My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
Skeletal manifestations including osteopenia, osteoporosis, and osteitis fibrosa cystica:
Are found in approximately 15% of patients with PHPT
PHPT is linked with a reduction in bone mineral density (BMD):
Particularly in the cortical bone:
Such as in the distal third of the radius
In the lumbar region, composed all most exclusively by trabecular bone, and in the femoral region, composed by cortical and trabecular bone:
The decrease in BMD is less severe
Osteitis fibrosa cystica:
A skeletal manifestation that is rarely seen today:
Seen in less than five percent of patients with PHPT
Is caused by an increase in bone turnover:
Can be determined by finding an:
Elevated serum alkaline phosphatase level
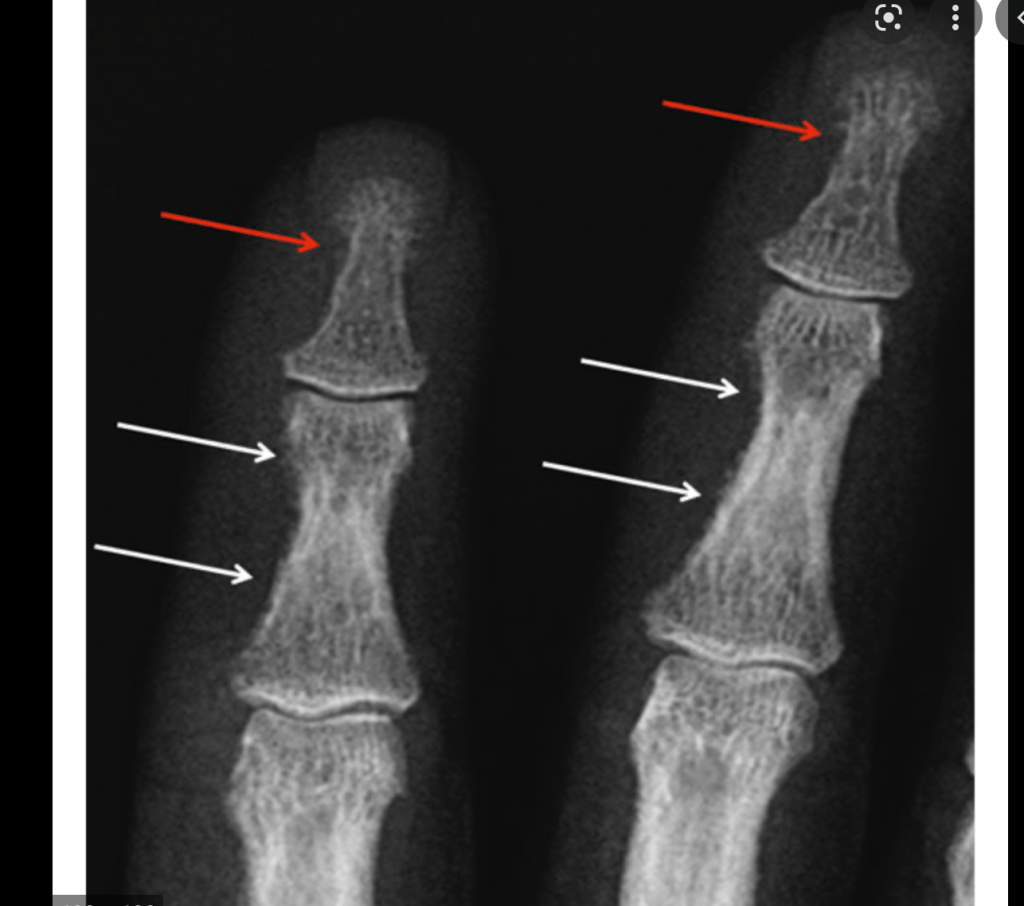
The radiologic findings seen in patients with PHPT with bone disease are characterized by:
Subperiosteal resorption:
Most obvious on the radial aspect of the middle phalanx of the second and third fingers
Bone cysts
Tufting of the distal phalanges:
Which are best evaluated on plain x-rays of the hands
Brown or osteoclastic tumors:
Caused by the accumulations of osteoclasts and fibrous tissue:
Brown tumors have a slightly greater incidence in PHPT than in secondary HPT:
3% versus 2%
In patients with chronic kidney disease:
Persistent and excessive urinary calcium elimination:
Can lower serum calcium level:
And lead to an increase in PTH secretion
This results in mobilization of calcium from the bones:
Through rapid osteoclastic turnover of bone to maintain normal serum calcium levels
In regions where bone loss is exceptionally fast:
Hemorrhage, and reparative granulation tissue, with active, vascular, proliferating fibrous tissue may replace the normal marrow contents:
Resulting in a brown tumor
Hemosiderin imparts the brown color (hence the name of the lesions
The skull also may be affected:
Appears mottled with a loss of definition of the inner and outer cortices
