- From a practical standpoint, postoperatively, the eighth edition of the American Joint Committee on Cancer / tumor node metastasis (AJCC / TNM) staging system is used to predict disease-specific mortality and the American Thyroid Association (ATA) risk stratification system to predict the risk of recurrent or persistent disease
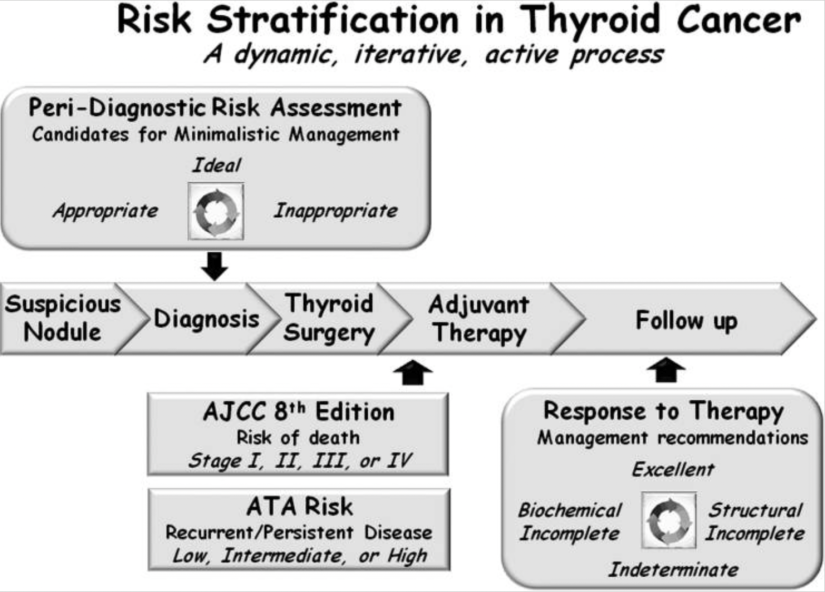
- These initial risk estimates are then modified over time:
- Using the descriptions from the ATA guidelines to define the patient’s response to therapy at any point during follow-up, as:
- Excellent:
- No evidence of persistent / recurrent disease
- Biochemically incomplete:
- Abnormal thyroglobulin (Tg) or rising Tg antibodies in the absence of identifiable structural disease
- Structurally incomplete:
- Structural evidence of persistent / recurrent disease
- Indeterminate:
- Nonspecific findings that cannot be confidently classified as benign or malignant
- Excellent:
- These modified risk estimates are then used to plan ongoing management
- Using the descriptions from the ATA guidelines to define the patient’s response to therapy at any point during follow-up, as:
- Recently, the move toward deferred intervention (active surveillance) of very low-risk thyroid cancers and a more minimalistic approach to thyroid surgery:
- Has expanded the risk-stratification horizon to include not only the intraoperative and postoperative time periods but also the peri-diagnostic time frame:
- That begins with the detection of a suspicious thyroid nodule
- Has expanded the risk-stratification horizon to include not only the intraoperative and postoperative time periods but also the peri-diagnostic time frame:
- In this peri-diagnostic period, it is important to identify low-risk thyroid cancers:
- That may be eligible for either an active surveillance management approach (with or without cytological confirmation) or for a minimalistic surgical intervention:
- Such as thyroid lobectomy without neck dissection
- That may be eligible for either an active surveillance management approach (with or without cytological confirmation) or for a minimalistic surgical intervention:
- Conversely, it is equally important to identify, in the peri-diagnostic period:
- Those patients who would be most likely to benefit from more aggressive initial interventions that could include:
- Total thyroidectomy:
- With or without prophylactic or therapeutic neck dissection
- Radioactive iodine treatment
- External beam radiation
- Upfront systemic therapy
- Total thyroidectomy:
- Those patients who would be most likely to benefit from more aggressive initial interventions that could include:
- It is also important to recognize that highly sensitive disease-detection tools can often detect small foci of papillary thyroid cancer that may not require immediate diagnosis and therapy:
- The 2015 ATA guidelines provided several specific examples where an observational management approach:
- Often without cytologic confirmation of disease, is recommended as the preferred or alternative management approach to small-volume disease:
- For example, an active surveillance observational management approach is allowed for carefully selected patients with either:
- Highly suspicious sub-centimeter asymptomatic thyroid nodules:
- Without the need for cytologic confirmation
- Biopsy-proven very low-risk thyroid cancers:
- Such as intra-thyroidal papillary microcarcinomas:
- In locations not adjacent to trachea or neurovascular structures without evidence of lymph node metastasis
- Such as intra-thyroidal papillary microcarcinomas:
- Furthermore, an observational management approach is also allowed for patients with persistent / recurrent small abnormal cervical lymph nodes
- Asymptomatic stable or slowly growing distant metastasis
- Stable or declining abnormal Tg or Tg antibodies
- Highly suspicious sub-centimeter asymptomatic thyroid nodules:
- For example, an active surveillance observational management approach is allowed for carefully selected patients with either:
- Often without cytologic confirmation of disease, is recommended as the preferred or alternative management approach to small-volume disease:
- The 2015 ATA guidelines provided several specific examples where an observational management approach:
- As it is clear that not all detectable findings require immediate diagnostic or therapeutic intervention:
- It is imperative that we develop a risk-stratification decision-making framework:
- To differentiate actionable findings from non-actionable findings
- It is imperative that we develop a risk-stratification decision-making framework:
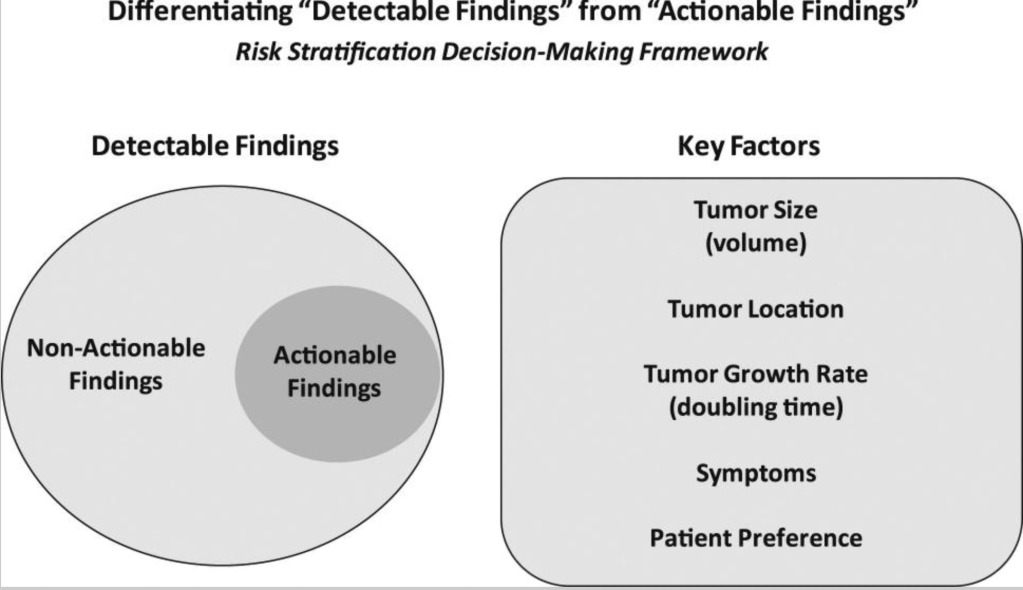
- Whether we are considering a highly suspicious sub-centimeter thyroid nodule without cytologic confirmation of disease, a biopsy-proven thyroid nodule with low-risk thyroid cancer, or persistent / recurrent disease in the neck or elsewhere:
- Consider five key factors that when taken together, allow us to predict the likelihood that a specific tumor focus represents clinically important disease:
- That may require additional evaluations, ongoing observation, or therapeutic intervention:
- Both tumor size and tumor location:
- Are the major factors that determine whether a tumor focus is likely to cause clinically substantial invasion into local structures, such as the recurrent laryngeal nerve, airway, gastrointestinal tract, major vessels, or other important structures
- A third important factor is the tumor growth rate (measured as tumor volume doubling time):
- With an observational management approach being much more appropriate for tumors either anticipated to have a slow tumor growth rate or with actual documented slow growth rates over time
- Obviously, tumors that are either symptomatic or likely to have symptomatic progression would be considered actionable
- Finally, patient preference plays a key role when deciding whether a particular lesion is actionable or non-actionable:
- As it is important to integrate the patient’s understanding of the risks and benefits of intervention vs observation with their value system and goals
- Both tumor size and tumor location:
- That may require additional evaluations, ongoing observation, or therapeutic intervention:
- In addition to providing initial guidance as to whether the detectable lesion is actionable at the time of detection:
- Ongoing re-evaluation of these same factors, using the basic concepts of dynamic-risk stratification:
- Can also assist the clinician in the determination of when it is time to transition from an observational management approach to active therapeutic intervention
- Thus, risk stratification has moved from a single postoperative static assessment of the risk of disease-specific mortality:
- To an all-encompassing evaluation of the patient that is continually modified over time:
- Beginning from the first detection of a suspicious thyroid nodule and continuing throughout the life of the patient
- To an all-encompassing evaluation of the patient that is continually modified over time:
- Ongoing re-evaluation of these same factors, using the basic concepts of dynamic-risk stratification:
- Consider five key factors that when taken together, allow us to predict the likelihood that a specific tumor focus represents clinically important disease:
#Arrangoiz #ThyroidSurgeon #ThyroidExpert #ThyroidCancer #DynamicRiskStratification #HeadandNeckSurgeon #CancerSurgeon
