My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
Retrospective studies of SLN biopsyvalidated by ALND:
Show that the success rate of SLN biopsy after neoadjuvant chemotherapy is:
About 90%:
Somewhat less than for SLN biopsy overall
The false-negative rate is about 10%:
Comparable to SLN biopsy overall)
For patients with proven nodal metastases:
The prospective American College of Surgeons Oncology Group (ACOSOG) Z1071 and SENTinel NeoAdjuvant (SENTINA) trial:
Observe success rates of:
85% to 90%:
False-negative rates of :
12% to 14% for SLN biopsy
In both studies the false-negative rate was minimized:
By dual-agent mapping (dye plus isotope) and the removal of greater than 2 SLN
These results suggest that ALND may not be required for node-positive patients postchemotherapy when a technically satisfactory SLN biopsy is negative:
Patients with any positive axillary nodes postchemotherapy require ALND and are at increased risk of locoregional recurrence.
A new trial:
Alliance 11202 is randomizing node-positive patients whose SLN remain positive after neoadjuvant chemotherapy to:
Boughey JC, Suman VJ, Mittendorf EA, et al. Sentinel lymph node surgery after neoadjuvant chemotherapy in patients with node-positive breast cancer: the ACOSOG Z1071 (Alliance) clinical trial. JAMA. 2013;310:1455-1461.
Houssami N, Macaskill P, von Minckwitz G, et al. Meta-analysis of the association of breast cancer subtype and pathologic complete response to neoadjuvant chemotherapy. Eur J Cancer. 2012;48:3342-3354.
Kuehn T, Bauerfeind I, Fehm T, et al. Sentinel-lymph-node biopsy in patients with breast cancer before and after neoadjuvant chemotherapy (SENTINA): a prospective, multicentre cohort study. Lancet Oncol. 2013;14:609-618.
Mamounas EP, Anderson SJ, Dignam JJ, et al. Predictors of locoregional recurrence after neoadjuvant chemotherapy: results from combined analysis of National Surgical Adjuvant Breast and Bowel Project B-18 and B-27. J Clin Oncol. 2012;30:3960-3966.
Mauri D, Pavlidis N, Ioannidis JPA. Neoadjuvant versus adjuvant systemic treatment in breast cancer: a meta-analysis. J Natl Cancer Inst. 2005;97:188-194.
van Deurzen CH, Vriens BE, Tjan-Heijnen VC, et al. Accuracy of sentinel node biopsy after neoadjuvant chemotherapy in breast cancer patients: a systematic review. Eur J Cancer. 2009;45:3124-3130.
👉Rodrigo Arrangoiz MS, MD, FACScirujano oncology y cirujanode mamáde Sociedad Quirúrgica S.C en el America British Cowdray Medical Center en la ciudad de Mexico:
Es experto en el manejo del cáncer de mama.
👉Esmiembrode la American Society of Breast Surgeons:
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012
• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
Remains the standard of care in the staging of clinically node-negative patients,:
And is endorsed in the 2014 update of the American Society of Clinical Oncology clinical practice guidelines.
For patients undergoing neoadjuvant chemotherapy:
The optimal timing of SLNB (pre- or postchemotherapy) is debated:
Concerns regarding performance of SLNB after neoadjuvant chemotherapy:
Have historically centered around the ability to both identify a sentinel node and the sensitivity of the SLNB to predict non-SLN involvement:
Particularly among clinically node-positive patients:
Whose lymphatic pathways may be occluded by tumorand/or scarring resultant from chemotherapy.
However, over the past 10 years, a number of prospective studies have shown:
A high accuracy of SLNB in the postneoadjuvant setting in patients presenting as clinically node negative prior to receiving neoadjuvant chemotherapy.
Proponents of SLNB subsequent to neoadjuvant chemotherapy tout the fact that:
This spares the patient another surgical procedure and that SLN posttreatment is more meaningful for predicting prognosis.