Patients with normal serum alkaline phosphatase levels:
Almost never have clinically apparent osteitis fibrosa cystica
Bone disease correlates with serum PTH and vitamin D levels
Generalized osteopenia, erosion of the terminal phalangeal tufts and subperiosteal resorption of bone particularly the radial aspects of the 2nd and 3rd middle phalanges.Brown TumorsSalt and Pepper Skull
Clinical and pathologic staging of patients with cancer is valuable for many reasons, including the following:
To estimate risk of recurrence and disease-specific mortality for an individual patient
To tailor decisions regarding postoperative adjunctive therapy (such as the need for radioiodine [RAI] ablation and degree of thyroid-stimulating hormone [TSH] suppression):
To the patient’s risk for disease recurrence and mortality
To make decisions regarding the frequency, modality, and intensity of follow-up based upon an individual patient’s risk of recurrence and mortality
To enable accurate communication regarding a patient among health care professionals
To allow evaluation of differing therapeutic strategies applied to comparable groups of patients in clinical studies
To provide “a method of conveying clinical experience to others without ambiguity
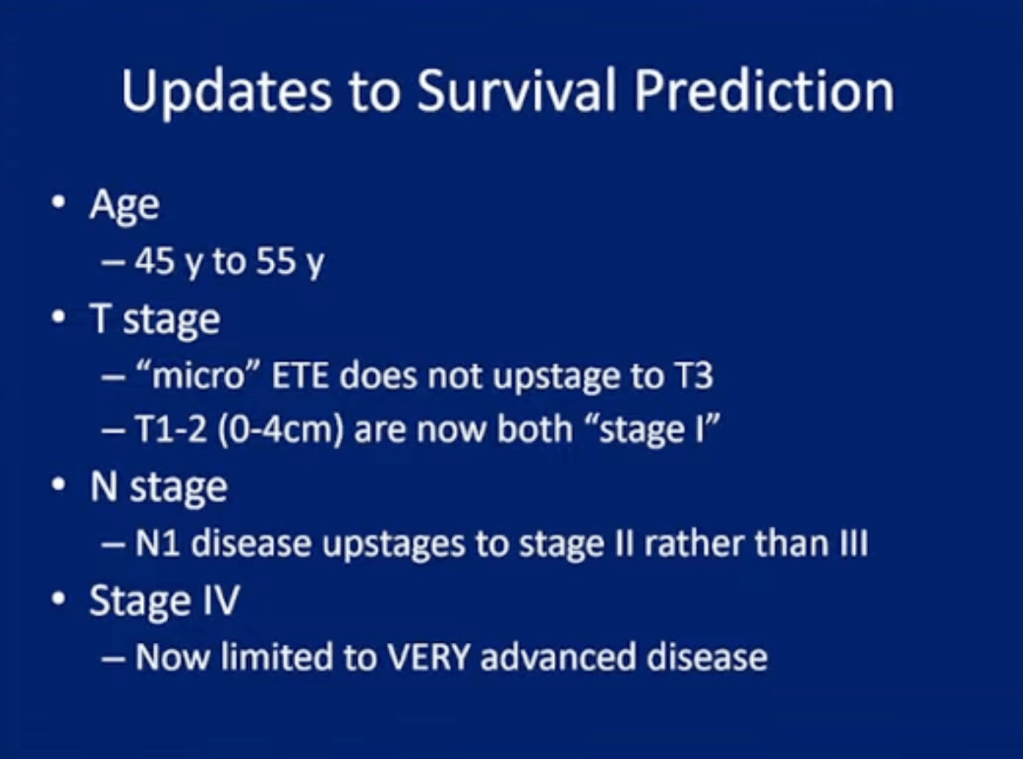
Initial postoperative staging:
You can use the several staging systems to estimate disease-specific mortality:
Elderly patients with pHPT are at increased risk of bone-related disease and fractures and are more likely to have neuropsychiatric complaints; however, referral for parathyroidectomy in the elderly is often limited due to the perceived risk of surgery.
Parathyroidectomy is the only curative treatment.
This study found that parathyroidectomy in the elderly was not associated with higher morbidity.
Elderly patients with hypercalcemia should be evaluated for pHPT and if confirmed should be considered for parathyroidectomy.
Am J Surg. 2021 Sep;222(3):549-553. doi: 10.1016/j.amjsurg.2021.01.027.
• Fibroadenomas typically appear as smooth masses:
• With high signal intensity on T2-weighted images
• Enhancement with the administration of gadolinium-based contrast
• T1:
• Typically hypointense or isointense compared with adjacent breast tissue
• T2:
• Can be hypointense or hyperintense compared with adjacent breast tissue
• T1 C+ (Gd):
• Can be variable:
• But a majority will show slow initial contrast enhancement:
• Followed by a persistent delayed phase:
• Type I enhancement curve:
• Non-enhancing internal septations may be seen
• Diagnosis:
• These lesions are easily biopsied under ultrasound guidance
• When a lesion has the typical features of a fibroadenoma on ultrasound and there are no clinical red flags:
• They can be safely followed clinically
• When lesions enlarge or have atypical imaging findings:
• Ultrasound-guided core biopsy is a minimally invasive outpatient procedure that will give a diagnosis with virtually no complications
• There may be a maximum diameter above which a biopsy should be done if no previous imaging is available:
• The reason for intervention based on size is that a phyllodes tumor may be indistinguishable from a fibroadenoma on ultrasound:
• A maximum diameter of 2.5 cm may be a useful benchmark for biopsy if you have no previous imaging
• Interval enlargement:
• Is an indication for biopsy
• Symptomatic, progressively enlarging masses or atypical presentations:
• May warrant surgical excision
• If a needle biopsy shows that a mass less than 2 centimeters in size is a fibroadenoma, with no other concerning features:
• It does not have to be surgically removed
• The patient’s core biopsy pathology demonstrating a fibroadenoma is consistent with the typical imaging findings of a smooth, round, hypoechoic mass:
• As the biopsy is concordant:
• No further intervention is needed:
• Follow-up for reassurance is acceptable
• Treatment and prognosis:
• They are benign lesions with minimal or no malignant potential
• The risk of malignant transformation is extremely low:
• Has been reported to range around 0.0125% to 0.3%
• Indications for biopsy include:
• Enlarging lesion
• Atypical findings on ultrasound
• A lesion above 2.5 cm and there are no previous studies for comparison
• Patient peace of mind:
• Some patients are simply not happy with a palpable mass in the breast without a histological diagnosis:
• This is a valid and reasonable indication for biopsy
• References:
• Tan BY, Tan PH A Diagnostic Approach to Fibroepithelial Breast Lesions. Surg Pathol Clin. 2018 Mar;11(1):17-42.
• The decision to administer radioiodine after thyroidectomy in patients with differentiated thyroid cancer is based upon the clinicopathologic features of each case
• The efficacy of radioiodine depends upon:
• Tumor-specific characteristics
• Sites of disease
• Patient preparation
• Dose
• Because of the careful risk stratification used in some studies, it is possible to identify specific patient and tumor characteristics which suggest that radioiodine may be beneficial:
• My approach outlined below is in agreement with the American Thyroid Association (ATA) guidelines on the role of postoperative radioiodine ablation:
• Low risk:
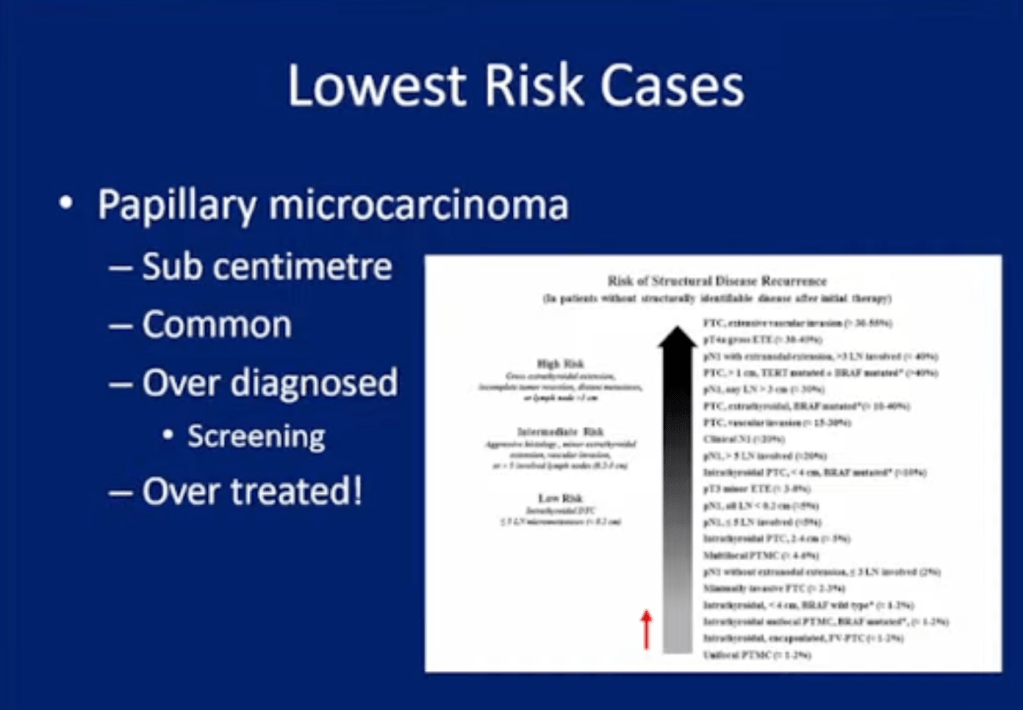
• The ATA guidelines do not routinely recommend administration radioiodine after lobectomy or total thyroidectomy to low-risk patients with differentiated thyroid cancer:
• This includes patients with:
• Unifocal cancer less than 1 cm without other high-risk features (eg, without distant metastases, vascular invasion, gross extrathyroidal extension, worrisome histologic subtypes):
• Even in the presence of small-volume regional lymph node metastases (less than five lymph nodes measuring less than 2 mm)
• Multifocal cancer when all foci are less than 1 cm and there are no other high-risk features:
• Without distant metastases
• Vascular invasion
• Gross extrathyroidal extension
• Worrisome histologic subtypes
• Intrathyroidal cancer in the 1 to 4 cm range without other high-risk features:
• Individual tumor- and patient-specific features may warrant radioiodine ablation in selected low-risk patients:
• As an example, low-dose radioiodine ablation (30 mCi) in low-risk patients with intrathyroidal tumors greater than 4 cm may be considered
