- The facial nerve, (CN VII), is the seventh paired cranial nerve.
- The facial nerve is associated with the derivatives of the second pharyngeal arch.
- Motor:
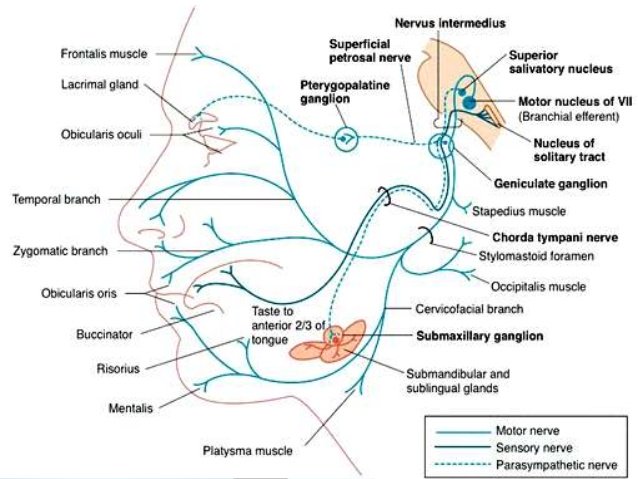
- Innervates the muscles of facial expression, the posterior belly of the digastric, the stylohyoid and the stapedius muscles.
- Sensory:
- A small area around the concha of the auricle.
- Special Sensory:
- Provides special taste sensation to the anterior 2/3 of the tongue.
- Parasympathetic:
- Supplies many of the glands of the head and neck, including:
- Submandibular and sublingual salivary glands.
- Nasal, palatine and pharyngeal mucous glands.
- Lacrimal glands.
- Supplies many of the glands of the head and neck, including:

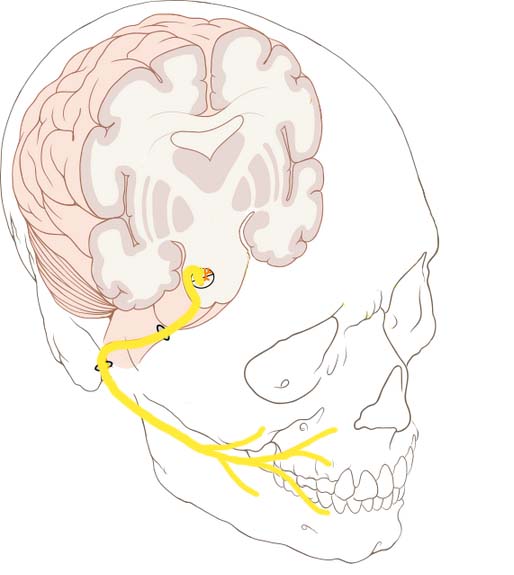
- Anatomical Course:
- The course of the facial nerve is very complex:
- There are many branches, which transmit a combination of sensory, motor and parasympathetic fibres.
- Anatomically, the course of the facial nerve can be divided into two parts:
- Intracranial:
- The course of the facial nerve through the cranial cavity, and the cranium itself.
- Extracranial:
- The course of the facial nerve outside the cranium, through the face and neck.
- Intracranial:
- The course of the facial nerve is very complex:
- Intracranial portion:
- The nerve arises in the pons, an area of the brainstem.
- It begins as two roots:
- A large motor root
- Small sensory root:
- The part of the facial nerve that arises from the sensory root is sometimes known as the intermediate nerve).
- The two roots travel through the internal acoustic meatus:
- A 1 cm long opening in the petrous part of the temporal bone.
- Here, they are in very close proximity to the inner ear.
- A 1 cm long opening in the petrous part of the temporal bone.
- Still within the temporal bone:
- The roots leave the internal acoustic meatus, and enter into the facial canal:
- The facial canal is a ‘Z’ shaped structure.
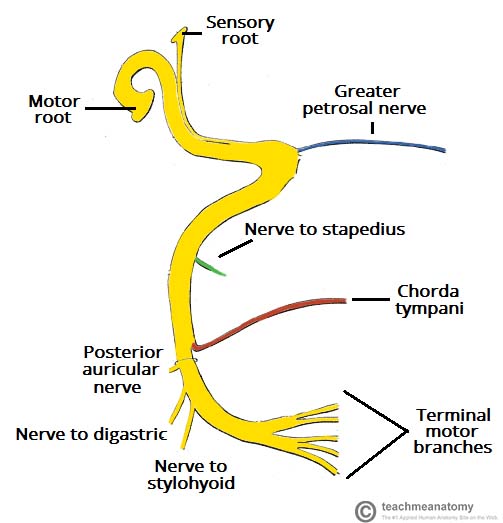
- Within the facial canal, three important events occur:
- Firstly the two roots fuse to form the facial nerve.-
- Next, the nerve forms the geniculate ganglion:
- A ganglion is a collection of nerve cell bodies
- Lastly, the nerve gives rise to:
- Greater petrosal nerve:
- Parasympathetic fibers:
- To mucous glands of the head and neck and lacrimal gland.
- Parasympathetic fibers:
- Nerve to stapedius muscle:
- Motor fibres to stapedius muscle of the middle ear.
- Chorda tympani:
- Special sensory fibers to the anterior 2/3 tongue
- Parasympathetic fibers to the submandibular and sublingual glands.
- Greater petrosal nerve:
- The roots leave the internal acoustic meatus, and enter into the facial canal:
- The facial nerve then exits the facial canal (and the cranium) via the stylomastoid foramen (in a lateral position):
- This is an exit located just posterior to the styloid process of the temporal bone.
- Extracranial portion of the facial nerve:
- After exiting the skull:
- The facial nerve turns superiorly to run just anterior to the outer ear.
- The first extracranial branch to arise is the posterior auricular nerve:
- It provides motor innervation to the some of the muscles around the ear.
- Immediately distal to this, motor branches are sent to the posterior belly of the digastric muscle and to the stylohyoid muscle.
- The main trunk of the nerve:
- Now termed the motor root of the facial nerve:
- Continues anteriorly and inferiorly into the parotid gland:
- The facial nerve does not contribute towards the innervation of the parotid gland:
- Which is innervated by the glossopharyngeal nerve).
- The facial nerve does not contribute towards the innervation of the parotid gland:
- Within the parotid gland, the nerve terminates by splitting into five branches:
- Temporal branch
- Zygomatic branch
- Buccal branch
- Marginal mandibular branch
- Cervical branch
- These branches are responsible for innervating the muscles of facial expression.
- Continues anteriorly and inferiorly into the parotid gland:
- Now termed the motor root of the facial nerve:
- After exiting the skull:
- Motor Functions:
- Branches of the facial nerve are responsible for innervating many of the muscles of the head and neck.
- All these muscles are derivatives of the second pharyngeal arch.
- The first motor branch arises within the facial canal:
- The nerve to stapedius muscle:
- The nerve passes through the pyramidal eminence to supply the stapedius muscle in the middle ear.
- Between the stylomastoid foramen, and the parotid gland, three more motor branches are given off:
- Posterior auricular nerve:
- Ascends in front of the mastoid process
- Innervates the intrinsic and extrinsic muscles of the outer ear.
- It also supplies the occipital part of the occipitofrontalis muscle.
- Nerve to the posterior belly of the digastric muscle:
- Innervates the posterior belly of the digastric muscle (a suprahyoid muscle of the neck):
- It is responsible for raising the hyoid bone.
- Innervates the posterior belly of the digastric muscle (a suprahyoid muscle of the neck):
- Nerve to the stylohyoid muscle:
- Innervates the stylohyoid muscle (a suprahyoid muscle of the neck):
- It is responsible for raising the hyoid bone.
- Innervates the stylohyoid muscle (a suprahyoid muscle of the neck):
- Posterior auricular nerve:
- Within the parotid gland, the facial nerve terminates by bifurcating into five motor branches:
- These innervate the muscles of facial expression:
- Temporal branch:
- Innervates the frontalis, orbicularis oculi and corrugator supercili
- Zygomatic branch:
- Innervates the orbicularis oculi.
- Buccal branch:
- Innervates the orbicularis oris, buccinator and zygomaticus muscles.
- Marginal Mandibular branch:;
- Innervates the mentalis muscle.
- Innervates the depressor anguli oris and the depressor labii inferioris
- Cervical branch:;
- Innervates the platysma.
- Temporal branch:
- These innervate the muscles of facial expression:
- The nerve to stapedius muscle:
- Special sensory functions:
-
The chorda tympani branch of the facial nerve is responsible for innervating the anterior 2/3 of the tongue with the special sense of taste:
- The nerve arises in the facial canal
- Travels across the bones of the middle ear
- Exiting via the petrotympanic fissure, and entering the infratemporal fossa:
-
Here, the chorda tympani ‘hitchhikes’ with the lingual nerve:
-
The parasympathetic fibres of the chorda tympani stay with the lingual nerve:
-
But the main body of the nerve leaves to innervate the anterior 2/3 of the tongue.
-
-
-
-
-
Parasympathetic functions:
-
The parasympathetic fibres of the facial nerve are carried by the greater petrosal and chorda tympani branches:
-
Greater Petrosal Nerve:
-
The greater petrosal nerve arises immediately distal to the geniculate ganglion within the facial canal:
-
It then moves in anteromedial direction:
-
Exiting the temporal bone into the middle cranial fossa.
-
From here, its travels across (but not through) the foramen lacerum:
-
Combining with the deep petrosal nerve to form the nerve of the pterygoid canal:
-
The nerve of pterygoid canal then passes through the pterygoid canal (Vidian canal) to enter the pterygopalatine fossa, and synapses with the pterygopalatine ganglion.
-
Branches from this ganglion then go on to provide parasympathetic innervation to the mucous glands of the oral cavity, nose and pharynx, and the lacrimal gland.
-
-
-
-
-
-
-
-
-
- Chorda Tympani:
- The chorda tympani also carries some parasympathetic fibres:
- These combine with the lingual nerve (a branch of the trigeminal nerve) in the infratemporal fossa and form the submandibular ganglion:
- Branches from this ganglion travel to the submandibular and sublingual salivary glands.
- These combine with the lingual nerve (a branch of the trigeminal nerve) in the infratemporal fossa and form the submandibular ganglion:
- The chorda tympani also carries some parasympathetic fibres:

Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon / surgical oncologist and is a member of Sociedad Quirúrgica S.C at the America British Cowdray Medical Center in Mexico City:
-
He is an expert in the management of head and neck cancers.