👉There is evidence that environmental factors, such as parity and alcohol consumption, can modify breast cancer risk associated with common, low-penetrance variant alleles (e.g., LSP1-rs3817198 and CASP8-rs17468277).
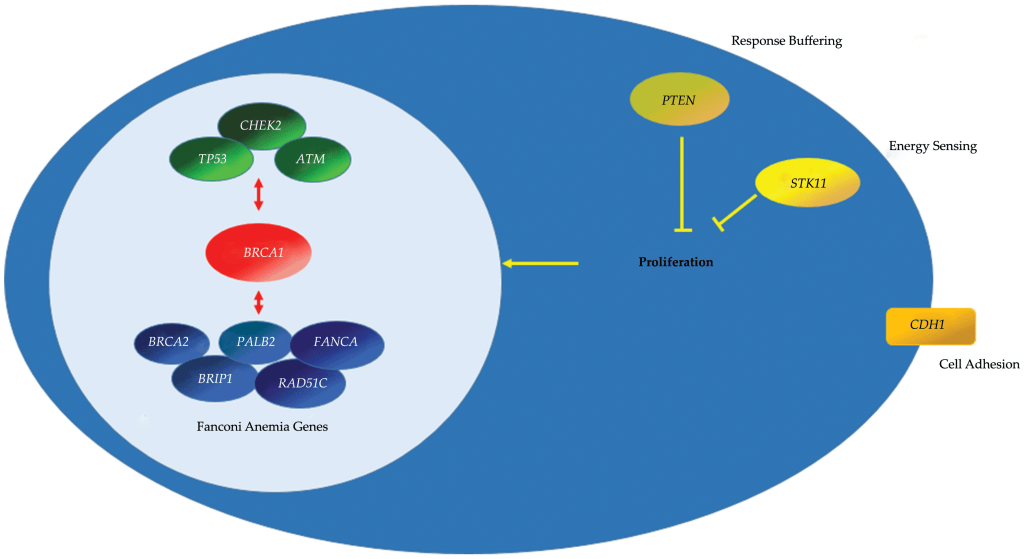
👉Alcohol consumption is of particular interest because the metabolic by-product, acetaldehyde, has been shown to damage DNA, leading to BRCA1 activation.
👉Nevertheless, available epidemiologic data have not identified an association between alcohol consumption and breast cancer risk among BRCA1 or BRCA2 gene mutation carriers.
👉In general, convincing examples of gene-environment interactions are rare for autosomal dominant breast cancer predisposition syndromes, and where such data exist, the effects are inconsistent.
👉A recent review of the literature and meta-analysis suggested that late age at first live birth and lactation reduced breast cancer risk in BRCA1 mutation carriers, but data were insufficient for BRCA2 mutation carriers.
👉An alternative interpretation of the available data is that parity and age at first live birth do not modify breast cancer risk in BRCA1 mutation carriers, although lactation may reduce risk.
👉There is also evidence suggesting that for BRCA2 mutation carriers, pregnancies do not reduce breast cancer risk the same way they do in nonmutation carriers and may even increase risk, with greater risk at later ages at first live birth.
👉Similar to other women, combined hormone replacement therapy (HRT) with estrogen and progestin seems to increase breast cancer risk in mutation carriers, whereas estrogen-only therapy does not.
👉Finally, weight gain in adulthood and higher caloric intake have been associated with increased breast cancer risk and earlier age at diagnosis in BRCA1 and BRCA2 mutation carriers.
👉It seems reasonable to counsel BRCA1 and BRCA2 mutation carriers to avoid weight gain in adulthood.
👉However, given the inconsistency of available data and interpretation of these data, childbearing decisions should be left to the individual but lactation encouraged as long as it is not considered a substitute for risk-reducing mastectomy.
#Arrangoiz #BreastSurgeon #BreastCancer #CancerSurgeon #SurgicalOncologist