In a small, early study published in 2000:
51 patients (postneoadjuvant chemotherapy) underwent SLNB followed by completion ALND:
SLN identification rate was high at 94%
The false-negative rate was low at 5.8%
In 2008, the Austrian Sentinel Node Study group published their results on 167 neoadjuvant chemotherapy patients who underwent postchemotherapy SLNB followed by completion ALND:
SLNB was only offered to those with clinically negative nodes after chemotherapy
SLN identification rate was:
Highest with use of both vital blue dye and radiocolloid:
88% identification with dual tracer
False-negative rate of the SLNB was:
Only 8%
In the larger, multicenter National Surgical Adjuvant Breast and Bowel Project (NSABP) B-27 trial:
428 patients underwent SLNB before a required ALND
Successful identification of a SLN was again high:
89% if radiocolloid was used:
The 10% false-negative rate comparable to the rate observed for prechemotherapy SLNB in multicenter studies
If SLNB is performed and the SLN(s) is positive prior to neoadjuvant chemotherapy:
A SLNB should not be repeated subsequent to chemotherapy:
The large, multicenter SENTinel NeoAdjuvant (SENTINA) trial:
Arm B demonstrated that in this setting, identification rates were:
Low (61%)
False-negative rates unacceptably high (52%)
👉Rodrigo Arrangoiz MS, MD, FACScirujano oncology y cirujanode mamáde Sociedad Quirúrgica S.C en el America British Cowdray Medical Center en la ciudad de Mexico:
Es experto en el manejo del cáncer de mama.
👉Esmiembrode la American Society of Breast Surgeons:
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012
• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016
#Arrangoiz
#Surgeon
#Cirujano
#SurgicalOncologist
#CirujanoOncologo
#BreastSurgeon
#CirujanodeMama
#CancerSurgeon
#CirujanodeCancer
References:
Breslin TM, Cohen L, Sahin A, et al. Sentinel lymph node biopsy is accurate after neoadjuvant chemotherapy for breast cancer. J Clin Oncol. 2000;18:3480-3486.
Kuehn T, Bauerfeind I, Fehm T, et al. Sentinel-lymph-node biopsy in patients with breast cancer before and after neoadjuvant chemotherapy (SENTINA): a prospective, multicentre cohort study. Lancet Oncol. 2013;14:609-618.
Mamounas EP, Brown A, Anderson S, et al. Sentinel node biopsy after neoadjuvant chemotherapy in breast cancer: results from National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J Clin Oncol. 2005;23:2694-2702.
Tan VKM, Goh BKP, Fook-Chong S, et al.The feasibility and accuracy of sentinel lymph node biopsy in clinically node-negative patients after neoadjuvant chemotherapy for breast cancer—a systematic review and meta-analysis. J Surg Oncol. 2011;104:97-103.
Tausch C, Konstantiniuk P, Kugler F, et al; Austrian Sentinel Node Study Group. Sentinel lymph node biopsy after preoperative chemotherapy for breast cancer: findings from the Austrian Sentinel Node Study Group. Ann Sur Oncol. 2008;15:3378-3383.
van Deurzen CH, Vriens BE, Tjan-Heijnen VC, et al. Accuracy of sentinel node biopsy after neoadjuvant chemotherapy in breast cancer patients: a systematic review. Eur J Cancer. 2009;45:3124-3130.
Xing Y, Foy M, Cox DD, et al. Meta-analysis of sentinel lymph node biopsy after preoperative chemotherapy in patients with breast cancer. Br J Surg. 2006;93:539-546.
👉This study suggests that the use of a standardized dose for prescribing the initial dose of levothyroxine after surgery based on the actual body weight frequently will result in either too high or too low thyroid levels.
👉In overweight and obese patients, a much lower mcg/kg body weight dose should be used, while a higher dose should be used in patients with a normal BMI.
👉These results will benefit patients after thyroid surgery as they may start taking a more appropriate dose of levothyroxine as soon as possible after thyroid surgery, and require fewer blood tests for dose adjustments.
👉Multiple endocrine neoplasia type 2 (MEN2) is subclassified into two distinct syndromes: types 2A (MEN2A) and 2B (MEN2B).
👉Within MEN2A, there are four variants:
● Classical MEN2A
● MEN2A with cutaneous lichen amyloidosis (CLA)
● MEN2A with Hirschsprung disease (HD)
● Familial medullary thyroid cancer (FMTC)
👉In both MEN2A and MEN2B, there is an occurrence of multicentric tumor formation in all organs where the RET proto-oncogene is expressed.
👉The thyroid, parathyroid, adrenal glands, and accessory adrenals are at risk for developing tumors that may reduce life expectancy and quality of life.
Multiple endocrine neoplasia type 2A
Classical MEN2A
👉Classical multiple endocrine neoplasia 2A (MEN2A) is the most common MEN2A variant.
👉It is a heritable predisposition to medullary thyroid cancer (MTC), pheochromocytoma, and primary parathyroid hyperplasia.
