- The exact mechanism by which breast cancer is initiated is unknown:
- However, much effort has been made to molecularly characterize breast cancer and delineate its formation and progression
- At the cell of origin level:
- The clonal evolution model:
- In which mutations accumulate
- Epigenetic changes in tumor cells occur
- The ‘fittest’ cells survive
- The cancer stem cell model:
- In which only the precursor cancer cells:
- Initiate and sustain progression
- In which only the precursor cancer cells:
- The clonal evolution model and the cancer stem cell model:
- Are both implicated, and further complicated by the fact that cancer stem cells may also evolve in a clonal fashion
- The clonal evolution model:
- At the morphological level:
- There is a continuum of lesions and genetic modifications from normal glands to cancer
- At the molecular level:
- There is evidence showing that breast cancer evolves along two divergent molecular pathways of progression:
- Mainly related to ER expression, and tumor grade and proliferation:
- Described in the intrinsic classification
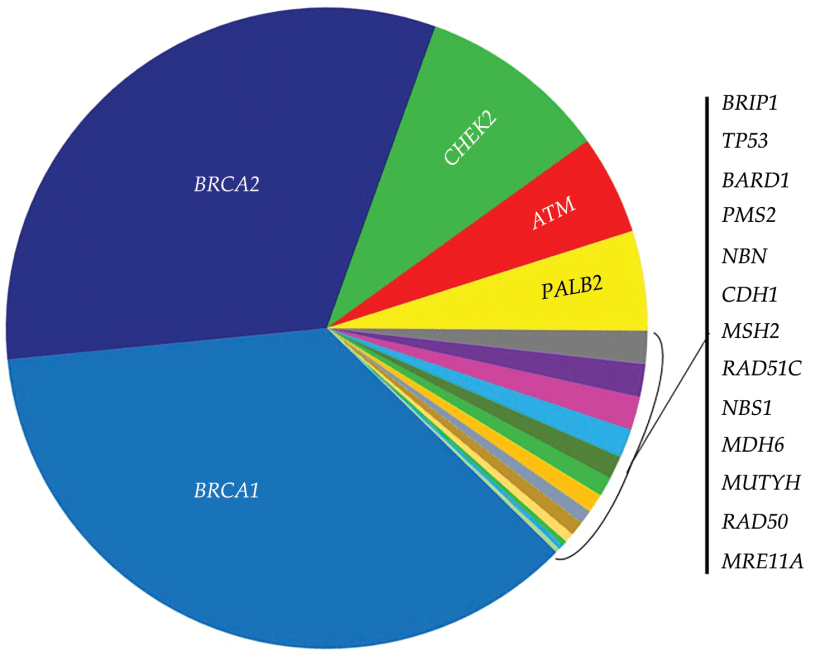
- Furthermore, the identification of breast cancer susceptibility genes:
- Has shed the light on some aspects of the pathogenesis of both sporadic and inherited breast cancer
- The first pathway:
- The low-grade-like pathway — is characterized by gain of 1q, loss 16q, infrequent amplification of 17q12 and a gene expression signature (GES) with a majority of genes associated with the ER phenotype, diploid or near diploid karyotypes and low tumour grade. The luminal A group and to some extent the luminal B group fall into this pathway. The second pathway — the high-grade-like pathway — is charac- terized by loss of 13q, gain of chromosomal region 11q13, amplification of 17q12 (containing ERBB2, encoding HER2) and an expression signature of genes involved in the cell cycle and cellular proliferation61. Tumours composed of intermediate to high grade, including HER2-positive tumours and TNBC, fall into this pathway
- Mainly related to ER expression, and tumor grade and proliferation:
- There is evidence showing that breast cancer evolves along two divergent molecular pathways of progression:
Author: Rodrigo Arrangoiz MS, MD, FACS, FSSO
My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
Fibroadenoma
- Fibroadenomas:
- Are benign tumors composed of stromal and epithelial elements
- That are commonly seen in young women
- Multiple or complex fibroadenomas:
- May indicate a slightly increased risk for breast cancer:
- The relative risk of breast cancer in patients with such fibroadenomas:
- Is approximately twice that of patients of similar age without fibroadenomas
- The relative risk of breast cancer in patients with such fibroadenomas:
- May indicate a slightly increased risk for breast cancer:
- A patient’s age determines the preferred imaging method:
- In general, ultrasonography (US) is preferred:
- If a palpable mass is found
- If a patient is younger than 30 years
- If the patient is pregnant
- Mammography and US are both useful if the patient has:
- A palpable mass
- Is older than 30 years
- Is not pregnant o In patients younger than 30 years:
- The most appropriate modality is US:
- Because the patient is spared radiation exposure and because the likelihood for fibroadenoma is not that high
- The most appropriate modality is US:
- Mammography is not indicated as the primary imaging study in women younger than 30 years:
- Unless high-risk factors are present
- Computed tomography (CT) scanning:
- Is not initially indicated for assessing a palpable lump in a woman in women younger than 30 years:
- Because of radiation exposure
- The inability of CT to demonstrate micro-calcifications
- The lack of specificity in the findings
- Is not initially indicated for assessing a palpable lump in a woman in women younger than 30 years:
- Magnetic resonance imaging (MRI):
- Is not initially indicated for assessing a palpable lump in women younger than 30 year:
- Mainly because of its high cost and the high likelihood of false-positive finding
- Is not initially indicated for assessing a palpable lump in women younger than 30 year:
- Positron emission tomography:
- Is expensive and is not universally available
- In general, ultrasonography (US) is preferred:
- On mammograms:
- Fibroadenomas typically appear as:
- Circumscribed oval or round masses:
- Which occasionally have coarse calcifications
- Circumscribed oval or round masses:
- Fibroadenomas typically appear as:
- On ultrasonograms:
- Fibroadenomas appear as circumscribed, homogeneous, oval, hypoechoic masses:
- That may have gentle lobulations
- A smooth, thin, echogenic capsule
- Variable acoustic enhancement; and homogeneity
- Fibroadenomas appear as circumscribed, homogeneous, oval, hypoechoic masses:
- On MRI:
- Fibroadenomas typically appear as smooth masses with high signal intensity on T2-weighted images and enhancement with the administration of gadolinium-based contrast agent
- Fibroadenoma:
- Is a common benign breast lesion:
- Results from the excess proliferation of connective tissue
- Fibroadenomas characteristically contain both:
- Stromal and epithelial cells
- Is a common benign breast lesion:
- Epidemiology:
- They usually occur in women:
- Between the ages of 10 and 40 years
- It is the most common breast mass:
- In the adolescent and young adult population
- Their peak incidence is between:
- 25 and 40 years
- The incidence decreases after 40 years
- Fibroadenomas commonly enlarge during pregnancy and involute at menopause: • Hence, they rarely present after the age of 40 years o The lesions are well defined and well-circumscribed clinically and the overlying skin is normal o The lesions are not fixed to the surrounding parenchyma and slip around under the palpating fingers: Hence the colloquial term a breast “mouse”. • Pathology: o A fibroadenoma is a type of adenomatous breast lesion: It contains epithelium Has minimal malignant potential o Multiple fibroadenomas occur in: 10% to 15% of patients: • Patients with multiple fibroadenomas: o Tend to have a strong family history of these tumors o They are assumed to be: Aberrations of normal breast development (ANDI) or the product of hyperplastic processes: • Rather than true neoplasms o Fibroadenomas can be stimulated by estrogen and progesterone o Some fibroadenomas also have receptors and respond to: Growth hormone and epidermal growth factor o When found in an adolescent girl: The term juvenile fibroadenoma is more appropriate • Location: o Although they can be located anywhere in the breast: There may be a predilection for the upper outer quadrant • Associations: o Cyclosporin use o Cowden syndrome • Radiographic features: o Mammography: Fibroadenomas have a spectrum of features: • Well-circumscribed discrete oval mass hypodense or isodense to the breast glandular tissue • Mass with macro-lobulation or partially obscured margin • Involuting fibroadenomas in older, typically postmenopausal patients may contain: o Calcification: Often producing the classic, coarse popcorn calcification appearance In some cases the whole lesion is calcified Calcification may also present as crushed stone-like micro-calcification which makes differentiation from malignancy difficult • Breast ultrasound: o Typically seen as a well-circumscribed, round to ovoid, or macro-lobulated mass with generally uniform hypoechogenicity o Intralesional sonographically detectable calcification: May be seen in approximately 10% of cases o Sometimes a thin echogenic rim (pseudo capsule) may be seen sonographically • Breast MRI: o T1: typically hypo intense or isointense compared with adjacent breast tissue o T2: can be hypo- or hyper intense o T1 C+ (Gd): can be variable but a majority will show slow initial contrast enhancement followed by a persistent delayed phase (type I enhancement curve); non-enhancing internal septations may be seen • Diagnosis: o These lesions are easily biopsied under ultrasound guidance o When a lesion has the typical features of a fibroadenoma on ultrasound and there are no clinical red flags: They can be safely followed clinically o When lesions enlarge or have atypical imaging findings: Ultrasound-guided core biopsy is a minimally invasive outpatient procedure that will give a diagnosis with virtually no complications o There may be a maximum diameter above which a biopsy should be done if no previous imaging is available: The reason for intervention based on size is that a phyllodes tumor may be indistinguishable from a fibroadenoma on ultrasound: • A maximum diameter of 2.5 cm may be a useful benchmark for biopsy if you have no previous imaging o Interval enlargement is an indication for biopsy • Treatment and prognosis: o They are benign lesions with minimal or no malignant potential o The risk of malignant transformation is extremely low: Has been reported to range around 0.0125% to 0.3%. o Indications for biopsy include: Enlarging lesion Atypical findings on ultrasound A lesion above 2.5 cm and there are no previous studies for comparison Patient peace of mind: • Some patients are simply not happy with a palpable mass in the breast without a histological diagnosis: o This is a valid and reasonable indication for biopsy
- They usually occur in women:
Antibiotics prophylaxis (thyroid surgery) (AAES guidelines 2020)
👉Surgical site infection is a rare complication after routine transcervical thyroidectomy, with a reported incidence of 0.09% to 2%.
👉In a small European study, preoperative antibiotic administration did not affect the incidence of surgical site infection.
👉Antimicrobial prophylaxis (AMP) for clean surgery of the head and neck was not recommended in a 1999 pharmacy guideline, with moderate strength of evidence.
👉A recent single-institution randomized trial confirmed the safety of clean thyroid and parathyroid surgery without AMP.
👉However, routine AMP is still commonly used for clean thyroid and parathyroid surgeries in Japan and many other countries; according to an international survey of 275 endocrine surgeons, 26% administered AMP “almost always”, particularly in Asia (59%).
👉Because both preoperative (obesity, alcohol use) and intraoperative factors (ie, operative time, airway injury) are associated with infection, high-risk patients may benefit from selective use of AMP, in which case gram-positive coverage should be administered before or on induction.
👉With rare exceptions, postoperative AMP is not indicated.
👉Recommendation 19 AAES: Antimicrobial prophylaxis is not necessary in most cases of standard transcervical thyroid surgery. (Strong recommendation, high-quality evidence)
#Arrangoiz #ThyroidSurgeon #ParathyroidSurgeon #HeadandaneckSurgeon #EndocrineSurgery #CASO #CenterforAdvancedSurgicalOncology #PalmettoGemeralHospital
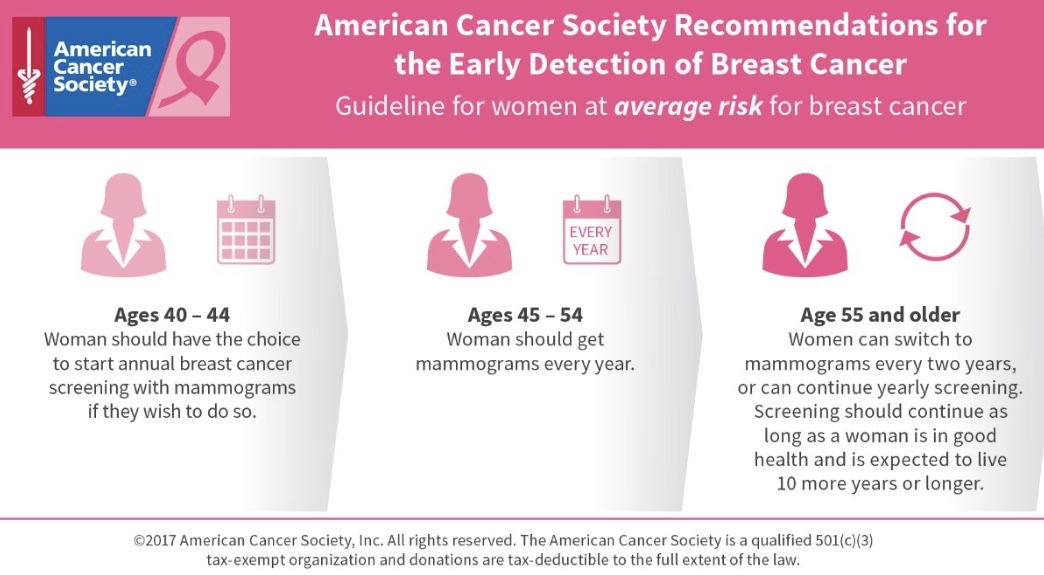
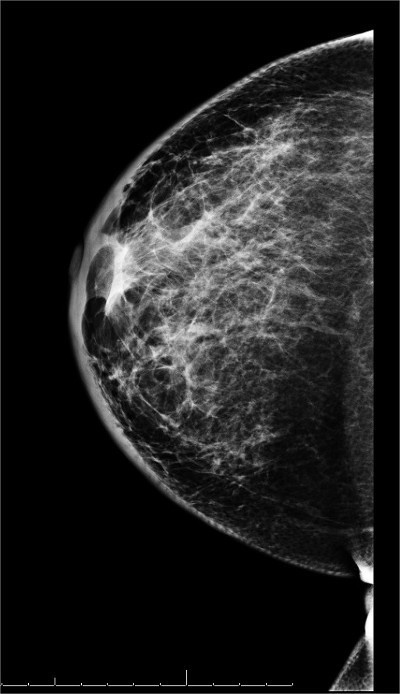
Why Undergo Screening Mammography?
👉The Swedish Two-County Trial was the first breast screening trial to demonstrate a reduction in breast cancer mortality from screening mammography alone, showing a 30% reduction in mortality among women aged 40 to 74 years invited to screening.
👉Three decades of follow-up on this study have shown a stable effect upon mortality reduction and an increased absolute benefit in terms of lives saved.
👉Mammographic screening has been shown to be associated with a reduction in breast cancer mortality across a range of study designs, including randomized controlled trials and observational studies.
👉Although specific estimates vary, a meta-analysis of eight randomized trials demonstrated a 14% to 32% mortality reduction among women invited to screening compared with women who were not invited.
👉A recent Norwegian prospective cohort study found invitation to modern mammography screening resulted in a 28% decrease in mortality.
👉An Australian case-control study and meta-analysis of women participating in organized clinical screening programs showed a 49% mortality reduction.
👉The Swedish Organised Service Screening Evaluation Group, in an incidence-based mortality study, demonstrated a mortality reduction of 40% to 45% in women screened.

👉REFERENCES
- Helvie MA, Chang JT, Hendrick RE, Banerjee M. Reduction in late-stage breast cancer incidence in the mammography era: implications for overdiagnosis of invasive cancer. Cancer. 2014;120:2649-2656.
- Nelson HD, Tyne K, Naik A, Bougatsos C, Chan BK, Humphrey L; U.S. Preventive Services Task Force. Screening for breast cancer: an update for the U.S. Preventive Services Task Force. Ann Intern Med. 2009;151:727-737.
- Nickson C, Mason KE, English DR, Kavanagh AM. Mammographic screening and breast cancer mortality: a case-control study and meta-analysis. Cancer Epidemiol Biomarkers Prev. 2012;21:1479-1488.
- Oeffinger KC, Fontham ET, Etzioni R, et al; American Cancer Society. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015;20;314:1599-1614.
- Swedish Organised Service Screening Evaluation Group. Reduction in breast cancer mortality from organized service screening with mammography: 1. Further confirmation with extended data. Cancer Epidemiol Biomarkers Prev. 2006;15:45-51.
- Tabár L, Fagerberg CJ, Gad A, et al. Reduction in mortality from breast cancer after mass screening with mammography. Randomised trial from the Breast Cancer Screening Working Group of the Swedish National Board of Health and Welfare. Lancet. 1985;13:829-832.
- Tabár L, Vitak B, Chen TH, et al. Swedish two-county trial: impact of mammographic screening on breast cancer mortality during 3 decades. Radiology. 2011;260:658-663.
- Weedon-Fekjær H, Romundstad PR, Vatten LJ. Modern mammography screening and breast cancer mortality: population study. BMJ. 2014;348:g3701.
#Arrangoiz
#BreastSurgeon
#CancerSurgeon
Nipple Discharge
- Definition of nipple discharge:
- Fluid that leaks from one or both nipples is called a nipple discharge:
- Each breast has several (15 to 20) milk ducts:
- A discharge can come from one or more of these ducts
- Each breast has several (15 to 20) milk ducts:
- Fluid that leaks from one or both nipples is called a nipple discharge:
- Nipple discharge accounts for approximately 2% to 10% of the symptoms that women report when they seek care at breast clinics:
- Causing anxiety in patients because it can be a presenting sign of breast cancer:
- However, it is usually benign in origin (papillomas and galactophore / mammary duct ectasia):
- With a 5% to 21.3% risk of an underlying malignant lesion:
- Mostly due to in situ carcinomas
- With a 5% to 21.3% risk of an underlying malignant lesion:
- However, it is usually benign in origin (papillomas and galactophore / mammary duct ectasia):
- Causing anxiety in patients because it can be a presenting sign of breast cancer:
- Nipple discharge can occur normally during the last weeks of pregnancy and after childbirth:
- When breast milk is produced
- A nipple discharge can also be normal in women who are not pregnant or breastfeeding:
- Especially during the reproductive years:
- For example, in women, fondling, suckling, irritation from clothing, or sexual arousal can stimulate a nipple discharge, as can stress:
- However, a nipple discharge in men is always abnormal
- For example, in women, fondling, suckling, irritation from clothing, or sexual arousal can stimulate a nipple discharge, as can stress:
- Especially during the reproductive years:
- A normal nipple discharge is usually:
- A thin, cloudy, whitish, or almost clear fluid that is not sticky:
- However, the discharge may be other colors, such as gray, green, yellow, or brown
- During pregnancy or breastfeeding:
- A normal discharge is sometimes slightly bloody
- A thin, cloudy, whitish, or almost clear fluid that is not sticky:
- If the discharge is considered to be physiologic on the basis of clinical information and characteristics of the nipple discharge:
- No further imaging studies of the breast are warranted:
- Although approximately 80% to 90% of patients with pathologic nipple discharge have been reported to have benign conditions:
- Breast imaging enables the localization of the breast abnormalities causing the pathologic nipple discharge:
- Which helps minimize the number of operations and / or the extent of surgery
- In addition, localizing the origin of pathologic nipple discharge enables percutaneous biopsy under imaging guidance:
- Which allows clinicians to be more confident when deciding upon management and when choosing whether to perform minimally invasive percutaneous vacuum-assisted excision
- Breast imaging enables the localization of the breast abnormalities causing the pathologic nipple discharge:
- Abnormal discharges vary in appearance depending on the cause:
- An abnormal discharge may be accompanied by other abnormalities:
- Such as dimpled skin, swelling, redness, crusting, sores, and a retracted nipple:
- A nipple is retracted if it pulls inward and does not return to its normal position when it is stimulated
- Such as dimpled skin, swelling, redness, crusting, sores, and a retracted nipple:
- If a discharge from only one breast occurs on its own (without any stimulation of the nipple):
- It is considered abnormal
- An abnormal discharge may be accompanied by other abnormalities:
- Causes:
- Several disorders can cause an abnormal discharge:
- A discharge from one milk duct or from one breast:
- Is likely to be caused by a problem with that breast:
- Such as a noncancerous (benign) or cancerous breast tumor
- Is likely to be caused by a problem with that breast:
- A discharge from both breasts or from several milk ducts in one breast is more likely to be caused by a problem outside the breast:
- Such as a hormonal disorder or use of certain drugs
- A discharge from one milk duct or from one breast:
- Several disorders can cause an abnormal discharge:
- Common causes of a nipple discharge:
- Usually, the cause is a benign disorder of the milk ducts, such as the following:
- A benign tumor in a milk duct (intra ductal papilloma):
- Intra ductal papilloma is the most common cause
- It is also the most common cause of a bloody nipple discharge when there is no lump in the breast
- Dilated milk ducts (mammary duct ectasia)
- Fibrocystic changes:
- Including pain, cysts, and general lumpiness
- A breast infection or abscess
- Less common causes of a nipple discharge:
- Certain disorders stimulate the production of breast milk in women who are not pregnant or breastfeeding:
- In most of these disorders, the level of prolactin (a hormone that stimulates production of breast milk) is elevated:
- Taking certain drugs can have the same effect
- In most of these disorders, the level of prolactin (a hormone that stimulates production of breast milk) is elevated:
- Cancer causes fewer than 10% of cases:
- Nipple discharge is a cause for concern when it:
- Occurs without the nipple’s being squeezed or stimulated by other means (when it occurs spontaneously)
- Occurs in women aged 40 or older
- Comes from only one breast
- Is bloody or pink
- Is accompanied by a lump that can be felt
- Occurs in a boy or man
- Nipple discharge is a cause for concern when it:
- Certain disorders stimulate the production of breast milk in women who are not pregnant or breastfeeding:
- A benign tumor in a milk duct (intra ductal papilloma):
- Usually, the cause is a benign disorder of the milk ducts, such as the following:
- Preferred examination:
- Mammography or digital breast tomosynthesis (DBT):
- Is the first-line study for a pathologic discharge in most patients:
- Mammography is limited:
- Because of its poor sensitivity of 20% to 25%
- A negative mammogram in the context of nipple discharge:
- Does not therefore exclude any underlying disease:
- Mammography is limited:
- Is the first-line study for a pathologic discharge in most patients:
- Ultrasound is performed immediately after mammography even if the mammogram is normal
- Mammography or digital breast tomosynthesis (DBT):
- According to the American College of Radiology (ACR) Appropriateness Criteria:
- For women 30 to 39 years of age:
- Either mammography or ultrasonography may be used as the initial examination
- For women aged 30 years or younger:
- Ultrasound should be the initial examination:
- With mammography / DBT added when ultrasound shows suspicious findings or if the patient is predisposed to developing breast cancer
- Ultrasound should be the initial examination:
- For men aged 25 years or older:
- Mammography / DBT should be, performed initially:
- With ultrasound added as indicated, given the high incidence of breast cancer in men with pathologic nipple discharge