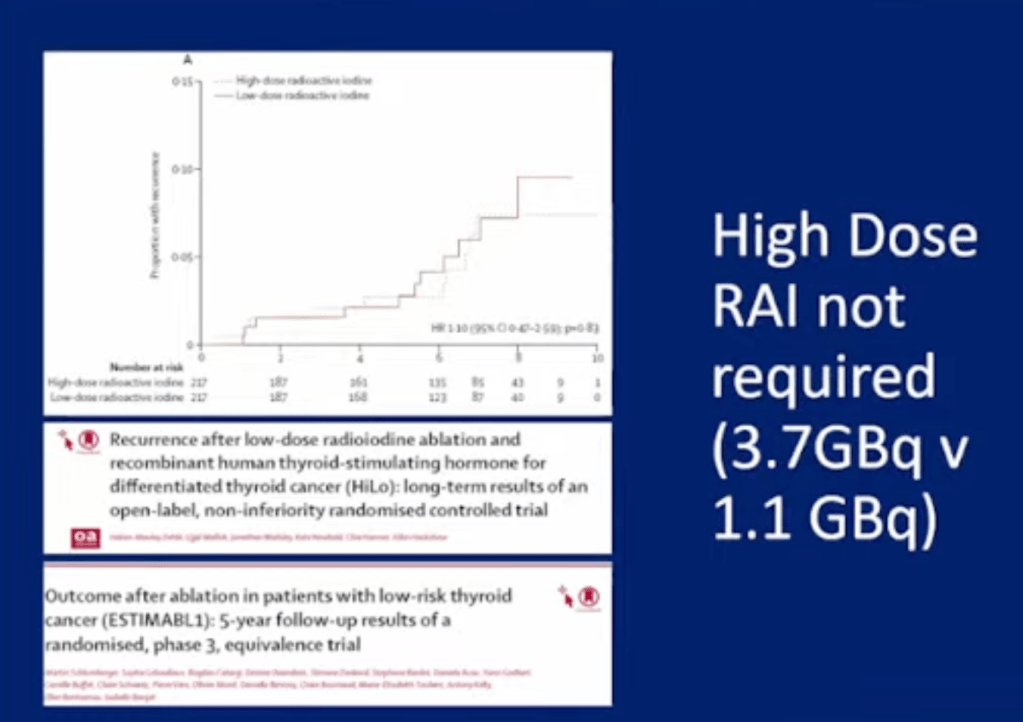
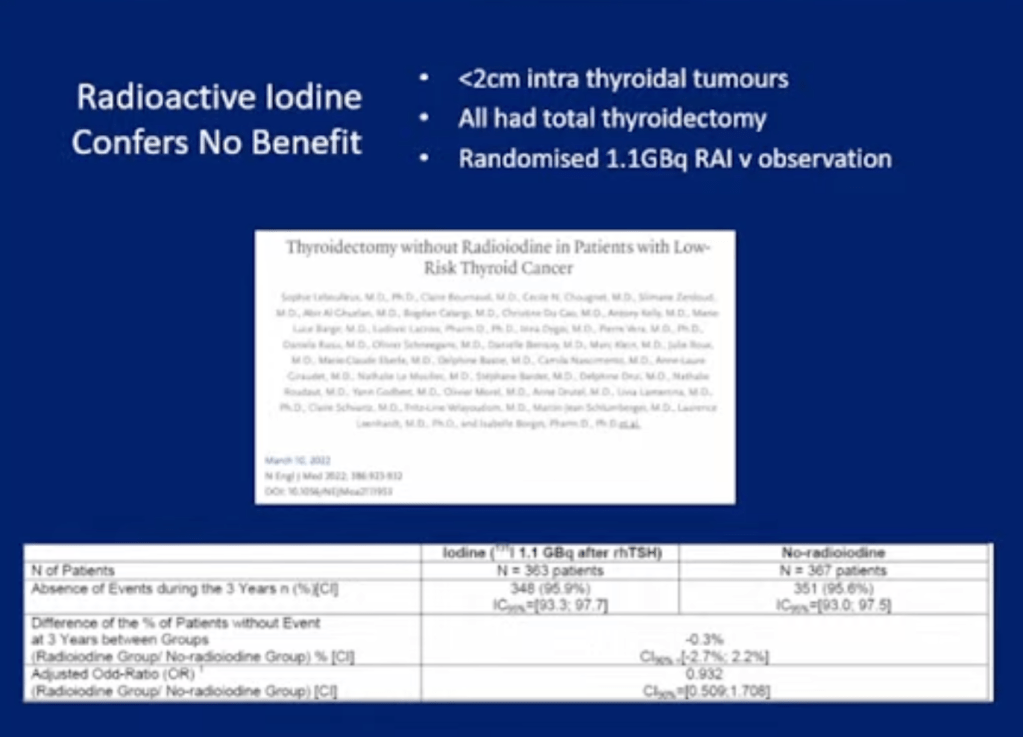
• In a randomized trial evaluating post-thyroidectomy radioiodine (1.1 GBq [30 mCi] after recombinant human TSH [rhTSH]) or no radioiodine therapy in 730 patients with low-risk differentiated thyroid cancer (multifocal pT1a with the sum of the longest diameters less than 2 cm, or pT1b, both with N0 or Nx, and without aggressive pathological subtypes or extrathyroidal extension, outcomes at three years were similar in the two groups, including the following:
• Primary disease-related events (identification of residual or recurrent disease or an elevated level of thyroglobulin or thyroglobulin antibodies) at three years occurred in:
• 4.1% and 4.4% of patients, respectively
• The frequency of BRAF mutation did not differ between cases with or without disease-related events:
• 61.5% versus 53.1% respectively
• An ATA excellent response at 10 months and 3 years occurred in:
• 86.8% and 86.3%, respectively, after 10 months
• 73% and 74.1%, respectively, after 3 years
• Quality-of-life scores related to:
• Anxiety, distress, and fear of recurrence
• In systematic reviews and meta-analyses of observational data:
• There was no benefit of radioiodine in low-risk patients with regard to either:
• Overall recurrence rate or disease-specific mortality
• As an example, in a retrospective analysis of 1129 patients who underwent total thyroidectomy for differentiated thyroid cancer and received radioiodine based upon risk assessment:
• The majority of patients with low-risk local disease (age less than 45 years, papillary cancer less than 4 cm without extrathyroidal extension, and without distant metastases):
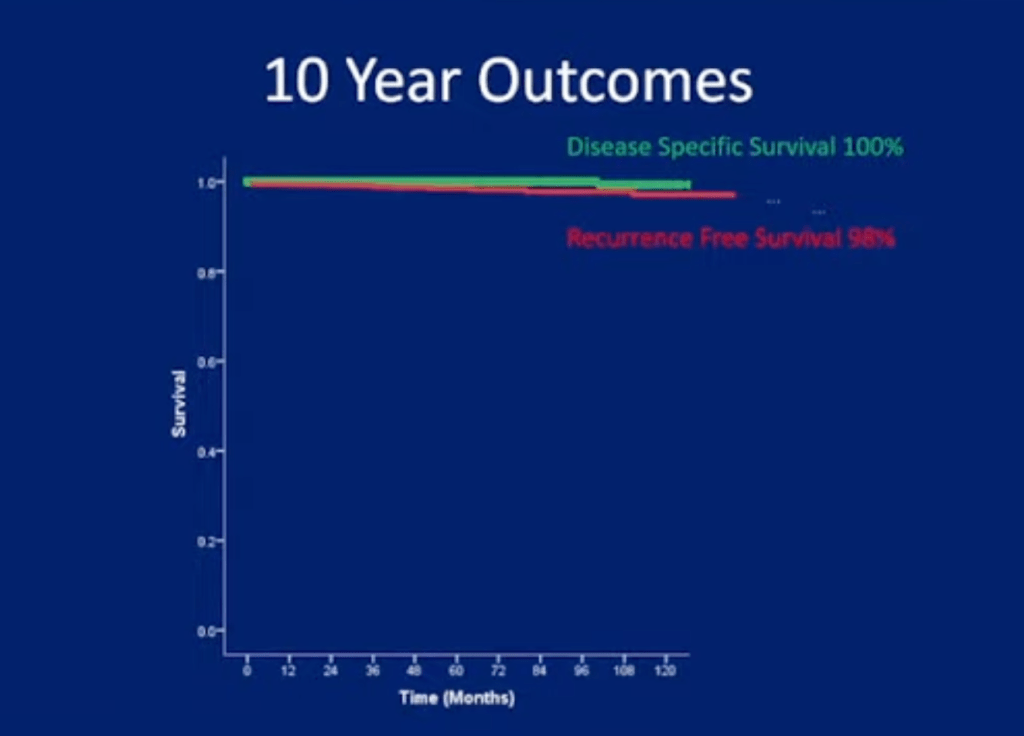
• Had low rates of recurrence and high rates of survival when managed without radioiodine;
• Five-year recurrence-free survival greater than 97%
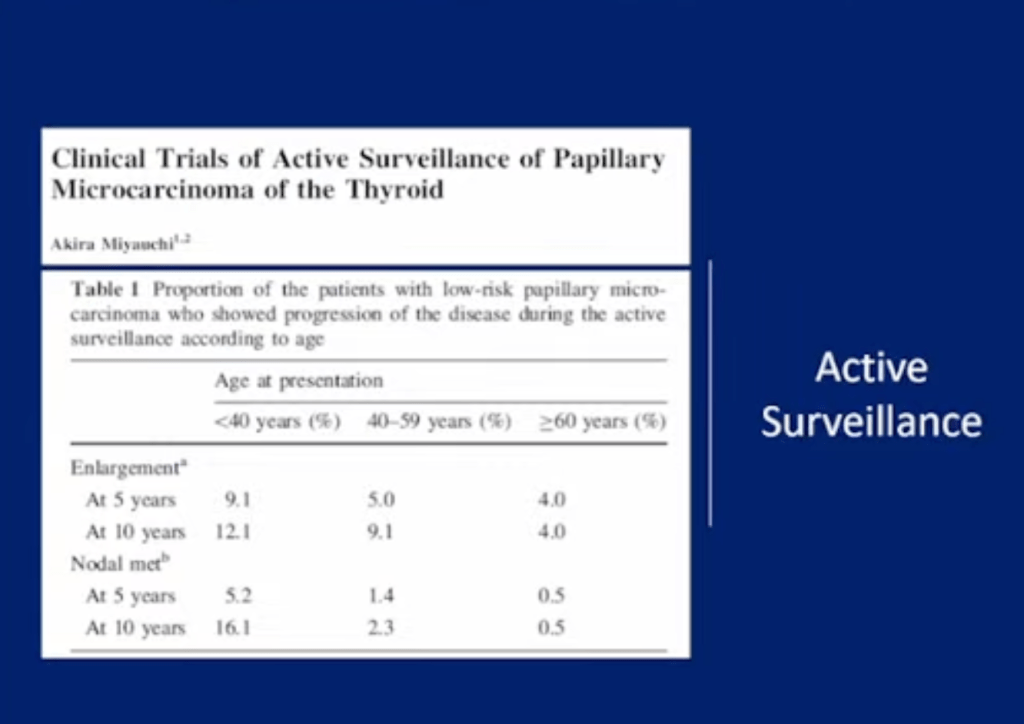
• Another retrospective study similarly showed no benefit of radioiodine ablation on disease recurrence in patients with papillary thyroid microcarcinoma (unifocal or multifocal):
