- Thyroid nodules are exceedingly common:
- With a reported prevalence between 19%to 68% in adults:
- On high-resolution ultrasound
- With a reported prevalence between 19%to 68% in adults:
- Currently, fine-needle aspiration (FNA):
- Is the most effective, practical test to determine whether a nodule is malignant or may require surgery to reach a definitive diagnosis
- Most thyroid nodules are benign, and even malignant nodules, particularly ones smaller than 1 cm, frequently exhibit indolent or nonaggressive behavior:
- Therefore, not all detected nodules require FNA and / or surgery
- Despite a rapid increase in the reported incidence of papillary thyroid cancer (PTC) that resulted from screening thyroid sonography in asymptomatic patients in South Korea:
- Mortality has remained extremely low
- In the United States, over-diagnosis of thyroid cancer:
- Defined as “diagnosis of thyroid tumors that would not, if left alone, result in symptoms or death”:
- Accounted for 70% to 80% of thyroid cancer cases in women and 45% of cases in men between 2003 and 2007:
- Therefore, a reliable, noninvasive method to identify which nodules warrant FNA on the basis of a reasonable likelihood of biologically significant malignancy would be highly desirable
- Accounted for 70% to 80% of thyroid cancer cases in women and 45% of cases in men between 2003 and 2007:
- Defined as “diagnosis of thyroid tumors that would not, if left alone, result in symptoms or death”:
- In 2015, committees convened by the ACR published white papers:
- That presented an approach to incidental thyroid nodules and proposed standard terminology (lexicon) for ultrasound reporting
- Project Rationale and Consensus Process:
- Several professional societies and groups of investigators have proposed methods to guide ultrasound practitioners in recommending FNA on the basis of ultrasound features
- Some of these systems were termed TI-RADS (Thyroid Imaging, Reporting and Data System):
- Because they were modeled on the ACR’s BI-RADS®, which has been widely accepted in breast imaging
- Other societies, such as the American Thyroid Association (ATA):
- Have taken a slightly different, pattern-oriented approach, but with the same intent
- The plethora, complexity, and lack of congruence of these systems has limited their adoption by the ultrasound community and inspired our effort to publish a classification system under the auspices of the ACR
- The ACR TI-RADS Committee agreed on the following attributes for our risk classification algorithm. It would be:
- Founded on the ultrasound features defined in there previously published lexico
- Easy to apply across a wide gamut of ultrasound practices
- Able to classify all thyroid nodules
- Evidence based to the greatest extent possible
- The proposals presented in this white paper, which were developed via conference calls, e-mail, and online surveys, represent the consensus opinion of the ACR TI-RADS Committee:
- They are based on the literature; analysis of data from the Surveillance, Epidemiology, and End Results (SEER) Program of the National Cancer Institute
- Evaluation of existing risk classification systems; and expert opinion
- Our recommendations are intended to serve as guidance for practitioners who incorporate ultrasound in the management of adult patients with thyroid nodules
- They should not be construed as standards
- Interpreting and referring physicians are legally and professionally responsible for applying their professional judgment to every case, regardless of the ACR TI-RADS recommendations
- The decision to perform FNA should also account for:
- The referring physician’s preference and the patient’s risk factors for thyroid cancer, anxiety, comorbidities, life expectancy, and other relevant considerations
- Overview of ACR TI-RADS:
- The ultrasound features in the ACR TI-RADS are categorized as:
- Benign
- Minimally suspicious for malignancy
- Moderately suspicious for malignancy
- Highly suspicious for malignancy
- Points are given for all the ultrasound features in a nodule:
- With more suspicious features being awarded additional points
- Figure 1 presents these features arranged per the five lexicon categories
- When assessing a nodule:
- The reader selects one feature from each of the first four categories and all the features that apply from the final category and sums the points
- The point total determines the nodule’s ACR TI-RADS level:
- Which ranges from TR1 (benign) to TR5 (high suspicion of malignancy)
- Note that although it is possible for a nodule to be awarded zero points and hence be characterized as TR1:
- All other nodules merit at least two points because a nodule that has a mixed cystic and solid composition (one point) will also gain at least one more point for the echogenicity of its solid component
- Note that although it is possible for a nodule to be awarded zero points and hence be characterized as TR1:
- Which ranges from TR1 (benign) to TR5 (high suspicion of malignancy)
- Finally, although sonoelastography is a promising technique, it is probably not available in many ultrasound laboratories and is not incorporated into the ACR TI-RADS
- In the ACR TI-RADS, recommendations for FNA or ultrasound follow-up:
- Are based on a nodule’s ACR TI-RADS level and its maximum diameter
- For risk levels TR3 through TR5:
- The chart presents a size threshold at or above which FNA should be recommended
- They also defined lower size limits for recommending follow-up ultrasound for TR3, TR4, and TR5 nodules to limit the number of repeat sonograms for those that are likely to be benign or not clinically significant
- In developing the ACR TI-RADS, the committee strived to account for the discrepancy between the sharp rise in the diagnosis and treatment of thyroid cancer resulting from increased detection and biopsy and the lack of commensurate improvement in long-term outcomes
- This suggested that diagnosing every thyroid malignancy should not be our goal
- Like other professional societies:
- The ACR TIRADS recommend biopsy of high-suspicion nodules only if they are 1 cm or larger
- As well, they advocate biopsy of nodules that have a low risk for malignancy only when they measure 2.5 cm or more
- The ACR TI-RADS is designed to balance the benefit of identifying clinically important cancers against the risk and cost of subjecting patients with benign nodules or indolent cancers to biopsy and treatment
- There recommendations for follow-up ultrasound substantially mitigate the possibility that significant malignancies will remain undetected over time and are concordant with the increasing trend toward active surveillance (“watchful waiting”) for low-risk thyroid cancer
- The ultrasound features in the ACR TI-RADS are categorized as:
- Differences Between ACR TI-RADS and Other Systems:
- Structure:
- To make the system easy to understand and apply, the ACR TI-RADS does not include:
- Subcategories, nor does it include a TR0 category to indicate a normal thyroid gland
- The ACR TI-RADS also lends itself to implementation as templates in voice recognition reporting or computerized decision support systems
- The committee decided against the pattern-based approach used by the ATA on the basis of the results of a study by Yoon et al:
- Which showed that the ATA guidelines:
- Were unable to classify 3.4% of 1,293 nodules:
- Of which 18.2% were malignant
- Notably, that study included only nodules that were subjected to FNA or surgery
- It is likely that an even greater percentage of nodules would not have been categorized had other nodules been included, as it is not practical to provide patterns that account for every potential constellation of features
- Were unable to classify 3.4% of 1,293 nodules:
- Which showed that the ATA guidelines:
- To make the system easy to understand and apply, the ACR TI-RADS does not include:
- Structure:
- Size Thresholds for FNA:
- The ACR TI-RADS is consistent with most other guidelines:
- In recommending FNA for highly suspicious nodules 1 cm or larger:
- However, thresholds for mildly suspicious and moderately suspicious nodules (2.5 and 1.5 cm, respectively):
- Are higher than the cutoffs advocated by the ATA and the Korean Society of Thyroid Radiology
- In a 2005 publication cited by both organizations, Machens et al:
- Contended that the cumulative risk for distant metastases from papillary and follicular thyroid cancer:
- Rose at a threshold of 2 cm
- They therefore advocated biopsy of nodules larger than 2 cm
- However, reviewing their graphs suggested a gradual, slight increase that began at a larger size
- More important, Machens et al based their analysis on tumor size in resected specimens, not on ultrasound dimensions
- Contended that the cumulative risk for distant metastases from papillary and follicular thyroid cancer:
- Subsequent research has demonstrated a significant lack of concordance between sonographic and pathologic sizing:
- With a tendency for ultrasound to result in larger measurements
- Of 205 papillary carcinomas ≥ 1.5 cm studied by Bachar et al:
- The mean diameter on ultrasound was 2.65 ± 1.07 cm, compared with 1.97 ± 1.17 cm on pathology
- The committee’s higher size cutoffs reflect this discrepancy:
- ACR further guided by evaluation of a database of more than 3,000 proven thyroid nodules that was created for a study sponsored by the Society of Radiologists in Ultrasound:
- Partial analysis showed cancer risk levels of:
- No more than 2% for TR1 and TR2 nodules
- 5% for TR3 nodules
- 5% to 20% for TR4 nodules
- At least 20% for TR5 nodules
- Partial analysis showed cancer risk levels of:
- They also considered published and SEER data analyses:
- That showed a slight increase in distant metastases:
- At 2.5 cm
- As well as slight increments in 10-year relative and thyroid cancer-specific mortality:
- At 3 cm
- That showed a slight increase in distant metastases:
- ACR further guided by evaluation of a database of more than 3,000 proven thyroid nodules that was created for a study sponsored by the Society of Radiologists in Ultrasound:
- The ACR TI-RADS is consistent with most other guidelines:
- ACR TI-RADS Feature Categories:
- Composition:
- Nodules that are cystic or almost completely cystic merit no points because they are almost universally benign
- A spongiform architecture is highly correlated with benign cytology:
- Regardless of its relative echogenicity or other features
- However, a spongiform nodule must be composed predominantly (greater than 50%) of small cystic spaces
- Nodules should not be characterized as spongiform solely on the basis of the presence of a few, scattered cystic components in an otherwise solid nodule
- “Mixed cystic and solid” combines two features from the lexicon, predominately solid and predominately cystic
- The appearance of the solid component is more important than the overall size of the nodule or the proportion of solid versus cystic components:
- In determining whether biopsy is warranted
- Solid material that is eccentric and has an acute angle with the nodule’s wall is suspicious, as is:
- Solid material with moderately or highly suspicious characteristics, such as:
- Decreased echogenicity
- Lobulation
- Punctate echogenic foci
- Solid material with moderately or highly suspicious characteristics, such as:
- As well, although color Doppler ultrasound has not been shown to reliably discriminate between benign and malignant nodules:
- The presence of flow in solid components:
- Distinguishes tissue from echogenic debris or hemorrhage:
- Inconsequential debris may be identified by:
- Layering or motion elicited by changes in patient position
- Inconsequential debris may be identified by:
- Distinguishes tissue from echogenic debris or hemorrhage:
- The presence of flow in solid components:
- Composition:
- Echogenicity:
- This feature refers to a nodule’s reflectivity relative to adjacent thyroid tissue:
- Except for very hypoechoic nodules:
- In which the strap muscles are used as the basis for comparison
- Except for very hypoechoic nodules:
- This category also includes “anechoic,” a zero-point feature that was absent from the lexicon:
- It applies to cystic or almost completely cystic nodules that would otherwise be given three points because of their very hypoechoic appearance
- This feature refers to a nodule’s reflectivity relative to adjacent thyroid tissue:
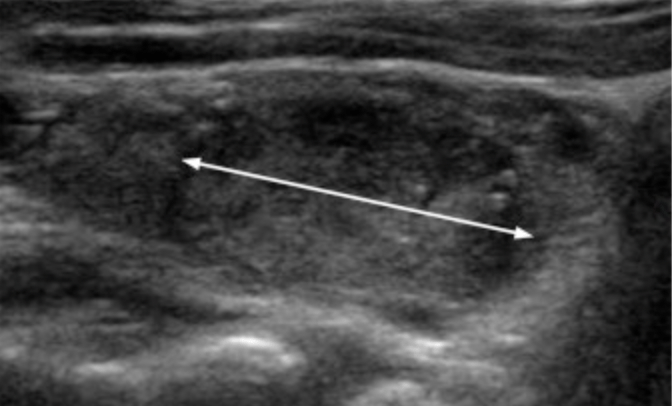
- Shape:
- A taller-than-wide shape:
- Is an insensitive but highly specific indicator of malignancy:
- This feature is evaluated in the axial plane:
- By comparing the height (“tallness”) and width of a nodule measured parallel and perpendicular to the ultrasound beam, respectively
- A taller-than-wide configuration is usually evident on visual inspection and rarely requires formal measurements
- This feature is evaluated in the axial plane:
- Is an insensitive but highly specific indicator of malignancy:
- A taller-than-wide shape:
- Margin:
- The presence of a halo is neither discriminatory nor mutually exclusive with other margin types; therefore, they elected to omit it
- They included “ill defined” in this group so that any reporting template that incorporates a field for margin will not be left empty if a nodule is not well defined.
- “Lobulated or irregular margin”:
- Refers to a spiculated or jagged edge, with or without protrusions into the surrounding parenchyma
- It may be difficult to recognize this finding if the nodule is:
- Ill defined, is embedded in a heterogeneous gland, or abuts multiple other nodules
- If the margin cannot be determined for any reason, zero points should be assigned
- Extension beyond the thyroid border is classified as:
- Extensive or minimal:
- We use the term border because the thyroid gland lacks a true fibrous capsule
- Extensive extra-thyroidal extension (ETE):
- That is characterized by frank invasion of adjacent soft tissue and / or vascular structures:
- Is a highly reliable sign of malignancy and is an unfavorable prognostic sign
- That is characterized by frank invasion of adjacent soft tissue and / or vascular structures:
- Minimal ETE may be suspected sonographically in the presence of:
- Border abutment
- Contour bulging
- Loss of the echogenic thyroid border
- However, agreement among pathologists for identification of minimal ETE is poor, and its clinical significance is controversial:
- Therefore, practitioners should exercise caution when reporting minimal ETE, particularly for otherwise benign-appearing nodules
- Extensive or minimal:
- Echogenic Foci:
- “Large comet-tail artifacts” are:
- Echogenic foci with V-shaped echoes greater than 1 mm deep to them
- They are associated with colloid and are strongly indicative of benignity when found within the cystic components of thyroid nodules
- “Macro-calcifications” are:
- Coarse echogenic foci accompanied by acoustic shadowing
- Evidence in the literature regarding their association with increased malignancy risk is mixed, especially in nodules lacking other malignant features
- Given published data that show a weakly positive relationship with malignancy:
- Macro-calcifications are assigned one point, recognizing that the risk is increased if the nodule also contains moderately or highly suspicious features that warrant additional points
- Peripheral calcifications:
- Lie along all or part of a nodule’s margin
- Their correlation with malignancy in the literature is variable
- However, because some publications suggest that they are more strongly associated with malignancy than macro-calcifications, they are awarded two points
- Some authors have called attention to interrupted peripheral calcifications with protruding soft tissue as suspicious for malignancy, but with low specificity
- In the ACR TI-RADS, this appearance qualifies as a lobulated margin:
- Which adds another two points to the nodule’s total assignment
- In nodules with calcifications that cause strong acoustic shadowing that precludes or limits assessment of internal characteristics, particularly echogenicity and composition:
- It is best to assume that the nodule is solid and assign two points for composition and one point for echogenicity
- Punctate echogenic foci are smaller than macro-calcifications and are non-shadowing:
- In the solid components of thyroid nodules, they may correspond to the psammomatous calcifications associated with papillary cancers and are therefore considered highly suspicious, particularly in combination with other suspicious features
- This category includes echogenic foci that are associated with small comet-tail artifacts in solid components:
- As distinguished from the large comet-tail artifacts described earlier
- Notably, small echogenic foci may be seen in spongiform nodules:
- Where they probably represent the back walls of minute cysts
- They are not suspicious in this circumstance and should not add to the point total of spongiform nodules
- “Large comet-tail artifacts” are:
- Additional Benign Appearances:
- Several ultrasound findings have been described as characteristic of benign nodules with a high degree of reliability
- These include:
- A uniformly hyperechoic (“white knight”) appearance
- A variegated pattern of hyperechoic areas separated by hypoechoic bands reminiscent of giraffe hide:
- Both in the setting of Hashimoto’s thyroiditis
- Because of their scarcity, the committee chose not to formally incorporate these patterns in the ACR TI-RADS chart
- Papillary Thyroid Micro-carcinomas:
- The ACR TI-RADS is concordant with other guidelines in recommending against routine biopsy of nodules smaller than 1 cm:
- Even if they are highly suspicious
- However, because some thyroid specialists advocate active surveillance, ablation, or lobectomy for papillary microcarcinomas:
- Biopsy of 5 mm to 9 mm TR5 nodules may be appropriate under certain circumstances
- The determination to perform FNA will involve shared decision making between the referring physician and the patient
- The report should indicate whether the nodule can be measured reproducibly on follow-up studies
- Additionally, nodules in critical submarginal locations may complicate surgery:
- Therefore, the report should also indicate whether the nodule abuts the trachea or whether it is adjacent to the tracheoesophageal groove (the location of the recurrent laryngeal nerve)
- The ACR TI-RADS is concordant with other guidelines in recommending against routine biopsy of nodules smaller than 1 cm:
- Reporting Considerations:
- Measurement and Documentation:
- Accurate sizing of thyroid nodules is critical, as the maximum dimension determines whether a given lesion should be biopsied or followed
- Although some interobserver discrepancy is inevitable because of variable conspicuity, consistent technique improves measurement accuracy and reproducibility
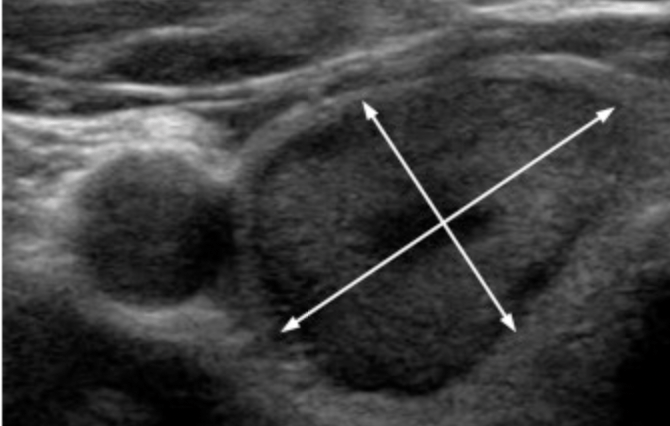
- Nodules should be measured in three axes:
- Maximum dimension on an axial image
- Maximum dimension perpendicular to the previous measurement on the same image
- Maximum longitudinal dimension on a sagittal image
- For obliquely oriented nodules, these measurements may be different than the ones used to determine a taller-than-wide shape, but this discrepancy should rarely present a problem in practice
- Measurements should also include:
- The nodule’s halo, if present
- Practitioners may use linear dimensions to determine volume, a calculation that is available on many ultrasound machines
- Regardless of the method used, each practice should measure and report nodules consistently to facilitate serial comparison
- Measurement and Documentation:
- Definition of Growth:
- Criteria for significant growth depend on:
- The size of the nodule and must take measurement variability into account
- In the ACR TI-RADS, significant enlargement is defined as:
- A 20% increase in at least two nodule dimensions and a minimal increase of 2 mm, or
- A 50% or greater increase in volume, as in the criteria adopted by other professional societies
- Because enlargement may not be apparent if the current sonogram is compared only with the immediately preceding one, it is important to also review measurements from earlier scans, if available
- Criteria for significant growth depend on:
- Timing of Follow-Up Sonograms:
- There is little consensus in the literature regarding optimal spacing of follow-up sonograms for nodules that do not meet size criteria for FNA, as growth rates do not reliably distinguish benign from malignant nodule
- The committee believes that scanning intervals of less than 1 year are not warranted:
- Except for proven cancers under active surveillance, which may require more frequent follow-up at the discretion of the referring physician
- We advocate timing on the basis of a nodule’s ACR TI-RADS level, with additional sonograms for lesions that are more suspicious:
- For a TR5 lesion, we recommend scans every year for up to 5 years
- For a TR4 lesion, scans should be done at 1, 2, 3, and 5 years
- For a TR3 lesion, follow-up imaging may be performed at 1, 3, and 5 years
- Imaging can stop at 5 years if there is no change in size, as stability over that time span reliably indicates that a nodule has a benign behavior
- There is no published evidence to guide management of nodules that enlarge significantly but remain below the FNA size threshold for their ACR TI-RADS level at 5 years, but continued follow-up is probably warranted
- If a nodule’s ACR TI-RADS level increases on follow-up, the next sonogram should be done in 1 year, regardless of its initial level
- Number of Nodules to Biopsy:
- Biopsy of three or more nodules is poorly tolerated by patients and increases cost with little or no benefit and some added risk
- Therefore, the committee recommends targeting no more than two nodules with the highest ACR TI-RADS point totals that meet criteria for FNA
- Size should not be the primary criterion for deciding which nodule(s) to sample
- They discourage usage of the term dominant nodule, which is often applied to the largest lesion in the gland:
- Because it downplays the primary role of architecture in determining management
- If three or more nodules fall within ACR TI-RADS guidelines for biopsy, the two with the most suspicious appearance on the basis of point totals should be biopsied, even if they are not the largest
- Conversely, in a gland that contains multiple discrete nodules that do not meet criteria, there is little reason to subject the largest one to FNA solely because of its size
- Although malignancy cannot be definitively excluded under these conditions, sampling variation lessens the chance of detecting cancer because it would be impractical to biopsy every nodule
- Likewise, biopsy is usually not indicated in a gland that is replaced by multiple, confluent nodules of similar appearance
- Assessment of Cervical Lymph Nodes:
- Evaluation of cervical lymph nodes is a vital part of every thyroid sonographic examination
- Abnormal findings suggestive of cervical lymph node metastasis include:
- A globular shape
- Loss of the normal echogenic hilum
- Presence of peripheral rather than hilar flow
- Heterogeneity with cystic components
- Punctate echogenic foci that may represent microcalcifications
- They recommend FNA of suspicious nodes, in addition to up to two nodules that warrant biopsy on the basis of the ACR TI-RADS
#Arrangoiz #Surgeon #ThyroidSurgeon #CancerSurgeon #ThyroidExpert #EndorineSurgery #HeadandNeckSurgeon