- Mammography / DBT should be, performed initially:
- Although MRI and ductography (galactography) are not usually appropriate as initial examinations:
- Each may be useful when the initial standard imaging evaluation is negative
- For women 30 to 39 years of age:

#Arrangoiz #CancerSurgeon #BreastSurgeon #BreastCancer #SurgicalOncologist #CASO #CenterforAdvancedSurgicalOncology #PalmettoGeneralHospital
Criteria for Observing Breast Fibroadenomas
- Criteria which allow safe observation of the suspected fibroadenoma:
- Age less than 35 years
- Physical examination demonstrating a mobile and well-circumscribed mass
- Size: 2.5 cm
- And if present:
- A biopsy definitive for fibroadenoma

#Arrangoiz #CancerSurgeon #BreastSurgeon #SurgicalOncologist #CASO #CenterforAdvancedSurgicalOncology #PalmettoGeneralHospital
Objective Responses Observed in Rare Thyroid Tumors With Dual Checkpoint Blockade
Dual anti-CTLA-4 and anti-PD-1 blockade with the combination of ipilimumab (Yervoy) with nivolumab (Opdivo) induced an objective response rate (ORR) of 12% as treatment of patients with thyroid cancer, according to findings for the thyroid cancer cohort in the phase 2 SWOG S1609 Dual Anti-CTLA-4 and Anti-PD-1 blockade in Rare Tumors (DART) clinical trial (NCT02834013).1
These 2 agents have proven effective in many different tumor histologies, including subpopulations of melanoma and lung cancer, but their efficacy as treatment of rare tumors has not been determined. The study, which was presented in a poster during the 2020 Society for Immunotherapy of Cancer (SITC) Annual Meeting, is a prospective, open-label, multicenter trial aimed to explore the efficacy of this combination in rare cancers.
Ipilimumab was administered intravenously (IV) at 1 mg/kg every 6 weeks plus nivolumab 240 mg IV every 2 weeks. The thyroid cancer cohort included 17 patients who were eligible and received therapy out of 21 patients who registered to this cohort. The primary end point of the study is ORR, and secondary end points include progression-free survival (PFS), overall survival (OS), stabled disease (SD) >6 months, and toxicity.
The median age of patients in the thyroid cohort was 59 years (range, 33-78), and 10 (59%) patients were male. The most common thyroid cancer subtype was papillary in 47% of patients, while other subtypes in the cohort included medullary thyroid cancer (MTC; 24%), anaplastic thyroid cancer (ATC; 24%), and Hurthle cell histology (6%).
In terms of ORR, 2 patients had a confirmed partial response (12%), which included 1 patient with PTC and 1 with ATC. One of the 4 patients with ATC had a response that lasted more than 2 years (25%). SD lasted for more than 6 months in 6 patients (35%), while 2 (12%) had SD for less than 6 months. The clinical benefit rate, which included all PRs and SD over 6 months, was 59%.
One patient with PTC who withdrew early due to toxicities, including neuropathic pain and arthralgias, had SD for more than 1 year but was not included in the response assessment.
The median PFS was 9.5 months (95% CI, 4.99-∞), and the median OS was not reached. The 6-month PFS rate was 58% (95% CI, 39-88), and the 6-month OS rate was 88% (95% CI< 74%-100%).
Overall, 94.1% of patients experienced adverse events (AEs), and 52.9% had grade 3-5 AEs. The most common AEs of any grade included fatigue in 41.2%, elevated lipase (29.4%), and acute kidney injury, diarrhea, generalized muscle weakness, anorexia, pruritis, nausea and alanine aminotransferase elevation in 21.1% each.
The most common immune-mediated AES included acute kidney injury and elevated lipase, which occurred in 29.4% of patients each. While enrolled in the study, 1 patient died.
Immunotherapy and monoclonal antibodies, such as nivolumab and ipilimumab, are suspected to assist the body’s immune system in order to attack the cancer, and these therapies may also interfere with the ability of tumor cells to grow and spread.
This combination has demonstrated its benefit with FDA approval as treatment of patients with metastatic or recurrent non–small cell lung cancer whose tumors express PD-L1 ≥1% and who do not harbor an EGFR or ALK tumor aberration. This approval was granted in May 2020 based on positive findings from the phase 3 CheckMate 227 study, which demonstrated a significant improvement in OS over chemotherapy alone.2
More recently in October 2020, the FDA also granted approval to this combination for the frontline treatment of adult patients with unresectable malignant pleural mesothelioma, which marked the first and only immunotherapy regimen indicated for the treatment of untreated, unresectable disease.3
References
1. Chae YK, Othus M, Patel SP, et al. A phase ii basket trial of dual anti-cdla-4 and anti-pd-1 blockade in rare tumors (DART) SWOG 1609: the thyroid tumor cohort. Poster presented at: SITC Annual Meeting. November 11-14, 2020; Virtual.
