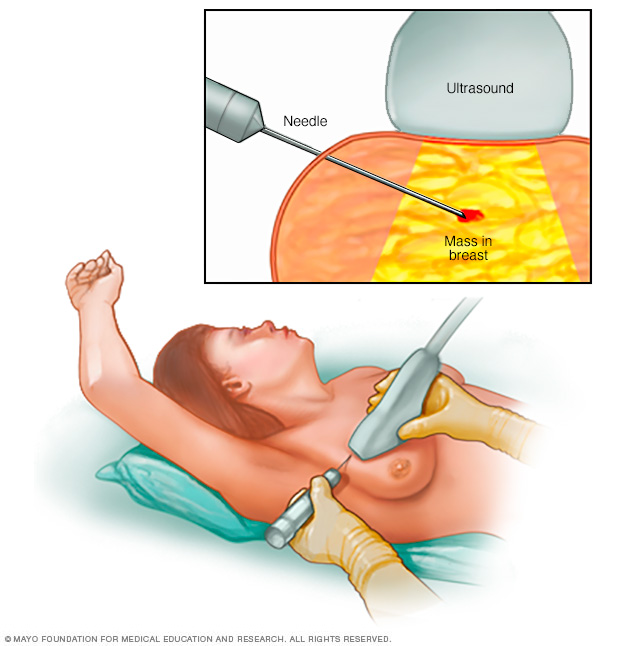
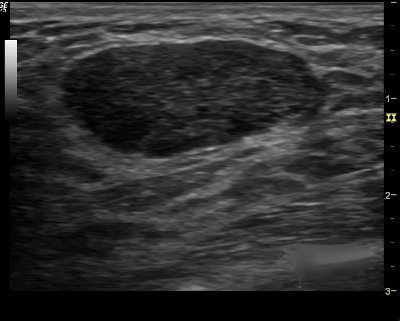
1. You first evaluate the lesion for any of the ten malignant signs identified on ultrasound:
-
- Shadowing
- Hypoechoic echotexture
- Spiculation
- Angular margins
- Thick echogenic capsule
- Taller than wider
- Microlobulation
- Duct extension
- Branching pattern
- Calcifications
-
2. Finding none, you move on to the second step in the evaluation process and specifically look for one of the three strictly defined benign signs, and if any of them is found, the lesion can be considered BI-RADS 3.
-
-
- The three benign findings defined by Stavros are:
-
-
-
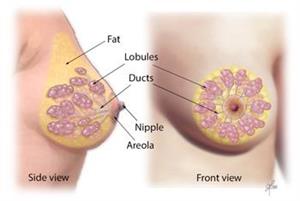
- A purely hyperechoic lesion with no hypoechoic area larger than a normal duct or lobule.
- Elliptical, wider than tall, well-circumscribed and thin echogenic capsule.
- Gently lobulated, wider than tall, well-circumscribed and thin echogenic capsule.
– Combining the elliptical or gently lobulated shapes with the presence of a complete, thin echogenic capsule is necessary because many circumscribed carcinomas and most ductal carcinoma in situ are encompassed in a thin, echogenic capsule.


👉Rodrigo Arrangoiz MS, MD, FACS cirujano oncology y cirujano de mamá de Sociedad Quirúrgica S.C en el America British Cowdray Medical Center en la ciudad de Mexico:
-
Es experto en el manejo del cáncer de mama.

👉Es miembro de la American Society of Breast Surgeons:

Training:
• General surgery:
• Michigan State University:
• 2004 al 2010

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016


#Arrangoiz
#Surgeon
#Cirujano
#SurgicalOncologist
#CirujanoOncologo
#BreastSurgeon
#CirujanodeMama
#CancerSurgeon
#CirujanodeCancer



 👉Rodrigo Arrangoiz MS, MD, FACScirujano oncology y miembro de Sociedad Quirúrgica S.C en el America British Cowdray Medical Center en la ciudad de Mexico:
👉Rodrigo Arrangoiz MS, MD, FACScirujano oncology y miembro de Sociedad Quirúrgica S.C en el America British Cowdray Medical Center en la ciudad de Mexico: