👉The soft palate is located in the oropharynx posteriorly.
👉It is mobile, and comprised of muscle fibres covered by a mucous membrane (stratified squamous epithelium).
👉The soft palate is a musculoaponeurotic curtain that hangs down from the posterior border of the hard palate and maintains velopharyngeal competence during speech and swallowing.
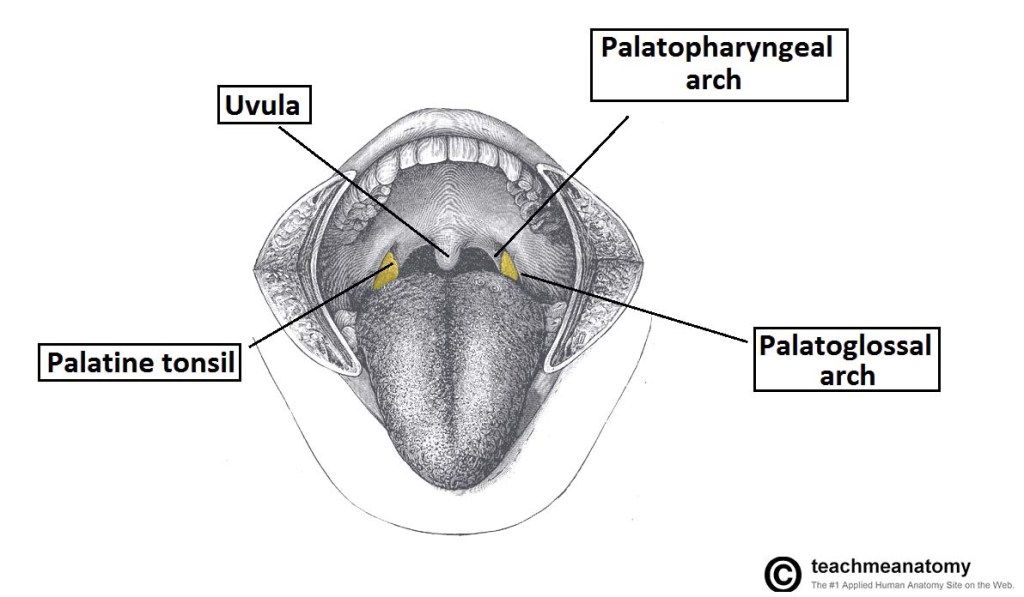
👉The midline uvula is located on the free inferior border and the sides blend into the faucial arches that attach to the lateral pharyngeal walls.
👉The mucosa of the soft palate is of the stratified squamous epithelium.
👉The submucosa of the soft palate contains minor salivary glands that mainly secret mucus.
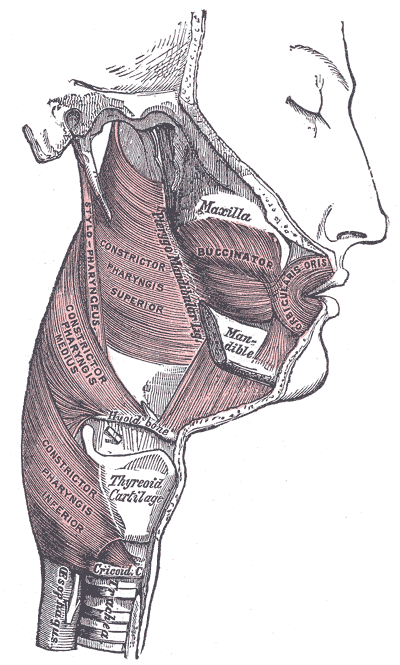
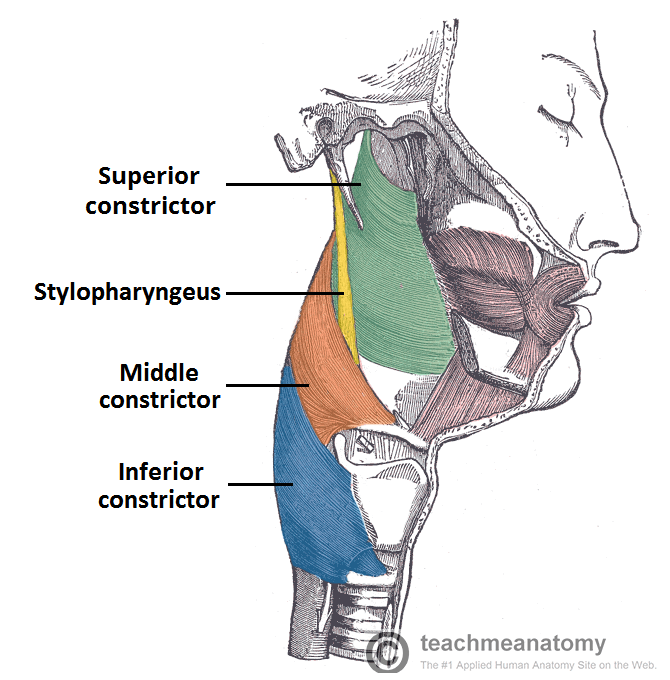
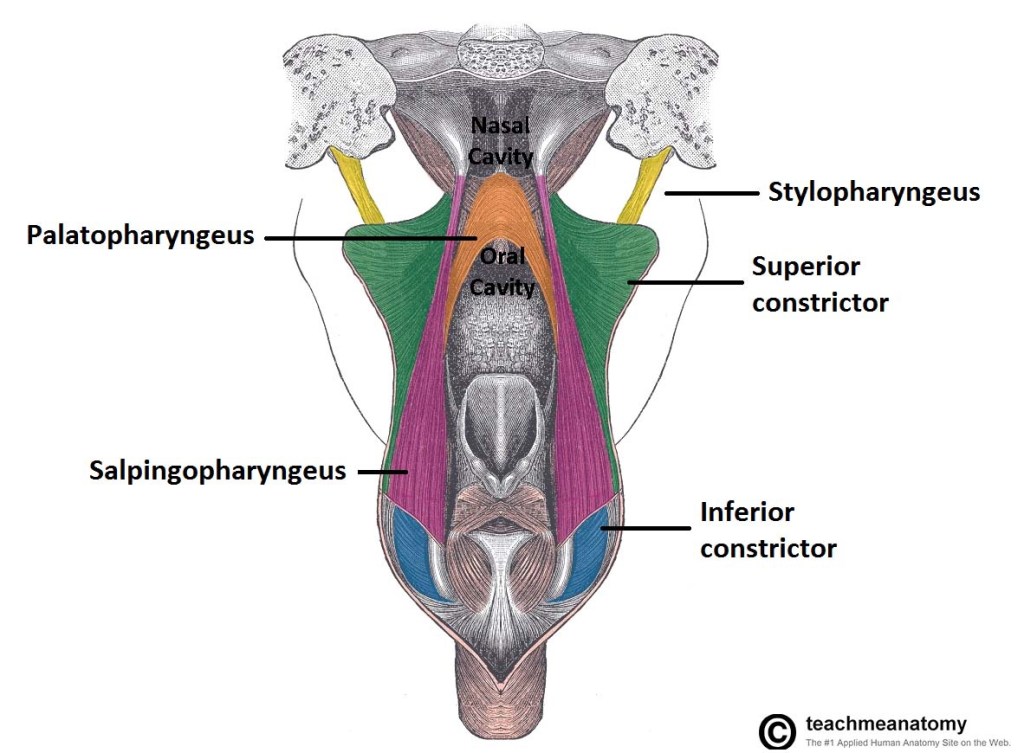
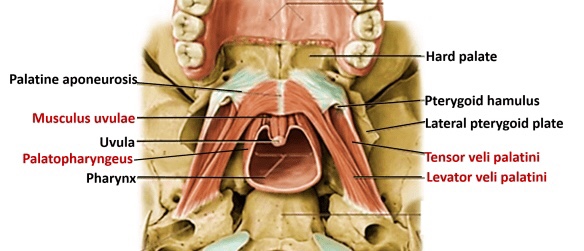
👉The muscles of the soft palate include the palatopharyngeus, palatoglossus, tensor veli palatini, levator veli palatini, and musculus uvulae.
👉Anteriorly, the soft palate is continuous with the hard palate and with the palatine aponeurosis.
👉The posterior border of the soft palate is free (i.e. not connected to any structure), and has a central process that hangs from the midline – the uvula.
👉The soft palate also forms the roof of the fauces; an area connecting the oral cavity and the pharynx.
👉Two arches bind the palate to the tongue and pharynx:
👉The palatoglossal arches anteriorly and the palatopharyngeal arches posteriorly.
👉Between these two arches lie the palatine tonsils, which reside in the tonsillar fossae of the oropharynx.
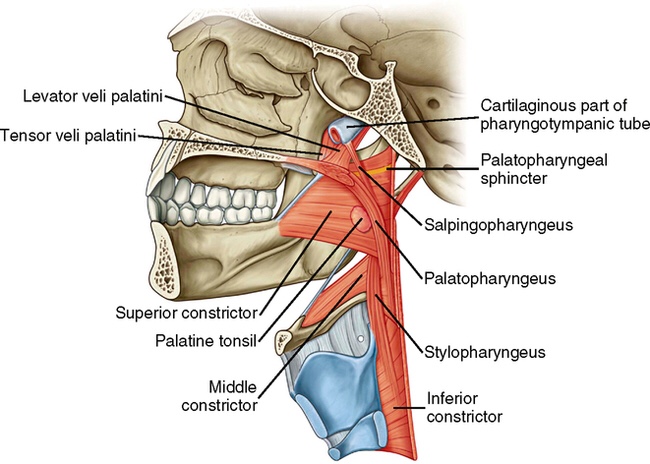
Muscles of the Soft Palate
👉There are five muscles which give the actions of the soft palate.
👉They are all innervated by the pharyngeal branch of the vagus nerve (CN X).
👉The Tensor veli palatini is the only muscle of the soft palate that is not innervated by the pharyngeal plexus derived from the vagus nerve.
👉The Tensor Veli palatini is innervated by the medial pterygoid nerve (madibular division of the trigeminal nerve / CN V).
Tensor Veli Palatini
- Attachments: Originates from the medial pterygoid plate of the sphenoid bone and inserts into the palatine aponeurosis.
- Function: Tenses the soft palate.
Levator Veli Palatini
- Attachments: Arises from the petrous portion of the temporal bone and the eustachian tube, before inserting into the palatine aponeurosis.
- Function: Elevation of the soft palate.
Palatoglossus
- Attachments: Originates from the palatine aponeurosis, and travels anteriorly, laterally and inferiorly to insert into the side of the tongue.
- Function: Pulls the soft palate towards the tongue.
Palatopharyngeus
- Attachments: Arises from the palatine aponeurosis and the hard palate, and inserts into the upper border of the thyroid cartilage.
- Function: Tenses soft palate and draws the pharynx anteriorly on swallowing.
Musculus Uvulae
- Attachments: Arises from the posterior nasal spine and the palatine aponeurosis, and inserts into the mucous membrane of the uvula.
- Function: Shortens the uvula.
Vasculature of the Soft Palate
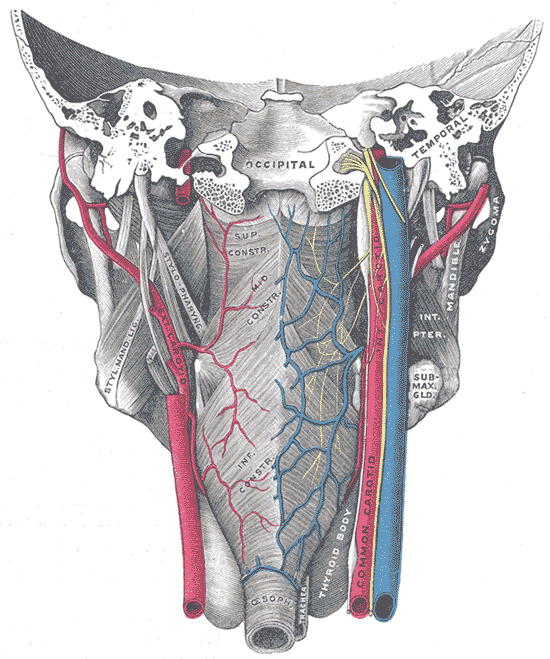
👉The palate receives its arterial supply primarily from the greater palatine arteries, which run anteriorly from the greater palatine foramen.
👉In addition, the anastomosis between the lesser palatine artery and ascending palatine artery provide collateral supply to the palate.
👉Venous drainage is into the pterygoid venous plexus.
Innervation of the Soft Palate
👉Sensory innervation of the palate is derived from the maxillary branch of the trigeminal nerve (CN V).
👉The greater palatine nerve innervates most of the glandular structures of the hard palate.
👉The nasopalatine nerve innervates the mucous membrane of the anterior hard palate and the lesser palatine nerves innervate the soft palate.
#Arrangoiz #HeadandNeckSurgeon #CancerSurgeon #SurgicalOncologist