👉The respective frequency of these tumors in classical MEN2A is over 90% for MTC, approximately 10% to 50% for pheochromocytoma, and 10% to 20% for multigland parathyroid hyperplasia.
👉The frequency of the development of MTC, pheochromocytoma, and parathyroid hyperplasia depends upon the specific RET mutation.
MEN2A with cutaneous lichen amyloidosis
👉CLA (also known as lichen planus amyloidosis [LPA]) has been described in some families with multiple endocrine neoplasia 2A (MEN2A), predominantly those with the RET codon 634 mutation, although it has also been reported in a patient with a codon 804 mutation.
👉The diagnosis of CLA may precede the onset of clinically evident MTC (Image).
👉Patients with this variant develop pheochromocytomas and parathyroid hyperplasia with a similar frequency as those with classical MEN2A.
The skin lesion is usually described as pruritic, scaly, papular, pigmented, and located in the interscapular region or on the extensor surfaces of the extremities. Amyloid deposition has been documented histologically.
MEN2A with Hirschsprung disease (HD)
👉HD is a motor disorder of the gut that is caused by the failure of neural crest cells (precursors of enteric ganglion cells) to migrate completely during intestinal development.
👉The resulting aganglionic segment of the colon fails to relax, causing a functional obstruction.
👉At least eight genetic mutations have been identified in patients with HD.
👉The predominant gene affected is the RET proto-oncogene.
👉RET malfunction accounts for at least 50% of familial and 20% of sporadic cases of HD.
👉In one study, the prevalence of HD in MEN2 was 7.5%.
👉The frequency of HD in MEN2A depends upon the specificRET mutation.
👉The co-occurrence of HD and MEN2A is predominantly associated withRETmutations involving codons 609, 611, 618, and 620.
👉In such patients, HD may be the first presentation of MEN2A.
👉Patients with this variant of MEN2A develop MTC, pheochromocytomas, and parathyroid hyperplasia with a similar frequency as those with classical MEN2A.
Familial medullary thyroid cancer
👉FMTC is a variant of MEN2A in which there is a strong predisposition to MTC but not the other clinical manifestations of MEN2A (or 2B).
👉The clinical distinction of FMTC from MEN2A may be difficult on statistical grounds in small families; even in some large kindreds, the clinical designation of FMTC has been changed to MEN2A after the diagnosis of pheochromocytoma or hyperparathyroidism in a family member.
👉Because FMTC is the most limited variant of MEN2, making the wrong diagnosis of FMTC could result in missing a pheochromocytoma in a patient with MEN2.
👉Therefore, an FMTC kindred should be defined using the following rigorous criteria:
● More than 10 carriers in the kindred
● Multiple carriers or affected members over the age of 50 years
● An adequate medical history, particularly in older family members
👉Why pheochromocytomas and hyperparathyroidism infrequently develop in these families is still unknown since many FMTC and MEN2A families carry identical RET mutations.
👉In rare families, both HD and FMTC appear to segregate.
👉In a report summarizing data from 250 Italian kindreds with hereditary MTC, the prevalence of the FMTC phenotype amongRET mutation carriers was higher than MEN2A and MEN2B (57%, 34% and 6.8%, respectively).
👉This may be related to the introduction ofRETscreening in the work-up of apparently sporadic MTC and the more extensive search forRETmutations in non-hot spot regions of the gene.
Multiple endocrine neoplasia type 2B
👉The frequency of MEN2B has been estimated at roughly 6% of all MEN2 patients.
👉MEN2B shares the inherited predisposition to MTC and pheochromocytoma that occurs in MEN2A.
👉On the other hand, parathyroid hyperplasia is not a feature of this disorder.
👉There are additional important clinical differences.
👉Patients with MEN2B tend to have mucosal neuromas, typically involving the lips and tongue, and intestinal ganglioneuromas.
👉Disturbances of colonic function are common, including chronic constipation and megacolon.
👉Many of these patients have development abnormalities, a Marfanoid habitus, and myelinated corneal nerves.
👉MTC is the most common component of the MEN2B syndrome.
👉Furthermore, the tumor is often more aggressive and of earlier onset than in MEN2A; as a result, early diagnosis and prevention are particularly critical.
What is Head and Neck Surgery?:
It is asurgical sub-specialtythat deals mainly with benign and malignant tumors of the head and neck region, including:
The scalp, facial region, eyes, ears, nose, nasal fossae, paranasal sinuses, oral cavity, pharynx (nasopharynx, oropharynx, hypopharynx), larynx (supraglotic larynx, glottis larynx, subglotic larynx), thyroid gland, parathyroid gland, salivary glands (parotid glands, submandibular glands, sublingual glands, minor salivary glands), soft tissues of the neck, skin of the head and neck region.
Thehead and neck surgeon’s work area:
Does not cover tumors or diseases of the brain and other areas of the central nervous system or those of the cervical spine:
This is the neurosurgeon field.
Among thediagnostic proceduresperformed by the head and neck surgeon, are the following:
Nasopharyngolaryngoscopy:
Performed toexamine, evaluate and, possibly perform a biopsy, of oral cavity, pharyngeal and laryngeal lesions.
The surgeries most commonly performed by the head and neck surgeon are:
Total or near total thyroidectomies
Hemithryoidectomies (lobectomies)
Comprehensive neck dissections
Selective neck dissections
Maxillectomies:
Total maxillectomy
Subtotal maxillectomy
Infrastructure maxillectomy
Suprastructure maxillectomy
Medial maxillectomy
Mandibulectomy:
Segmental
Marginal
Tracheostomy
Salivary gland surgeries:
Parotid gland operations:
Limited superficial parotidectomy with identification and preservation of the facial nerve
Superficial parotidectomy with identification and preservation of the facial nerve
Near total parotidectomy with identification and preservation of the facial nerve
Total parotidectomy
Submandibular gland resection
Sublingual gland resection
Resection of tumors of the oral cavity:
Glossectomy
Resection of the floor of the mouth tumors
Resection of tumors of the pharynx
Resection of tumors of the larynx
Split-thickness skin grafts
Full-thickness skin grafts
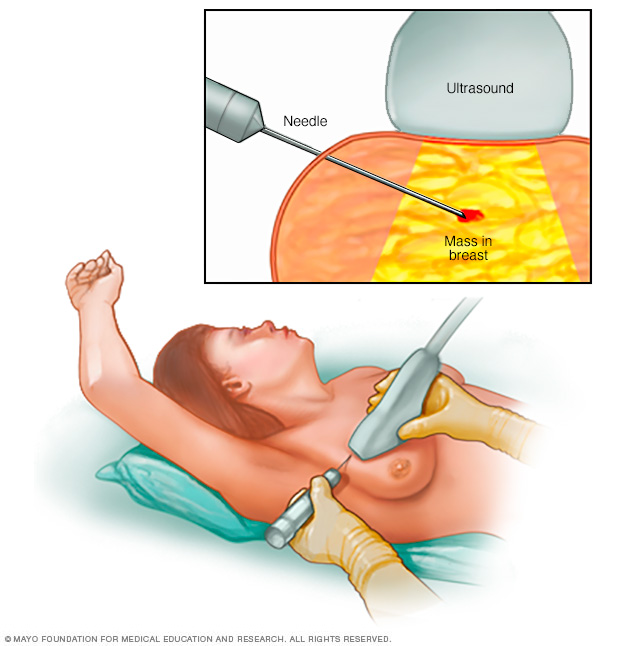
Sentinel lymph node mapping and sentinel lymph node biopsy
Resection of malignant skin tumors (BCC, SCC, melanoma) of the head and neck region
Theformation of the head and neck surgeon includes masteringthe following subjects:
Surgical Anatomy
History and Basic Principles of Head and Neck Surgery
Epidemiology, Etiology, and Pathology of Head and Neck Diseases
Diagnostic Radiology of the Head and Neck Region
Tumors of the Scalp, Skin and Melanoma
Eyelids and Orbit
Nasal Cavity and Paranasal Sinuses
Skull Base and Temporal Bone
Lips and Oral Cavity
Pharynx and Esophagus
Larynx and Trachea
Cervical Lymph Nodes
Thyroid and Parathyroid Glands
Salivary Glands
Neurogenic Tumors and Paragangliomas
Soft Tissue Tumors
Bone Tumors and Odontogenic Lesions
Reconstructive Surgery
Oncologic Dentistry and Maxillofacial Prosthetics
Principles of Radiation Oncology
Principles of Chemotherapy
Molecular Oncology, Genomics and Immunology
Nutrition
Biostatistic
Rodrigo Arrangoiz MS, MD, FACSa head and neck surgeon / endocrine surgeon / surgical oncologist and is a member of Sociedad Quirúrgica S.C at the America British Cowdray Medical Center in Mexico City:
Rodrigo Arrangoiz MS, MD, FACS:
Is a member of theAmerican Head and Neck Society
He is a member of the American Thyroid Association:
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012
• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
👉Capecitabine isoften used to treat breast cancer, but the best use of capecitabine is open for discussion.
