- Resistance:
- Is the impedance of flow:
- In the tubing and airways and therefore:
- Can only occur when there is:
- Airflow
- Can only occur when there is:
- In the tubing and airways and therefore:
- According to Ohm’s Law:
- Resistance (R) = Δ pressure /Δ volume
- R = (Peak inspiratory pressure – Plateau pressure) / Tidal volume
- R = (PIP- Pplat) / (TV)
- R = (Peak inspiratory pressure – Plateau pressure) / Tidal volume
- Resistance (R) = Δ pressure /Δ volume
- Is the impedance of flow:
- Assuming a constant tidal volume:
- The resistance equation can be simplified to:
- R ≈ (PIP- Pplat)
- The resistance equation can be simplified to:
- Normal airway resistance:
- Should be ≤ 5 cmH20
- Resistance is a factor in ventilating all patients but can become particularly important:
- When ventilating patients with COPD or asthma:
- The resistance in a system:
- Increases with decreasing diameter
- While common examples include:
- A very small endotracheal tube (ETT) or bronchospasm leading to narrowing of the airways:
- Recall that a “decrease in the diameter” can also occur at just one point:
- Such as with kinking or biting of the ETT, or a mucous plug in a large airway
- Recall that a “decrease in the diameter” can also occur at just one point:
- A very small endotracheal tube (ETT) or bronchospasm leading to narrowing of the airways:
- While common examples include:
- Increases with decreasing diameter
- The resistance in a system:
- When ventilating patients with COPD or asthma:
- Compliance refers to:
- The distensibility of the system and is the inverse of elastance:
- In other words:
- It a measure of the lung’s ability to stretch and expand:
- The more elastic a system, or higher the “recoil,”:
- The lower the compliance:
- A common analogy to understand the concepts of elastance is to analyze the recoil of springs:
- Imagine a very tightly wound and stiff spring
- This spring is difficult to stretch and wants to stay in the coiled position
- This spring would have high elastance and low compliance
- Envision a second, loosely coiled spring:
- Very little force is required to stretch out this spring, and therefore, it has low elastance but high compliance
- A common analogy to understand the concepts of elastance is to analyze the recoil of springs:
- The lower the compliance:
- The more elastic a system, or higher the “recoil,”:
- It a measure of the lung’s ability to stretch and expand:
- In other words:
- The distensibility of the system and is the inverse of elastance:
- Although compliance commonly is used to describe the lung parenchyma:
- Remember that compliance actually involves all components of the system:
- In other words:
- A patient with pulmonary edema may have low compliance:
- Due to an issue with the lung parenchyma
- But another patient may have similarly low compliance due to severe chest wall stiffness after a third-degree burn
- Clinically, knowing the exact cause of decreased compliance in a given patient can be challenging:
- Physicians should not, therefore, always assume that it is always related to “stiff lungs.”
- A patient with pulmonary edema may have low compliance:
- In other words:
- Remember that compliance actually involves all components of the system:
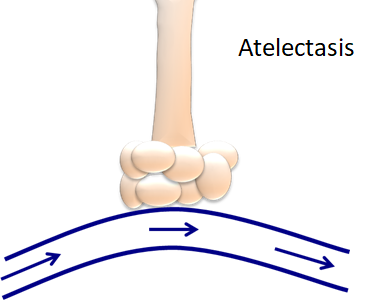
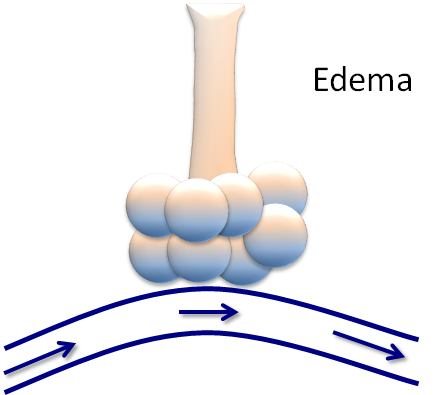
- In the figure below, the top “lungs” are healthy:
- The lungs on the left have a resistance problem or impairment in airflow
- The lungs on the right have a compliance problem or impairment in stretch and recoil
- In this picture:
- Both figures could have elevated peak inspiratory pressures (PIP):
- Due to the excess pressure generated in the system:
- However:
- Only the right-hand figure would have an elevate plateau pressure (Pplat):
- Since this process occurs when there is an absence of airflow
- Only the right-hand figure would have an elevate plateau pressure (Pplat):
- However:
- Due to the excess pressure generated in the system:
- Both figures could have elevated peak inspiratory pressures (PIP):

- Compliance (C) = ∆ volume / ∆ pressure
- C = Tidal volume / Plateau pressure – Peak inspiratory pressure
- C = (TV) / (Pplat – PEEP)
- C = Tidal volume / Plateau pressure – Peak inspiratory pressure
- Therefore, when troubleshooting high-pressures on the ventilators:
- Two values are needed:
- The peak inspiratory pressure (PIP):
- Is the maximum pressure in the system and includes both:
- Resistance and compliance:
- An inspiratory pause stops all airflow:
- Thereby removing resistance, and only leaving compliance, as illustrated in this diagram below:
- The plateau pressure, or Pplat, is, therefore:
- A measure of compliance
- The plateau pressure, or Pplat, is, therefore:
- Thereby removing resistance, and only leaving compliance, as illustrated in this diagram below:
- An inspiratory pause stops all airflow:
- Resistance and compliance:
- Is the maximum pressure in the system and includes both:
- The peak inspiratory pressure (PIP):
- Two values are needed:

- These values can be displayed on the ventilator screen:
- On most ventilators:
- The PIP is always seen
- While the Pplat is seen by pushing the “inspiratory hold” or “inspiratory pause” button on the ventilator
- An elevated PIP and normal Pplat is:
- Indicative of increased airway resistance
- An elevated PIP and elevated Pplat is:
- Indicative of abnormal compliance
- On most ventilators:

- Determining whether the patient has a:
- Resistance problem or a compliance problem:
- Can assist in the differential diagnosis of respiratory failure:
- High Resistance:
- High PIP, Low / Normal Pplat:
- Kinked / obstructed ETT
- Mucus plugging
- Brochospasm
- Endotracheal tube to narrow:
- Small
- Coughing
- Bronchospasm:
- Obstructive lung disease
- High PIP, Low / Normal Pplat:
- High Resistance:
- Can assist in the differential diagnosis of respiratory failure:
- Low Compliance:
- High PIP, High Pplat:
- Atelectasis
- Pulmonary edema
- ARDS
- Hemothorax /pneumothorax
- Pneumonia
- Pulmonary fibrosis:
- Restrictive lung disease
- Air-trapping with accumulated auto-PEEP
- Obesity
- Abdominal compartment syndrome
- Circumferential burns of the chest
- Scoliosis
- Supine position
- High PIP, High Pplat:
- Resistance problem or a compliance problem:
- Air trapping:
- Also referred to as breath-stacking:
- Can lead to the development of auto-PEEP, or intrinsic PEEP (iPEEP):
- These pressures should be differentiated from the set PEEP, or extrinsic PEEP (ePEEP):
- ePEEP refers to the additional end-expiratory positive pressure set during mechanical ventilation:
- To prevent alveolar collapse and derecruitment
- ePEEP refers to the additional end-expiratory positive pressure set during mechanical ventilation:
- These pressures should be differentiated from the set PEEP, or extrinsic PEEP (ePEEP):
- In contrast:
- Auto-PEEP, or iPEEP:
- Is a pathophysiological process:
- That can occur when the ventilator initiates the next breath prior to complete exhalation:
- While this is most common in patients with prolonged expiratory phases, such as asthma or COPD:
- It can also occur in patients:
- Who have a fast respiratory rate or
- Those who are being ventilated with large tidal volumes
- It can also occur in patients:
- The amount of auto-PEEP can be measured by:
- Pressing the “expiratory hold” or “expiratory pause” button on the ventilator:
- When this button is pressed, the ventilator will display the total PEEP:
- The auto-PEEP is the difference between the total PEEP and the set PEEP:
- Auto-PEEP (iPEEP) = Total PEEP – ePEEP
- The auto-PEEP is the difference between the total PEEP and the set PEEP:
- When this button is pressed, the ventilator will display the total PEEP:
- Pressing the “expiratory hold” or “expiratory pause” button on the ventilator:
- While this is most common in patients with prolonged expiratory phases, such as asthma or COPD:
- That can occur when the ventilator initiates the next breath prior to complete exhalation:
- Is a pathophysiological process:
- Auto-PEEP, or iPEEP:
- Can lead to the development of auto-PEEP, or intrinsic PEEP (iPEEP):
- Also referred to as breath-stacking:
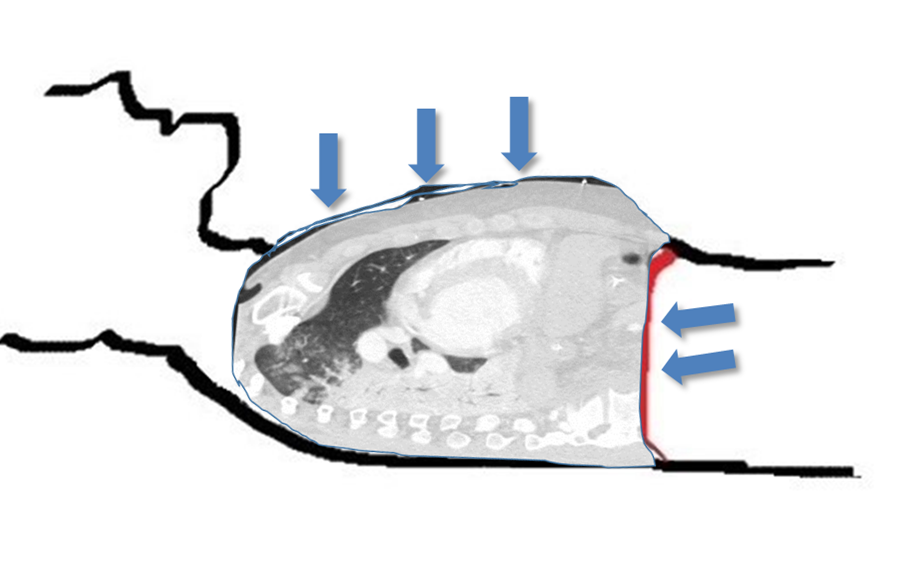
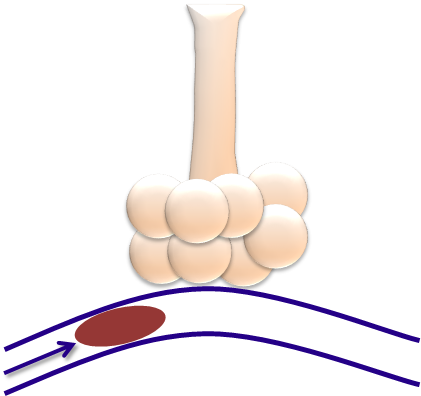
- The Figure represents the effects of air trapping:

- Air trapping, or autoPEEP:
- Can lead to significant adverse cardiopulmonary effects
- The increased intrathoracic pressure from autoPEEP can:
- Decrease venous return and lead to hemodynamic instability, even cardiac arrest in severe cases
- The increased pressures may also result in:
- A pneumothorax or pneumomediastium
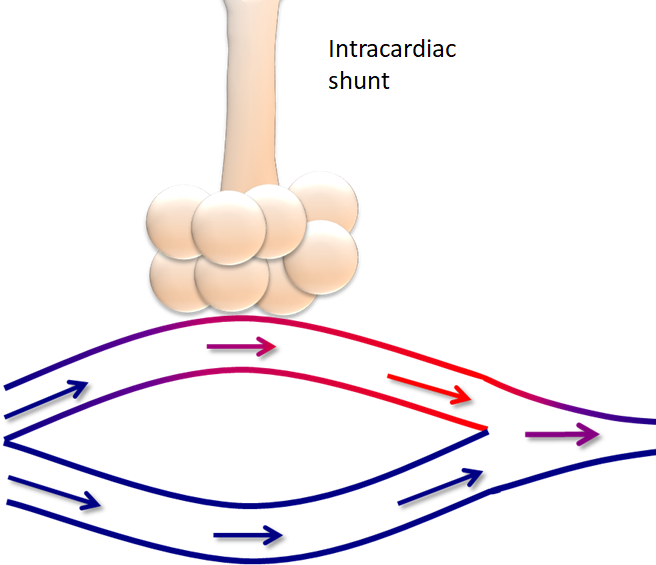
- Additionally, air trapping can lead to:
- Ineffective ventilation due to:
- Collapse of the capillaries responsible for gas exchange:
- With worsening hypercarbia and hypoxemia
- Collapse of the capillaries responsible for gas exchange:
- While this may seem like a paradox:
- As one may assume that increasing the minute ventilation, or moving more air:
- Will improve ventilation, there is a limit to the beneficial effects:
- Once the lungs are overdistended, gas exchange is ineffective
- In these circumstances, allowing the patient sufficient time to exhale can decrease CO2 retention
- Will improve ventilation, there is a limit to the beneficial effects:
- As one may assume that increasing the minute ventilation, or moving more air:
- Ineffective ventilation due to:
#Arrangoiz #Surgeon #Teacher