- Hypoxemia:
- There are four broad physiologic causes of hypoxemia:
- Shunting
- VQ mismatch
- Alveolar hypoventilation
- Decreased partial pressure of oxygen
- Understanding these mechanisms:
- Allows the clinician at the bedside to quickly develop a differential diagnosis for hypoxemia and target diagnostics to assess for the precise etiology
- Understanding these mechanisms:
- There are four broad physiologic causes of hypoxemia:
- Shunts, or blood bypassing normal gas exchange:
- Is one of the most common causes of hypoxemia
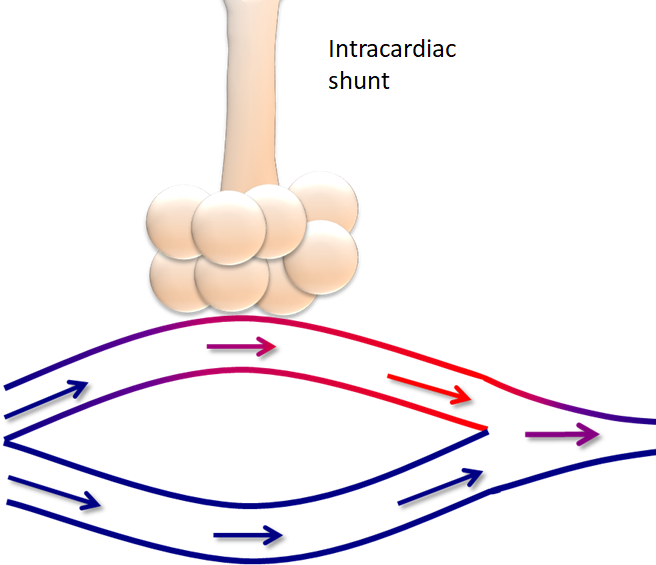
- A classic example of a shunt is an intracardiac shunt:
- In this example:
- Much of the blood passes by the alveoli, participating in normal gas exchange:
- However, a small amount is diverted through the heart, bypassing the lungs:
- This deoxygenated blood mixes with the oxygenated blood:
- Leading to hypoxemia
- This deoxygenated blood mixes with the oxygenated blood:
- However, a small amount is diverted through the heart, bypassing the lungs:
- Much of the blood passes by the alveoli, participating in normal gas exchange:
- In this example:
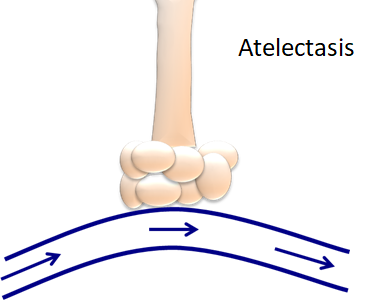
- When an area of the lung is perfused, but not ventilated:
- That results in an intra-pulmonary shunt:
- In other words:
- The inspired oxygen cannot reach the alveoli for gas exchange
- There are several different causes of intra-pulmonary shunts, including:
- Atelectasis
- Pneumonia
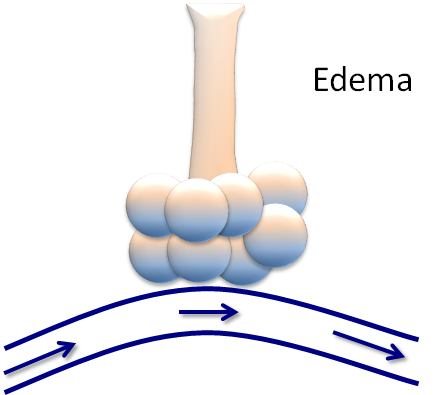
- Pulmonary edema
- Acute respiratory distress syndrome (ARDS)
- Hemothorax
- Pneumothorax
- Hyperinflation or auto-PEEPing
- All of these pathological processes:
- Prevent effective gas exchange at the alveoli
- All of these pathological processes:
- In other words:
- That results in an intra-pulmonary shunt:
- When an area has ventilation, but no perfusion:
- This is dead space:
- In other words:
- The airways are functioning normally:
- But there is a disease process in the vasculature
- The best example would be a patient in cardiac arrest who is intubated and ventilated:
- But there is an interruption of chest compressions
- The airways are functioning normally:
- Dead space can be:
- Anatomic and physiologic:
- Such as oxygenation but lack of gas exchange:
- That occurs in the upper airways, like the trachea
- Such as oxygenation but lack of gas exchange:
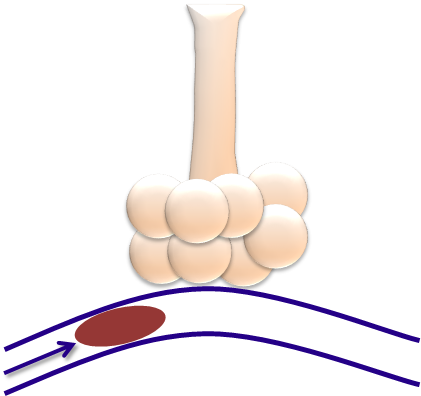
- There can also be pathological causes of dead space:
- Such as this diagram of microthrombi blocking a capillary
- Anatomic and physiologic:
- In other words:
- This is dead space:
- Other examples of dead space include:
- Low cardiac output and hyperinflation:
- As occurs in obstructive lung disease:
- In diseases such as chronic obstructive lung disease (COPD):
- There can be a significant level of hyperinflation or auto-PEEP:
- Which can lead to vasoconstriction of the capillaries involved in gas exchanged:
- Thereby leading to impaired gas exchanged
- Which can lead to vasoconstriction of the capillaries involved in gas exchanged:
- There can be a significant level of hyperinflation or auto-PEEP:
- In diseases such as chronic obstructive lung disease (COPD):
- As occurs in obstructive lung disease:
- Low cardiac output and hyperinflation:
- Dead space ventilation can lead to both:
- Hypoxia and hypercapnia:
- Due to CO2 retention
- Hypoxia and hypercapnia:
#Arrangoiz #Surgeon #Teacher