👉According to a large meta-analysis of the effects of capecitabine in early breast cancer, capecitabine improves disease-free and overall survival for patients with triple-negative breast cancer, but only when it is added to other systemic therapies and not when it is used as a substitute.
👉The results of the meta-analysis were presented at the 2019 San Antonio Breast Cancer Symposium (SABCS) by Marion van Mackelenbergh, MD, of the University of Kiel, Germany.
👉Capecitabine alone did not alter overall disease-free survival, but when added to other systemic therapies, there was an improvement.
👉Overall survival was also improved when capecitabine was given in addition to other therapies.
👉There is no evidence supporting a predictive value of capecitabine-specific adverse events on outcome.
👉It can be concluded that the addition of capecitabine to other treatment may be recommended for patients with triple-negative.
👉The meta-analysis showed no data comparing the effects of capecitabine with carboplatin in triple-negative breast cancer.
👉One trial is recruiting patients to evaluate this in the post-neoadjuvant setting.
👉The effect of capecitabine compared with other systemic therapies, including carboplatin, remains to be investigated.
👉Capecitabine is approved by the U.S. Food and Drug Administration (FDA) for use as monotherapy or in combination with docetaxel in metastatic breast cancer.
👉The meta-analysis results addressed its use in early breast cancer.
👉Several randomized trials have evaluated the effect of capecitabine in early breast cancer, mainly in high-risk patients.
👉The German Breast Group investigators sought to examine the effect of capecitabine in patients with early breast cancer on disease-free survival as the primary objective; secondary endpoints included the effect of capecitabine on overall survival and to determine whether there was an interaction between capecitabine-specific toxicity and treatment effect.
👉Study Details👈
👉The meta-analysisincluded individual patient data from 15,457 patients enrolled in 12 randomized controlled trials; 7,983 patients with early breast cancer were treated with capecitabine, and 7,474 patients were in the control arms.
👉Five of the trials included in the meta-analysis addressed capecitabine given instead of other therapies, and seven evaluated the use of capecitabine in addition to other therapies.
👉The analysis was performed on the overall study population and in two predefined subsets: patients who received capecitabine in addition to other therapies and those who received capecitabine instead of another systemic treatment.
👉The median age of patients at initial diagnosis was 53 years.
👉Nearly three-quarters of patients had nodal involvement; 56% presented with tumor stage II disease; about 68% had hormone receptor–positive disease; 45% had high-grade disease; 15% had HER2-positive breast cancer.
👉About 80% of the patients were treated in the adjuvant setting and almost 20%, in the neoadjuvant setting.
👉Key Findings👈
👉Among the entiredata set, there was no significant effect of capecitabine alone on disease-free survival, but a significant benefit was observed in the patients who received capecitabine in addition to other systemic therapies (hazard ratio [HR] = 0.888, 95% confidence interval [CI[ = 0.817–0.965).
👉Only the CREATE-X trial had positive results for disease-free survival, and no benefit of capecitabine on disease-free survival was observed when capecitabine was given instead of another treatment.
👉A slight benefit for capecitabine was observed in overall survival for the total data set (HR = 0.892, 95% CI = 0.824–0.965;P= .005), which was more pronounced when capecitabine was added to other systemic therapies (HR = 0.837, 95% CI = 0.751–0.933;P= .001).
👉Only the CREATE-X and USON 01062 trials were positive for overall survival.
👉There was no overall survival benefit [in the meta-analysis] when capecitabine was substituted for another systemic therapy.
👉In patients with triple-negative breast cancer, capecitabine improved disease-free survival by 18% when added to standard chemotherapy and overall survival by 22% (P= .004 for both analyses).
👉Only benefit of capecitabine was observed in the triple-negative breast cancer overall cohort and when capecitabine was added [to another therapy].
👉No benefit was observed in triple-negative breast cancer when capecitabine was given instead of another systemic therapy.
👉The most common grade 3 and 4 toxicities associated with capecitabine were mucositis, hand-foot syndrome, and diarrhea.
👉No significant associations were reported between capecitabine-specific toxicities and treatment benefit.
