- Hereditary MTC:
- Is unique in many ways among inherited cancer syndromes:
- MTC is founded on the following findings:
- The hereditary variant:
- Affecting as many as 25% of MTC patients:
- Is more frequent than many other common hereditary tumors.
- Affecting as many as 25% of MTC patients:
- Unlike many other hereditary tumors:
- Hereditary MTC features a strong genotype-phenotype correlation:
- That is utilized worldwide for risk assessment
- This genotype-dependent, age-related tumor progression:
- Not only underlies the development of:
- Hereditary MTC
- But also the formation of:
- MEN 2–associated pheochromocytoma and hyperparathyroidism (HPT).
- Not only underlies the development of:
- Hereditary MTC features a strong genotype-phenotype correlation:
- The hereditary variant:
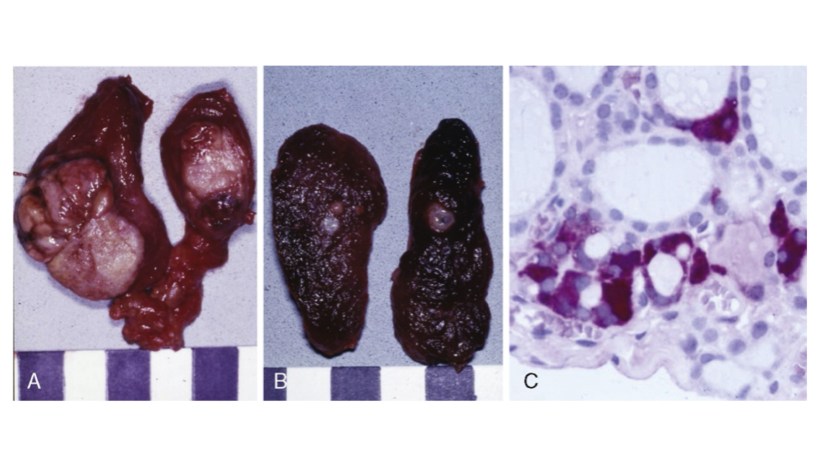
- Disease progression from C-cell hyperplasia to MTC:
- Requiring the acquisition of somatic mutations for malignant progression:
- Is a stochastic sequence of events not fully under the control of a gene carrier’s genetic makeup.
- Requiring the acquisition of somatic mutations for malignant progression:
- Serum calcitonin:
- A sensitive diagnostic marker of MTC, better reflects a gene carrier’s stage of C-cell disease than his or her underlying germline mutation in the RET (REarranged during Transfection) proto-oncogene:
- We may now tailor the timing and extent of surgical intervention in the neck to the gene carrier’s stage of disease through consideration of serum calcitonin levels.
- A sensitive diagnostic marker of MTC, better reflects a gene carrier’s stage of C-cell disease than his or her underlying germline mutation in the RET (REarranged during Transfection) proto-oncogene:
- Lymph node metastases are indicative of progressive disease:
- Portending a worse prognosis for sporadic and hereditary MTC alike.
- Although multifocal tumor growth:
- More common in hereditary than sporadic MTC:
- 65% versus 8%:
- No difference in biochemical cure and survival between hereditary and sporadic disease has been found after adjusting for extent of disease.
- 65% versus 8%:
- More common in hereditary than sporadic MTC:
- MEN 2B is a special and virulent variant of MEN type 2:
- Characterized by the presence of MTC in early infancy.
- More than 90% of MEN 2B RET gene carriers:
- Harbor de novo germline mutations.
- Such de novo germline mutations are rare in other MTC syndromic settings such as familial MTC (FMTC) and MEN 2A.
- DNA-based screening of families for the MEN 2B trait for early detection of hereditary MTC hence is rarely an option.
- Intriguingly, there are some early clues in MEN 2B infants:
- Notably tearless crying and pseudo-Hirschsprung’s disease:
- These clinical signs may help identify gene carriers before they develop the more characteristic MEN 2B stigmata:
- Prompting rapid DNA-based screening and immediate surgical intervention.
- These clinical signs may help identify gene carriers before they develop the more characteristic MEN 2B stigmata:
- Notably tearless crying and pseudo-Hirschsprung’s disease:
- MTC is founded on the following findings:
- Is unique in many ways among inherited cancer syndromes:

- What is Head and Neck Surgery?:
- It is a surgical sub-specialty that deals mainly with benign and malignant tumors of the head and neck region, including:
- The scalp, facial region, eyes, ears, nose, nasal fossae, paranasal sinuses, oral cavity, pharynx (nasopharynx, oropharynx, hypopharynx), larynx (supraglotic larynx, glottis larynx, subglotic larynx), thyroid gland, parathyroid gland, salivary glands (parotid glands, submandibular glands, sublingual glands, minor salivary glands), soft tissues of the neck, skin of the head and neck region.
- The head and neck surgeon’s work area:
- Does not cover tumors or diseases of the brain and other areas of the central nervous system or those of the cervical spine:
- This is the neurosurgeon field.
- Does not cover tumors or diseases of the brain and other areas of the central nervous system or those of the cervical spine:
- The head and neck surgeon’s work area:
- The scalp, facial region, eyes, ears, nose, nasal fossae, paranasal sinuses, oral cavity, pharynx (nasopharynx, oropharynx, hypopharynx), larynx (supraglotic larynx, glottis larynx, subglotic larynx), thyroid gland, parathyroid gland, salivary glands (parotid glands, submandibular glands, sublingual glands, minor salivary glands), soft tissues of the neck, skin of the head and neck region.
- Among the diagnostic procedures performed by the head and neck surgeon, are the following:
- Nasopharyngolaryngoscopy:
- Performed to examine, evaluate and, possibly perform a biopsy, of oral cavity, pharyngeal and laryngeal lesions.
- Nasopharyngolaryngoscopy:
- The surgeries most commonly performed by the head and neck surgeon are:
- Total or near total thyroidectomies
- Hemithryoidectomies (lobectomies)
- Comprehensive neck dissections
- Selective neck dissections
- Maxillectomies:
- Total maxillectomy
- Subtotal maxillectomy
- Infrastructure maxillectomy
- Suprastructure maxillectomy
- Medial maxillectomy
- Mandibulectomy:
- Segmental
- Marginal
- Tracheostomy
- Salivary gland surgeries:
- Parotid gland operations:
- Limited superficial parotidectomy with identification and preservation of the facial nerve
- Superficial parotidectomy with identification and preservation of the facial nerve
- Near total parotidectomy with identification and preservation of the facial nerve
- Total parotidectomy
- Submandibular gland resection
- Sublingual gland resection
- Parotid gland operations:
- Resection of tumors of the oral cavity:
- Glossectomy
- Resection of the floor of the mouth tumors
- Resection of tumors of the pharynx
- Resection of tumors of the larynx
- Split-thickness skin grafts
- Full-thickness skin grafts
- Sentinel lymph node mapping and sentinel lymph node biopsy
- Resection of malignant skin tumors (BCC, SCC, melanoma) of the head and neck region
- It is a surgical sub-specialty that deals mainly with benign and malignant tumors of the head and neck region, including:
- The formation of the head and neck surgeon includes mastering the following subjects:
- Surgical Anatomy
- History and Basic Principles of Head and Neck Surgery
- Epidemiology, Etiology, and Pathology of Head and Neck Diseases
- Diagnostic Radiology of the Head and Neck Region
- Tumors of the Scalp, Skin and Melanoma
- Eyelids and Orbit
- Nasal Cavity and Paranasal Sinuses
- Skull Base and Temporal Bone
- Lips and Oral Cavity
- Pharynx and Esophagus
- Larynx and Trachea
- Cervical Lymph Nodes
- Thyroid and Parathyroid Glands
- Salivary Glands
- Neurogenic Tumors and Paragangliomas
- Soft Tissue Tumors
- Bone Tumors and Odontogenic Lesions
- Reconstructive Surgery
- Oncologic Dentistry and Maxillofacial Prosthetics
- Principles of Radiation Oncology
- Principles of Chemotherapy
- Molecular Oncology, Genomics and Immunology
- Nutrition
- Biostatistic
-
Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon / endocrine surgeon / surgical oncologist and is a member of Sociedad Quirúrgica S.C at the America British Cowdray Medical Center in Mexico City:

- Rodrigo Arrangoiz MS, MD, FACS:
- Is a member of the American Head and Neck Society

-
- He is a member of the American Thyroid Association:





