- Clinical and pathologic staging of patients with cancer is valuable for many reasons, including the following:
- To estimate risk of recurrence and disease-specific mortality for an individual patient
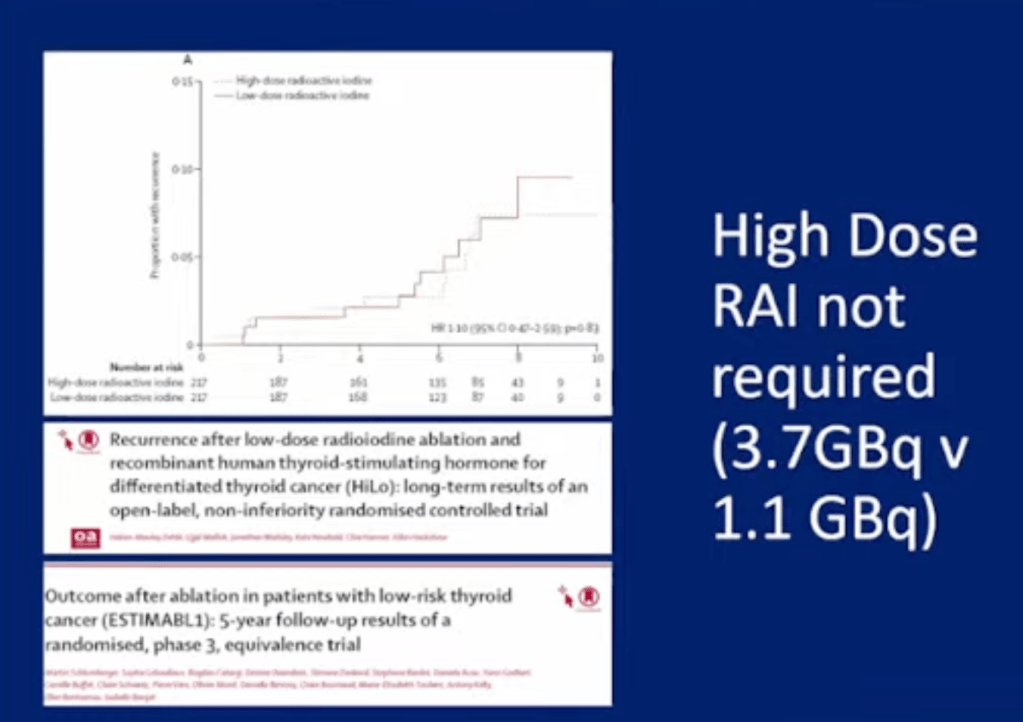
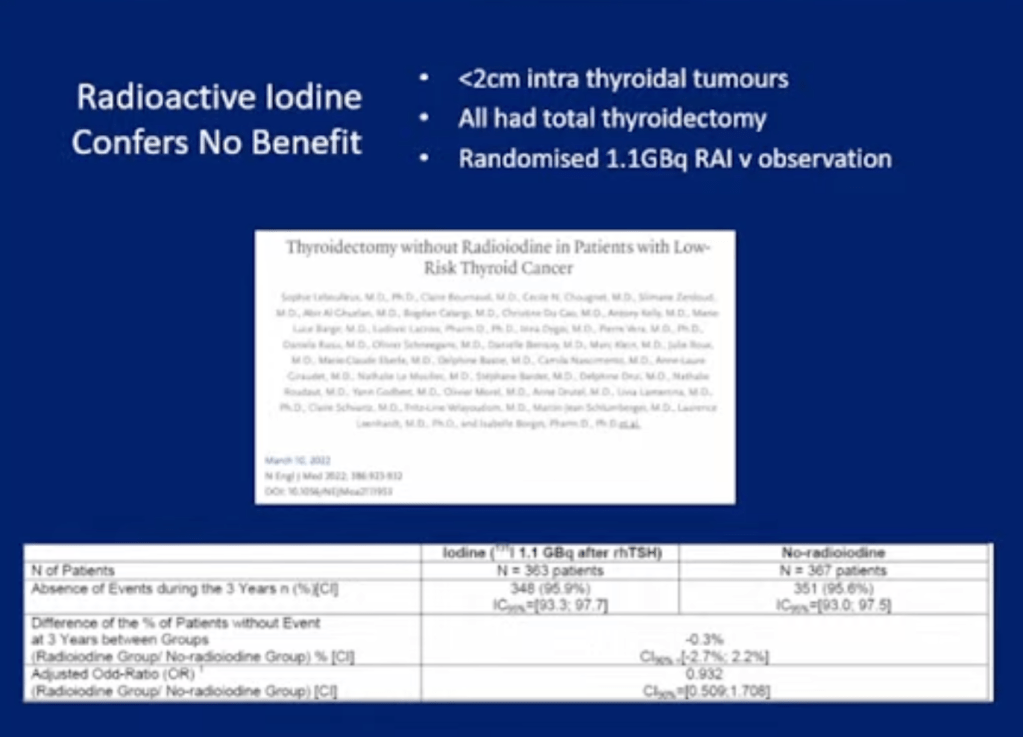
- To tailor decisions regarding postoperative adjunctive therapy (such as the need for radioiodine [RAI] ablation and degree of thyroid-stimulating hormone [TSH] suppression):
- To the patient’s risk for disease recurrence and mortality
- To make decisions regarding the frequency, modality, and intensity of follow-up based upon an individual patient’s risk of recurrence and mortality
- To enable accurate communication regarding a patient among health care professionals
- To allow evaluation of differing therapeutic strategies applied to comparable groups of patients in clinical studies
- To provide “a method of conveying clinical experience to others without ambiguity
- Initial postoperative staging:
- You can use the several staging systems to estimate disease-specific mortality:
- Tumor, node, metastasis (TNM) staging systems
- MSKCC:
- Grade, Age, Metastases, Extent, Size (GAMES)
- Mayo Clinic:
- Metastases, Age, Complete Resection, Invasion, Size (MACIS)
- Karolinska Hospital and Institute:
- DNA ploidy, Age, Metastases, Extent, Size (DAMES)
- Age, Grade, tumor Extent, Size (AGES)
- Lahey Clinic:
- Age, distant Metastasis, Extent, Size (AMES)
- Clinical and pathologic staging system:
- Such as the American Thyroid Association (ATA) system:
- To estimate the risk of recurrence
- Such as the American Thyroid Association (ATA) system:
- You can use the several staging systems to estimate disease-specific mortality:
- Re-staging during follow-up:
- These initial risk assessments are then:
- Actively modified based upon data obtained during follow-up:
- That reflect the individualized patient’s response to therapy
- Actively modified based upon data obtained during follow-up:
- This dynamic risk assessment approach:
- Allows for more accurate risk assessments:
- Than either a static estimate of risk based on the:
- TNM staging system or the ATA risk of recurrence classification system
- Than either a static estimate of risk based on the:
- Allows for more accurate risk assessments:
- These initial risk assessments are then:
- The ATA recommends the TNM staging system:
- For all patients with differentiated thyroid cancer and any of the:
- Postoperative clinicopathologic staging systems:
- To achieve more accurate risk factor stratification
- Postoperative clinicopathologic staging systems:
- For all patients with differentiated thyroid cancer and any of the:
- It should be recognized, however:
- No staging system reliably predicts outcome in individual patients:
- Clinicians should use individual clinicopathologic characteristics:
- To determine the specific treatment for a given patient
- Clinicians should use individual clinicopathologic characteristics:
- No staging system reliably predicts outcome in individual patients:

#Arrangoiz #ThyroidSurgeon #CancerSurgeon #SurgicalOncologist #HeadandNeckSurgeon #EndocrineSurgery #ThyroidCancer #Miami #Mexico #MountSinaiMedicalCenter #Surgeon #Teacher #ThyroidNodules #RadioactiveIodine #RAI #PTC #MSMC