2. FDA approves nivolumab plus ipilimumab for first-line mNSCLC (PD-L1 tumor expression ≥1%) BMS [news release]. FDA. May 15, 2020. Accessed November 12, 2020. https://bit.ly/3cwvlo2
3. U.S. Food and Drug Administration Approves Opdivo® (nivolumab) + Yervoy® (ipilimumab) as the First and Only Immunotherapy Treatment for Previously Untreated Unresectable Malignant Pleural Mesothelioma. News release. Bristol Myers Squibb. October 2, 2020. Accessed November 12, 2020. https://bwnews.pr/
#Arrangoiz #ThyroidSurgeon #ThyroidExpert #ThyroidCancer #HeadandNeckSurgeon #CASO #CenterforAdvancedSurgicalOncology #PalmettoGeneralHospital

Time Intervals for Imaging Evaluation of Patients Following Breast-Conservation Surgery
- Previously, there was no consensus on the optimal time intervals for imaging evaluation of patients following breast-conservation surgery:
- Many practices performed 6-month interval mammography of the treated breast for a variable number of years in an effort to monitor post-procedure changes
- The usefulness of short-term follow-up mammography in women undergoing breast conservation has been challenged:
- Local recurrence in the ipsilateral breast following breast conservation and radiotherapy occurs at:
- An estimated rate of:
- 1% in the first year
- 3% to 9% at 5 years
- 14% to 20% at 20 years
- An estimated rate of:
- Retrospective studies have verified that the yield from a 6-month follow-up mammogram on the affected side is:
- Low (≤ 1%)
- Local recurrence in the ipsilateral breast following breast conservation and radiotherapy occurs at:
- Therefore, the ACR and ASCO recommendations are:
- To perform a bilateral mammogram at 12 months from the initial mammogram:
- Which should be at least 6 months following completion of radiotherapy:
- And should include a diagnostic mammogram on the affected side and a screening mammogram on the nontreated side
- Which should be at least 6 months following completion of radiotherapy:
- Bilateral annual mammography is recommended thereafter
- To perform a bilateral mammogram at 12 months from the initial mammogram:
- Elimination of the 6-month and 18-month interval diagnostic mammograms after breast conservation:
- Should spare women unnecessary anxiety, discomfort, and inconvenience while lowering costs and improving efficiency

- References:
- https://www.asco.org/research-guidelines/quality-guidelines/guidelines/breast-cancer#/9821 Accessed July 20, 2020
- Monticciolo DL, Newell MS, Moy L, Niell B, Monsees B, Sickles EA. Breast cancer screening in women at higher-than-average risk: recommendations from the ACR. J Am Coll Radiol. 2018;15(3 Pt A):408-414.
- Khatcheressian JL, Hurley P, Bantug E, Esserman LJ, Grunfeld E, Halberg F, et al. Breast cancer follow-up and management after primary treatment: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2013;31(7):961-965.
#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOncologist #BreastCancer #intervalBreastImaging #CASO #CenterforAdvancedSurgicalOncology #PalmettoGeneralHospital
Accelerated Partial Breast Irradiation
- Accelerated partial breast irradiation includes multiple techniques such as:
- Interstitial brachytherapy
- Applicator brachytherapy
- External beam radiation therapy
- The Groupe Européen de Curie thérapie of European Society for Radiotherapy and Oncology (GEC-ESTRO) trial:
- Randomized 1184 patients with:
- Low-risk invasive carcinoma or ductal carcinoma in situ (DCIS) treated with breast-conserving surgery to either whole-breast irradiation (WBI) or APBI using multi catheter brachytherapy:
- The cumulative incidence of local recurrence at 5 years was:
- 1.44% with APBI
- 0.92% with WBI
- The cumulative incidence of local recurrence at 5 years was:
- Low-risk invasive carcinoma or ductal carcinoma in situ (DCIS) treated with breast-conserving surgery to either whole-breast irradiation (WBI) or APBI using multi catheter brachytherapy:
- Randomized 1184 patients with:
- The Florence trial:
- Randomized 520 patients to either WBI or APBI with intensity-modulated radiation therapy:
- With a mean follow-up of 5 years:
- The rate of local recurrence was:
- 1.5% in both arms
- The rate of local recurrence was:
- With a mean follow-up of 5 years:
- Randomized 520 patients to either WBI or APBI with intensity-modulated radiation therapy:
- The American Society of Breast Surgeons’ Mammo Site Registry found:
- 5-year rates of local recurrence were less than 4%
- An older randomized trial from Hungary using interstitial APBI and electrons:
- 5-year local recurrence rate of 4.7%
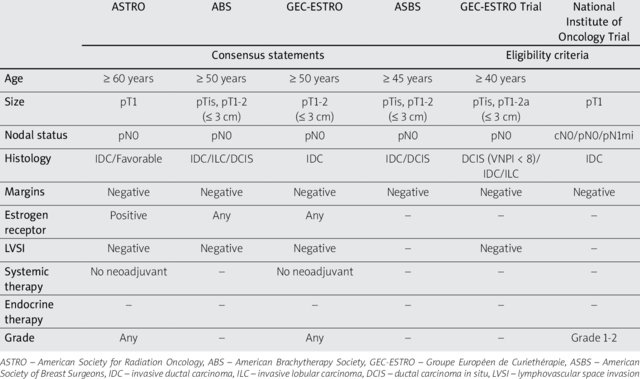
- It is important to recognize that these outcomes are likely due to:
- The highly selected, low-risk patient populations included in many of the APBI trials as evidenced by the tables / guidelines:
- Patients tend to be:
- Postmenopausal
- Tumors less than 3 cm, without DCIS
- Node negative
- ER-positive
- Patients tend to be:
- The highly selected, low-risk patient populations included in many of the APBI trials as evidenced by the tables / guidelines:
#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOncologist #BreastCancer #CASO #CenterforAdvancedSurgicalOncology #PalmettoGeneralHospital

TP53 Gene Mutation and Breast Cancer Risk
- The TP53 gene:
- Is a key tumor-suppressor gene:
- That acts as a checkpoint control for DNA damage
- Due to its critical role in controlling cellular damage:
- A TP53 germline mutation predisposes patients to multiple malignancies, including:
- Breast cancer and soft tissue sarcomas
- A TP53 germline mutation predisposes patients to multiple malignancies, including:
- Is a key tumor-suppressor gene:
- The associated familial syndrome was first observed in 1969 and is known as the Li-Fraumeni syndrome:
- The penetrance of breast cancer related to TP53 mutations is higher than seen in the more common BRCA 1 or BRCA 2 mutations:
- With a cumulative incidence reported for TP53 of:
- 85% by age 60.
- TP53-associated breast cancers:
- Present at an early age:
- Median age of diagnosis is 34
- The majority are:
- Hormone receptor positive and / or HER-2 positive
- Present at an early age:
- Due to this high penetrance and associated increased risk for a secondary breast cancer:
- Bilateral prophylactic mastectomy is recommended:
- For management of an early-stage breast cancer in patients with a mutation in TP53
- This is especially true in younger women:
- As contralateral breast cancer risk inversely correlates with the patient’s age
- The recommendation for mastectomy is further supported by the concern regarding radiation use in this patient population already at increased risk for soft tissue sarcomas:
- Radiation should be used with extreme caution and careful consideration of the risk / benefit
- Bilateral prophylactic mastectomy is recommended:
- With a cumulative incidence reported for TP53 of:
- For patients presenting with a known TP53 germline mutation and without a diagnosis of breast cancer:
- NCCN guidelines recommend:
- Annual breast MRI at 20 to 29 years
- Annual MRI and mammography at 30 to 75 years for high-risk breast cancer screening
- Consideration of prophylactic risk-reducing mastectomy should be made in context of the age of presentation:
- As breast cancer risk increases significantly after the second decade of lifein these patients:
- Bilateral mastectomy should be considered:
- Starting at age 20
- Bilateral mastectomy should be considered:
- The risk of breast cancer peaks at age 40 to 45 and then decreases:
- Therefore bilateral mastectomy offers significantly less benefit in women over 60 years of age
- As breast cancer risk increases significantly after the second decade of lifein these patients:
- NCCN guidelines recommend:
- The penetrance of breast cancer related to TP53 mutations is higher than seen in the more common BRCA 1 or BRCA 2 mutations:
- References:
- Mai PL, Best AF, Peters JA, DeCastro RM, Khincha PP, Loud JT, Bremer RC, Rosenberg PS, Savage SA Risks of first and subsequent cancers among TP53 mutation carriers in the National Cancer Institute Li-Fraumeni syndrome cohort. Cancer. 2016 Dec 1; 122(23):3673-3681.
- Masciari S, Dillon DA et al. Breast cancer phenotype in women with TP53 germline mutations: a Li Fraumeni syndrome consortium effort. Breast Cancer Res Treat. 2012;133(3):1125–1130.
- Schon, K, Tischkowitz, M. Clinical implications of germline mutations in breast cancer: TP53 Breast Cancer Res Treat. 2018; 167(2): 417–423.
- National Comprehensive Cancer Network (2014) Genetic/familial high risk assessment: breast and ovarian. Li Fraumeni syndrome management. NCCN Clinical Practice Guidelines in Oncology. Version 1.2018.
#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOncologist #BreastCancer #CASO #CenterforAdvancedSurgicalOncology #PalmettoGeneralHospital