👉A recent consensus statement from the Society of Surgical Oncology and American Society for Radiation Oncology has indicated that “no ink on tumor” is an adequate margin for patients undergoing lumpectomy for invasive breast cancer.
👉This recommendation applies regardless of the molecular phenotype.
👉Although the triple-negative phenotype has been associated with a higher local recurrence rate than other phenotypes, there is no evidence to indicate that these patients benefit from wider excision, including mastectomy, for early-stage breast cancer.
👉The American College of Surgeons Oncology Group Z0011 trial established that for patients with clinical T1 to T2, N0 breast cancer found to have only 1 or 2 positive sentinel nodes who will receive whole breast irradiation as a component of breast conserving therapy, a completion ALND is not required.
👉In that trial, patients were randomized to ALND versus no further surgery, and at a median follow-up of 6.3 years, there were no differences between the groups with respect to locoregional recurrence.
👉Regional recurrences in the ipsilateral axilla were similar between study arms with four (0.9%) patients in the sentinel lymph node dissection alone group compared with two (0.5%) in the ALND group.
👉Although the Z0011 trial accrued only 16% ER/PR-negative patients, there was no indication of a higher risk of axillary recurrence among these patients.
👉REFERENCES
Adkins FC, Gonzalez-Angulo AM, Lei X, et al. Triple-negative breast cancer is not a contraindication for breast conservation.Ann Surg Oncol. 2011;18:3164-3173.
Chung A, Gangi A, Mirocha J, et al. Applicability of the ACOSOG Z0011 criteria in women with high-risk node-positive breast cancer undergoing breast conserving surgery.Ann Surg Oncol. 2015;22:1128-1132.
Giuliano AE, McCall L, Beitsch P, et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: the American College of Surgeons Oncology Group Z0011 randomized trial.Ann Surg. 2010;252:426-432.
Hwang ES, Lichtensztajn DY, Gomez SL, et al. Survival after lumpectomy and mastectomy for early stage invasive breast cancer: the effect of age and hormone receptor status.Cancer. 2013;119:1402-1411.
Moran MS, Schnitt SJ, Giuliano AE, et al. Society of Surgical Oncology-American Society for Radiation Oncology consensus guideline on margins for breast-conserving surgery with whole-breast irradiation in stages I and II invasive breast cancer.J Clin Oncol. 2014;32:1507-1515.
👉Rodrigo Arrangoiz MS, MD, FACScirujano oncology y cirujanode mamáde Sociedad Quirúrgica S.C en el America British Cowdray Medical Center en la ciudad de Mexico:
Es experto en el manejo del cáncer de mama.
👉Esmiembrode la American Society of Breast Surgeons:
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012
• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
👉Although breast cancer with isolated intramammary lymph node metastases is considered stage II disease, few studies have explored the clinical significance of this finding.
👉In one large retrospective review of 7140 patients, intramammary lymph nodes were identified in 2% of patients.
👉Among these patients, the intramammary nodes were positive in 35/151, or 24% .
👉Axillary metastases were identified in 61% of intramammary node-positive patients.
👉Among those with a positive intramammary node but negative axillary sentinel node, completion axillary node dissection revealed no additional axillary metastases.
👉Another large retrospective review also found that the majority (81%) of patients with intramammary node metastases also had axillary metastases.
👉On both univariate and multivariate analysis, when compared to patients without intramammary nodal tumor deposits, the presence of intramammary node metastases was significantly associated with worse disease-free survival (89% vs 54%, p=0.001).
👉Although important for disease staging and prognosis, management of the axilla should rely on axillary node status, and axillary node dissection should not be performed on the basis of intramammary node positivity alone.
👉REFERENCES
Pugliese MS, Stempel MM, Cody HS 3rd, et al. Surgical management of the axilla: do intramammary nodes matter? Am J Surg. 2009;198:532-537.
Shen J, Hunt KK, Mirza NQ, et al. Intramammary lymph node metastases are an independent predictor of poor outcome in patients with breast carcinoma.Cancer. 2004;101:1330-1337.
View Response
👉Rodrigo Arrangoiz MS, MD, FACScirujano oncology y cirujanode mamáde Sociedad Quirúrgica S.C en el America British Cowdray Medical Center en la ciudad de Mexico:
Es experto en el manejo del cáncer de mama.
👉Esmiembrode la American Society of Breast Surgeons:
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012
• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center: