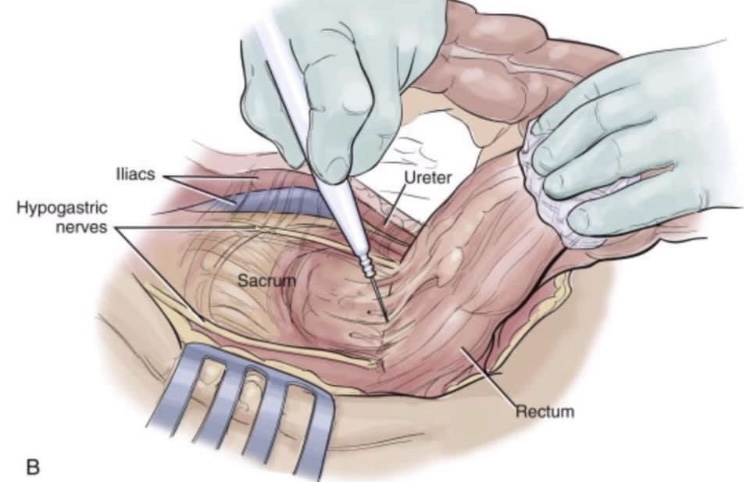
📙📜Holy plane of Heald📜📙
🔴Dissection is along the avascular alveolar plane between the presacral and mesorectal fascia, described as holy plane (Heald’s “holy plane”).
🔴The mesorectum refers to a fatty connective tissue layer, measuring 2–3 cm in thickness, with associated vessels, lymphatics and lymph nodes, which surrounds the rectum and is enveloped by fascia.
🔴mesorectal dissection occurs in a total avascular plane that, once identified, can be easily dissected, exposing ‘the white side of the yellow’ as Heald first described in 1979. As the posterior dissection continues downward, the mesorectum looks more and more bilobate (indicating a good quality of the dissection) until it thins out and disappears.
Once again traction and counter traction are essential in lateral and anterior resection to identify the dissection plane.
🔴The relationship of the rectum and pelvic autonomic nerves during open surgery when standing on the patient’s left. The ligation of the inferior mesenteric artery should be performed 1.5–2 cm from its origin from the aorta to avoid damaging the superior hypogastric plexus. At the pelvis, for posterior and lateral tumours, dissection should be directed below the Denonvillliers fascia to avoid damaging the neurovascular bundles that run along the tip of the seminal vesicle (2 and 10 o’clock directions).
#Arrangoiz #Surgeon #Teacher #CancerSurgeon #CASO #Miami #CenterforAdvancedSurgicalOncology