• In this study, there was no disease-related mortality
• Intermediate risk:
• The administration of radioiodine after total thyroidectomy is considered in selected intermediate-risk patients depending upon specific tumor characteristics, including:
• Microscopic invasion into the perithyroidal soft tissue
• Clinically significant lymph node metastases outside of the thyroid bed
• Other higher-risk features:
• Vascular invasion
• More aggressive histologic subtypes such as:
• Tall cell histology
• Columnar cell histology
• Insular histology
• Poorly differentiated histology
• When the combination of age, tumor size or multifocality, lymph node status, and individual histology:
• Predicts an intermediate to high risk of recurrence or death from thyroid cancer
• In the absence of evidence supporting survival benefit for all of the factors listed:
• Clinical judgment and an individualized approach to care are important
• Postoperative serum thyroglobulin is a critical factor that should be routinely integrated into clinical decision-making:
• For example, in a retrospective cohort study, there was no difference in the five-year recurrence-free survival among intermediate-risk patients who did or did not receive radioiodine therapy:
• When postoperative unstimulated serum thyroglobulin levels were less than 1 ng/mL
• There are limited data showing a benefit of radioiodine in intermediate-risk patients:
• In a study using the National Cancer Database registry, which included 21,870 patients with intermediate-risk papillary thyroid cancer who had total thyroidectomy with or without radioiodine:
• Patients who received radioiodine had improved overall survival (hazard ratio [HR] 0.71, 95% CI 0.62-0.82)
• In the National Thyroid Cancer Treatment Cooperative Study Group (NTCTCSG), a multicenter thyroid cancer registry that has analyzed the outcomes of nearly 5000 patients with differentiated thyroid cancer:
• Multivariable analysis showed that radioiodine ablation was associated with:
• Improvement in overall survival in stage II patients:
• But this did not reach statistical significance (relative risk [RR] 0.67, 95% CI 0.36-1.28)
• High risk:
• Based on the ATA guidelines high risk patients are routinely treated with radioiodine after total thyroidectomy, including patients with:
• Distant metastases
• Macroscopic tumor invasion,
• Incomplete tumor resection with gross residual disease
• In the National Thyroid Cancer Treatment Cooperative Study Group:
• Radioiodine was associated with improved overall survival in stage III patients (RR 0.66, 95% CI 0.46-0.98), with similar but nonsignificant improvement in stage IV (RR 0.70, 95% CI 0.46-1.10)
• In addition, data prospectively collected from the Surveillance, Epidemiology, and End Results (SEER) database showed:
• Benefit from radioiodine in patients older than 45 years with primary tumors greater than 2 cm, with disease in the lymph nodes at initial diagnosis, and with distant metastatic disease
• The benefits and dose limits of iodine-131 (131-I) therapy for metastatic disease were evaluated in a retrospective analysis of 444 patients treated between 1953 and 1994 (analysis of whole-body iodine scans and conventional radiographs):
• 43% of the 295 patients with radioiodine uptake achieved resolution of radioiodine-avid metastases on iodine scan and negative conventional radiographs
• Additional features of patients in this group included the following:
• They were more likely to be younger:
• With differentiated tumors
• 96% of these patients were given cumulative doses of 100 to 600 mCi (3700 to 22,000 MBq)
• 7% had a recurrence
• 10-year survival was 92% in this group:
• Compared with only 19% in patients who did not achieve resolution of the radioiodine-avid metastatic lesions
👉Common labs ordered in the workup of patients with Primary hyperparathyroidism include a serum calcium (+/- ionized calcium), albumin (for correction of total serum calcium level), PTH, phosphate, creatinine, 25-hydroxy vitamin D, and a 24-hour urine calcium & creatinine.
👉Hypercalcemia with with an elevated PTH with normal kidney function and without hypocalciuria indicates primary hyperparathyroidism.
👉However, some patients with this disease will have hypercalcemia with an “inappropriately normal” PTH – this can be a common cause of delayed diagnosis.
PHPT is symptomatic in more than 95% of the cases:
If proper attention is payed to the subtle symptoms and signs that this disease can produce due to the fluctuating calcium levels
The “classic” pentad of:
Kidney stones
Painful bones
Abdominal groans
Psychic moans
Fatigue overtones
Are rarely seen today since the advent and general use of automated blood analyzers in the early 1970s
At this point in time most patients present with:
Fatigue (# 1 symptom)
General malaise
Decrease levels of energy
Anxiety
Irritability leading to decrease social interaction
Depression (10% of cases)
Memory loss
Decrease concentration
Decrease ability to learn new things
Decrease ability to complete daily tasks at home
Decrease ability to complete daily tasks at work
Decrease social interaction
Insomnia
Arthralgia’s (32% of the cases)
Myalgia’s (14% to 41% of the cases)
Bone pain
Muscle weakness:
Specially proximal muscle groups
Intermittent headaches
Polydipsia
Polyuria
Nocturia
Nausea (24% of the cases)
Anorexia (15% of the cases)
Non-specific abdominal pain
Heartburn (30% of the cases)
Constipation (33% of the cases)
Palpitations
Arrhythmias:
Usually atrial fibrillation
Elevated blood pressure
Thinning of the hair:
Specially in women in the frontal region
Pruritus
Patients with PHPT also tend to score lower than healthy controls:
When evaluated by general multidimensional health assessment tools such as the Medical Outcomes Study Short-Form Health Survey (SF-36) and other specific questionnaires
PHPT that is truly “asymptomatic” is a rare occurrence:
Seen in less than 5% of patients:
This is important when talking about management based on current guidelines
Patients with PHPT have some degree of renal dysfunction or symptoms:
In approximately 80% of the cases
The renal manifestations implicated with PHPT are:
Decreased glomerular filtration rate
Hypercalciuria
Nephrolithiasis
Nephrocalcinosis
Impaired urinary concentrating ability:
Sometimes leading to:
Polyuria
Polydipsia
Nocturia
Reduced fractional phosphate reabsorption:
Leading to hypophosphatemia
Increased urinary exertion of magnesium
Nephrolithiasis was previously reported in approximately 40% to 80% of patients:
But now occur only in about:
20% to 25% of the cases
The pathophysiology is thought to be related to the filtered load of calcium in the glomerulus:
That increases proportionately with the degree of hypercalcemia
Most renal stones in patients with PHPT are composed of calcium oxalate:
Although slightly alkaline urine may favor the precipitation of:
Calcium phosphate stones
Stone formers are more likely to be hypercalciuric:
But less than one-third of the hypercalciuric patients with PHPT:
Actually develop renal stones
Hypercalciuria is not a predictor of nephrolithiasis in patients with PHPT:
Is no longer considered as an indication for surgery
At the present time, it is almost impossible to securely foresee which patients with PHPT would develop a new onset nephrolithiasis:
Based on the biochemical measurements in the blood or urine (including hypercalciuria)
Nephrocalcinosis:
Which refers to renal parenchymal calcification:
Is found in less than 5% of patients and is more likely to lead to renal dysfunction
The incidence of hypertension is variable:
Anywhere between 30% to 50% of patients with PHPT
Hypertension appears to be more common in:
Older patients and correlates with the magnitude of renal dysfunction and, in contrast to other symptoms, is least likely to improve after parathyroidectomy
Another plausible explanation of the origin of hypertension in patients with PHPT is the synthesis of parathyroid hypertensive factor that triggers an increase in blood pressure
The elevated levels of PTH:
Is also linked with the disruption in the renin-angiotensin-aldosterone system
Skeletal manifestations including osteopenia, osteoporosis, and osteitis fibrosacystica:
Are found in approximately 15% of patients with PHPT
PHPT is linked with a reduction in bone mineral density (BMD), particularly in the cortical bone, such as in the distal third of the radius m.
In the lumbar region, composed all most exclusively by trabecular bone, and in the femoral region, composed by cortical and trabecular bone, the decrease in BMD is less severe [88-90]. Osteitis fibrosacystica, a skeletal manifestation that is rarely seen today (seen in less than five percent of patients with PHPT), is caused by an increase in bone turnover and can be determined by finding an elevated serum alkaline phosphatase level [91]. The radiologic findings seen in patients with PHPT with bone disease are characterized by subperiosteal resorption (most obvious on the radial aspect of the middle phalanx of the second and third fingers), bone cysts, and tufting of the distal phalanges [92], which are best evaluated on plain x-rays of the hands. Brown or osteoclastic tumors (accumulations of osteoclasts and fibrous tissue) and bone cysts also may be present [93]. Brown tumors have a slightly greater incidence in PHPT than in secondary HPT (3% versus 2%). In patients with chronic kidney disease, persistent and excessive urinary calcium elimination can lower serum calcium level and lead to an increase in PTH secretion. This results in mobilization of calcium from the bones through rapid osteoclastic turnover of bone to maintain normal serum calcium levels [94]. In regions where bone loss is exceptionallyfast, hemorrhage, and reparative granulation tissue, with active, vascular, proliferating fibrous tissue may replace the normal marrow contents, resulting in a brown tumor. Hemosiderin imparts the brown color(hence the name of the lesions). The skull also may be affected and appears mottled with a loss of definition of the inner and outer cortices.