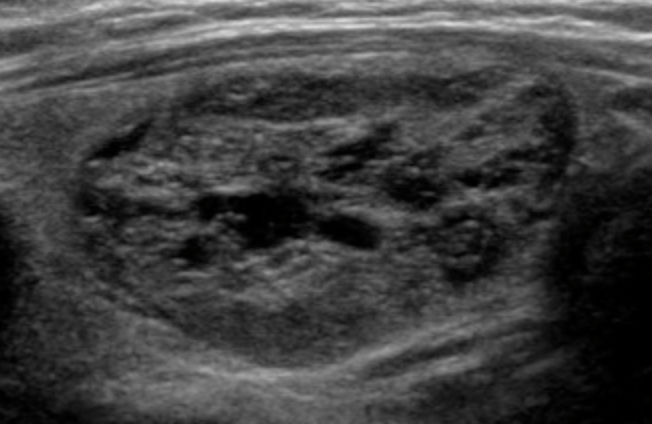
- Asymptomatic, small thyroid nodules (usually ≤ 1 cm maximal diameter, 1 cm3, or 1 mL volume) confined to the thyroid and surrounded by normal thyroid parenchyma:
- Can be followed with active surveillance:
- With or without cytologic confirmation:
- In patients who value their normal thyroid function and who desire avoidance of thyroid surgery
- Can be followed with active surveillance:
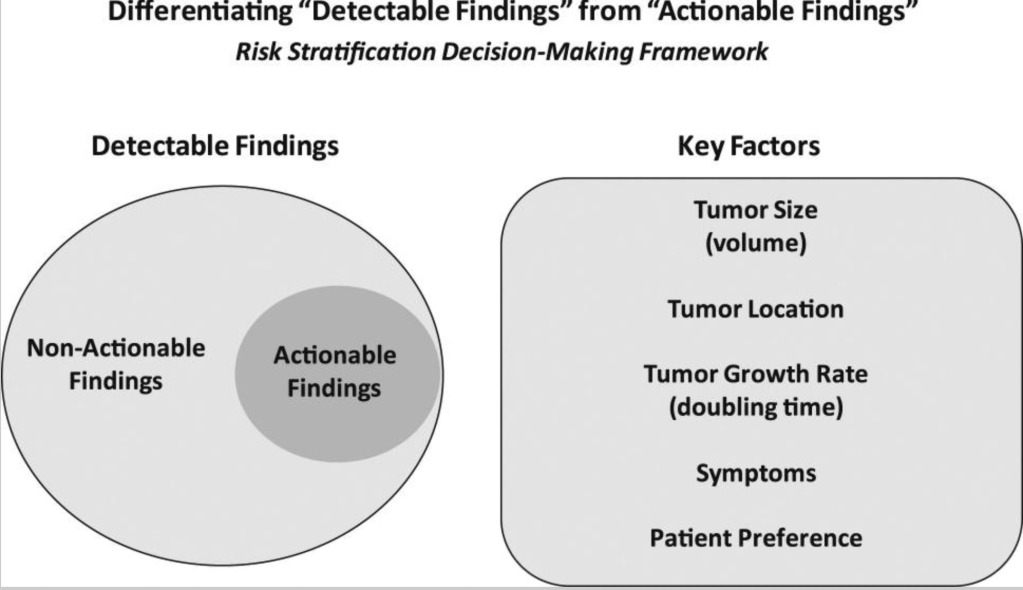
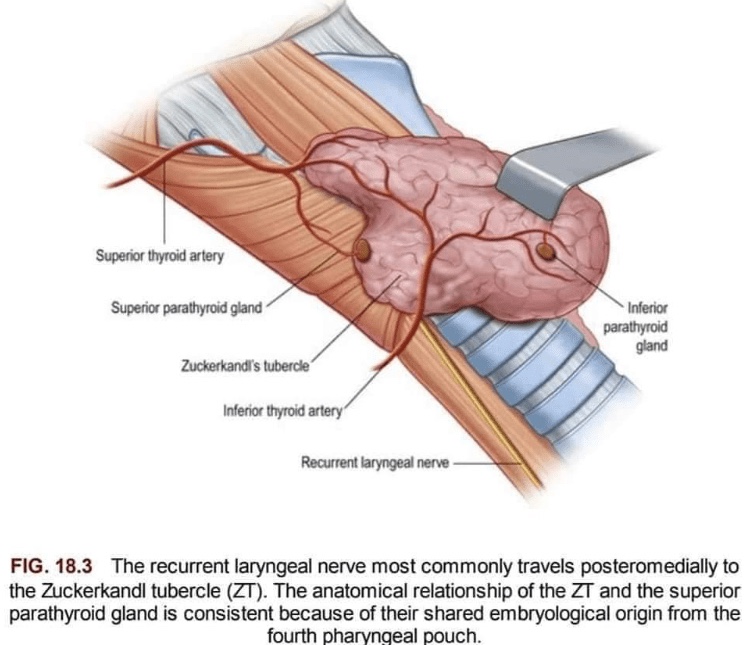
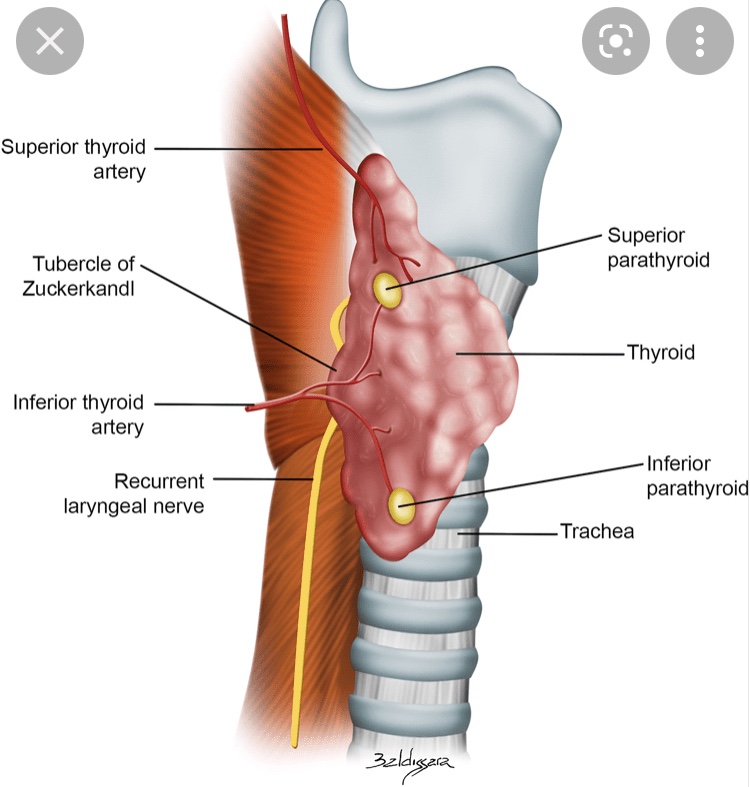
- Patients who demonstrate tumors larger than 1.5 to 2.0 cm; tumors in subcapsular locations adjacent to important structures, such as the trachea and recurrent laryngeal nerve; or tumors with documented growth rate doubling times of less than 2 years:
- Are generally considered inappropriate for observation and would be considered to have actionable disease
- If the tumor growth rate is unknown at the time of nodule detection:
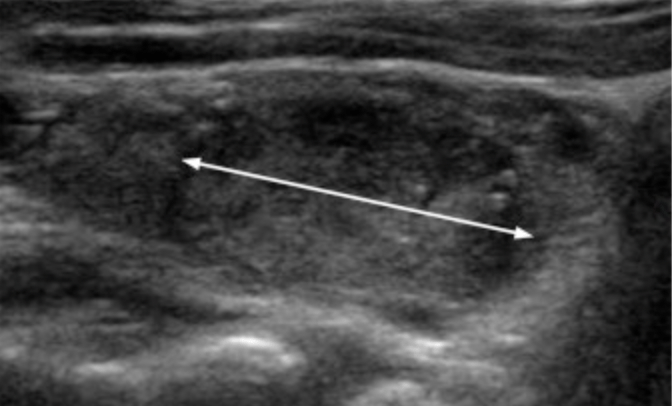
- Then this can be established with serial ultrasound evaluations:
- Done approximately every 6 months for 1 to 2 years
- Then this can be established with serial ultrasound evaluations:
- The frequency of ultrasound evaluations and long-term follow-up depends on the tumor size, location, and established growth rate
- With the use of this paradigm, active surveillance continues until there is a:
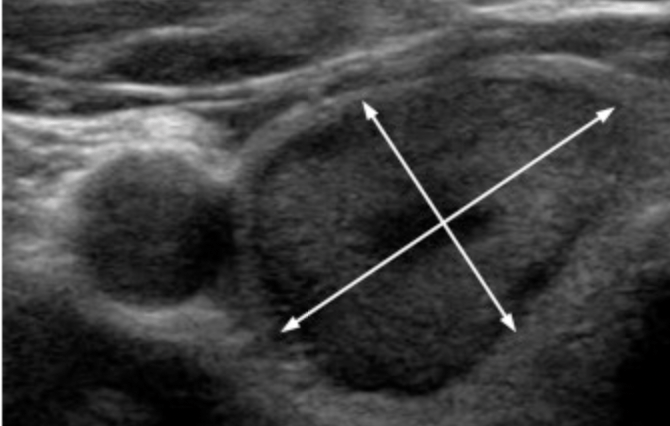
- 3-mm increase in tumor diameter:
- Which corresponds to a 100% increase in tumor volume
- Identification of metastatic disease
- Direct invasion into surrounding structures of the thyroid
- A decision to discontinue active surveillance based on patient preference
- 3-mm increase in tumor diameter:
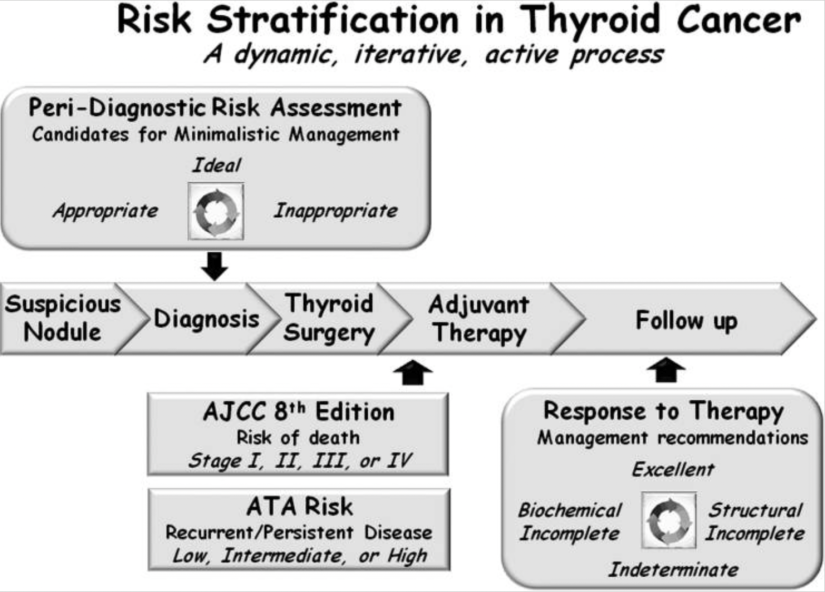
- This risk-stratified, minimalistic management approach to very low-risk thyroid cancers:
- Has been shown to be safe and effective over 5 to 10 years of follow-up in studies from Japan, Korea, and the United States
- In the first 10 years of active surveillance follow-up:
- Only 2% to 8% of papillary micro-carcinomas increase ≥ 3 mm in maximum diameter
- 12% to 14% demonstrate an increase in tumor volume of > 50% (the smallest change in nodule volume that can be reproducibly measured)
- Novel lymph node metastases are detected in 2% to 4%
- The likelihood of disease progression is higher in younger patients than in older patients
- Importantly, at the time of disease progression:
- Deferred surgical intervention is quite effective with excellent outcomes and no disease-specific mortality
#Arrangoiz #ThyroidSurgeon #ThyroidExpert #CancerSurgeon #SurgicalOncologist #HeadandNeckSurgeon #ThyroidCancer
 • Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina:
• Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina: • Maestria en ciencias (Clinical research for healthprofessionals):
• Maestria en ciencias (Clinical research for healthprofessionals): • Cirugia de tumores de cabeza y cuello / cirugiaendocrina
• Cirugia de tumores de cabeza y cuello / cirugiaendocrina
