👉The external branch of the superior laryngeal nerve (EBSLN) has been labelled ‘the neglected nerve’ of thyroid surgery.
👉Most surgeons have simply attempted to avoid this nerve on the assumption that so doing will prevent injury; however, it is now recognized that injury is relatively common and associated with the potential for significant impairment, espe- cially for those who use their voices professionally.
👉I was taught to always attempt to identify the nerve and recommend doing so.
👉Recently Aina and Hisham have shown that the nerve can be routinely identified in over 90% of cases, a level that sets a new benchmark for head and neck surgeons / endocrine surgeons.
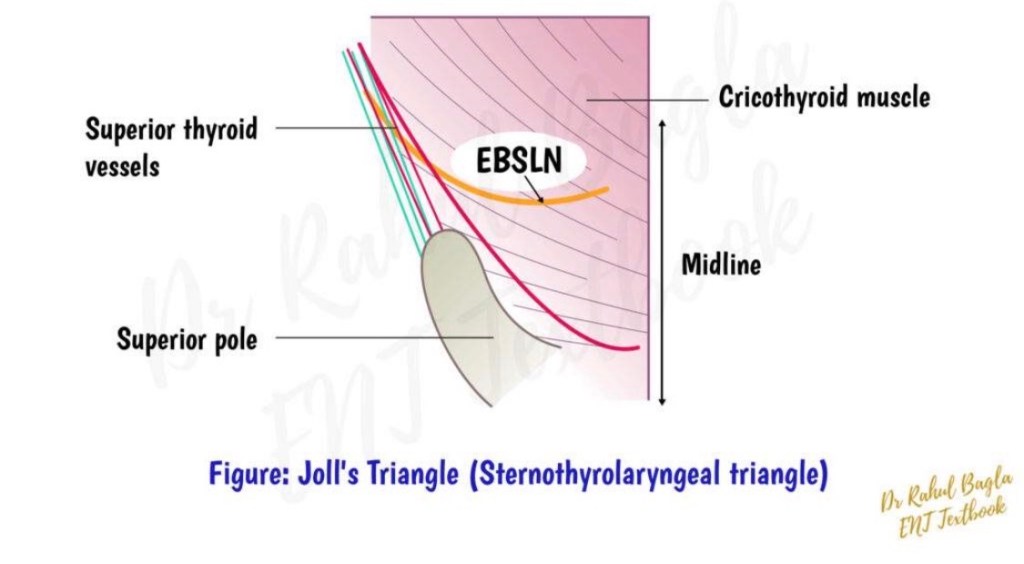
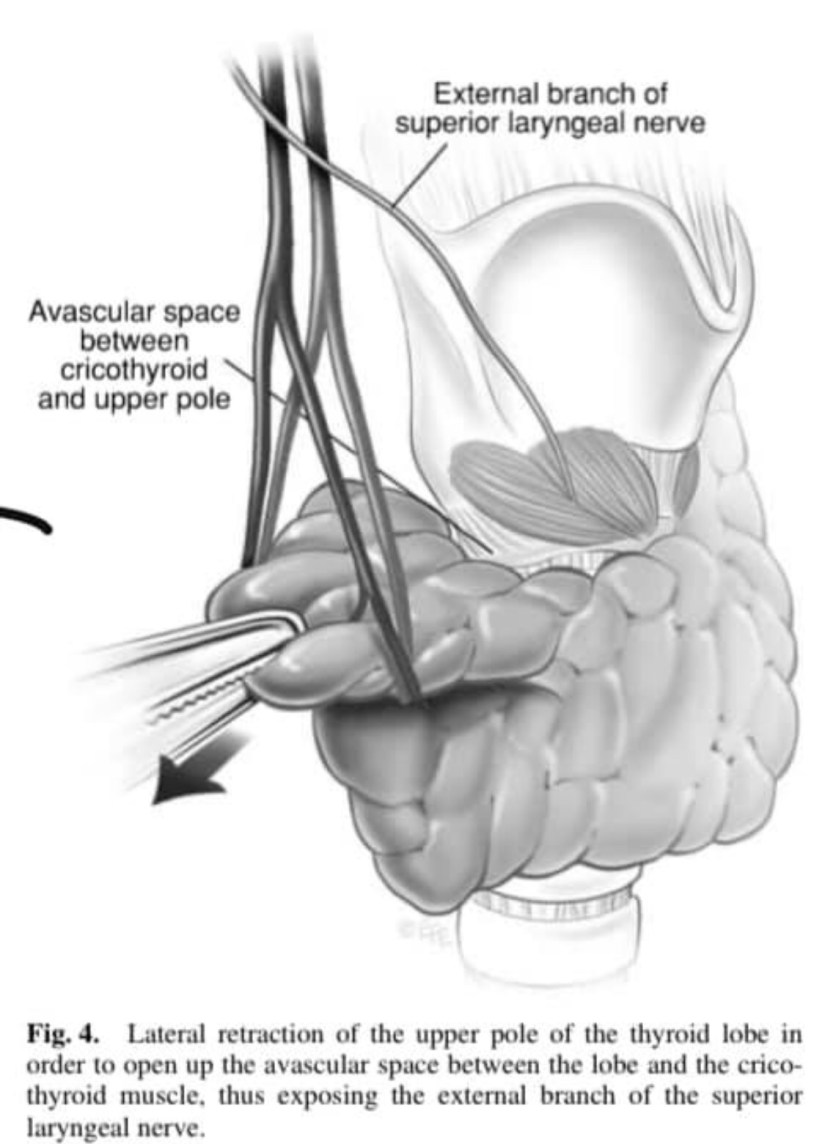
👉The key to identifying the nerve is to develop the avascular plane between the cricothyroid muscle and the medial border of the upper pole of the thyroid lobe, a manoeuvre facilitated by lateral retraction of the lobe.
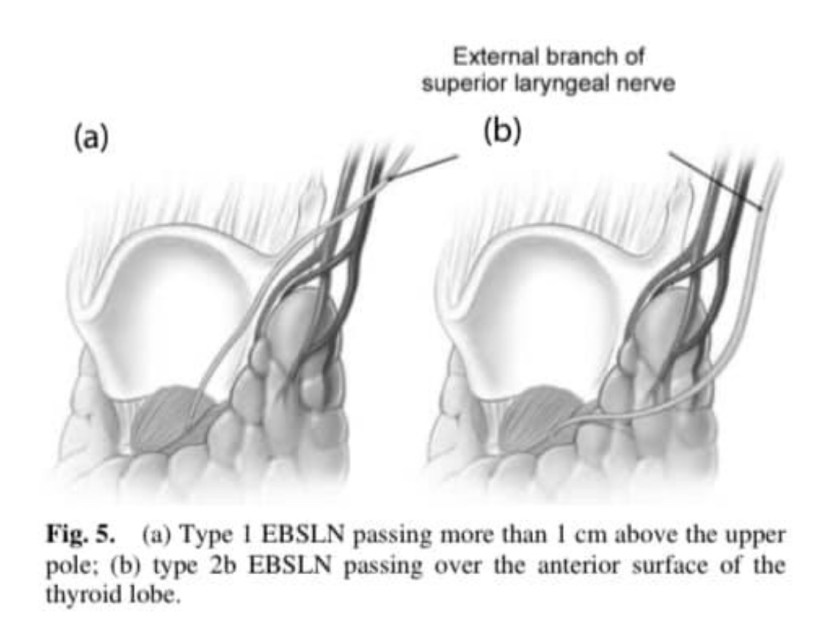
👉Awareness of the various positions of the EBSLN according to the Cernea classification is also essential if the nerve is to be both identified and preserved.
👉Type 1 EBSLN are located well clear of the thyroid, more than 1 cm above the upper pole of the lobe passing directly into the cricothyroid muscle.
👉Type 2a nerves pass in the vicinity of the superior thyroid vessels as they enter the gland substance.
👉Type 2b nerves cross over the anterior surface of the thyroid lobe.
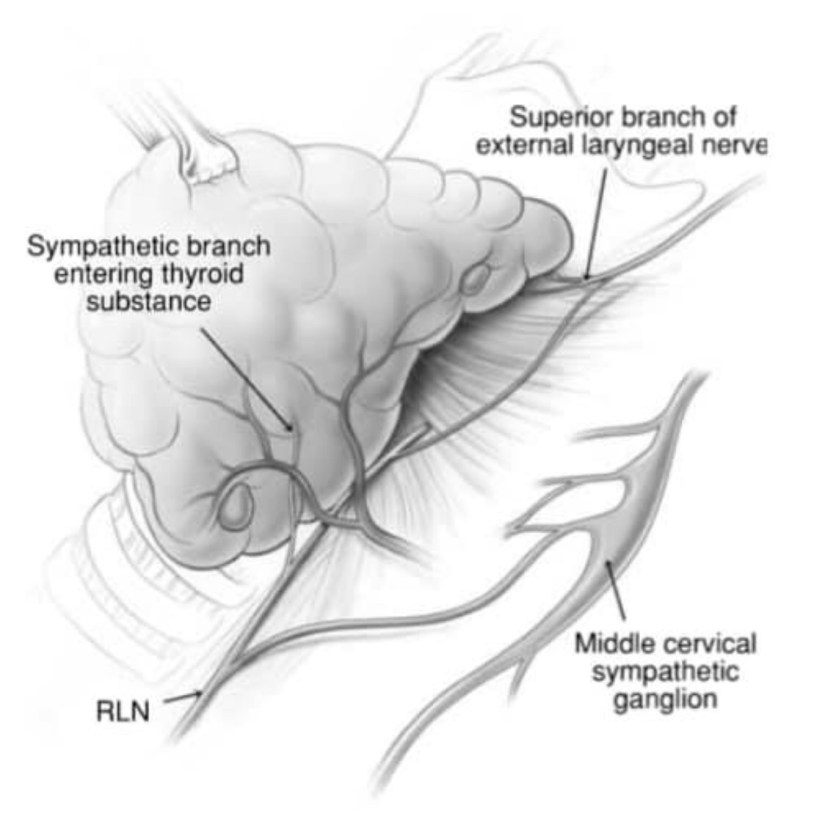
👉Awareness of the anatomic variations, such as the nerve of Galen, a direct communication between the RLN and EBSLN, is important in avoiding injury to the nerve.
#Arrangoiz
#HeadandNeckSurgeon
#ThyroidSurgeon
#ParathyroidSurgeon
#CancerSurgeon
#SurgicalOncologist
#EndocrineSurgery
#Teacher
#MSMC
#MountSinaiMedicalCenter