SENOMAC enrolled some patients with ECE, cT3, and men
Prespecified subgroup analyses did not show detriment with ALND omission:
Though numbers are smaller – supporting wider generalizability makadu.live
After mastectomy with 1 to 2 positive SLNs, do I need ALND?
Not routinely – With planned comprehensive RNI, ALND can be omitted (AMAROS, SENOMAC) a position reflected in the 2025 ASTRO-ASCO-SSO PMRT guideline language emphasizing less invasive axillary management with nodal RT PubMed+2PubMed+2
Omission of any axillary surgery (SLNB-omission):
SOUND (JAMA Oncol 2023) – who can skip SLNB entirely?
Women with small tumors and negative axillary ultrasound:
Had noninferior 5-yr distant DFS with no axillary surgery vs SLNB
If axillary pathology doesn’t change therapy:
Omission is safe
INSEMA (NEJM 2024/2025) – does it reinforce SLNB omission?
Yes:
In cT1 to cT2 cN0 undergoing BCS + WBRT, omitting SLNB was noninferior for invasive DFS, with fewer arm morbidities:
Broadening omission beyond SOUND’s entry criteria
Guideline impact – what does ASCO 2025 now recommend?
ASCO now supports SLNB omission for select postmenopausal ≥50, HR+/HER2-, G1–2, ≤2 cm tumors with negative AUS undergoing BCS + RT, when nodal status won’t alter adjuvant therapy
How do I counsel a 65-year-old with 1.5 cm HR+/HER2–, AUS-negative tumor?
Discuss SLNB omission per ASCO 2025, referencing SOUND / INSEMA
Emphasize shared decision-making and document that nodal status won’t change systemic therapy / RNI plans
Does negative AUS define cN0 reliably enough to omit surgery?
In SOUND / INSEMA, AUS was adequate for selection:
Axillary failures were rare with omission when systemic / RT plans were appropriat:
Still, ensure imaging quality and consider biology.
Pathology definitions and “what counts”
Define ITCs vs micrometastases (AJCC 8e):
ITCs:
< 0.2 mm or < 200 cells (N0[i+])
Micrometastases:
0.2 mm to 2 mm (N1mi)
Management parallels the trials:
Micrometastases (IBCSG 23-01) often no ALND:
ITCs generally node-negative
Do ITCs change indications for ALND or RNI
ITCs typically do not mandate ALND:
Decisions on RNI hinge on comprehensive risk assessment rather than ITCs alone (Use institutional protocols)
Neoadjuvant chemotherapy (NAC): SLNB and TAD
ACOSOG Z1071 – what did we learn?
In biopsy-proven cN1→ycN0 after NAC:
SLNB had an FNR ≈ 12%:
Improved by dual tracer and retrieving ≥ 3 SLNs
Capturing the clipped node lowered the FNR further – ushering in targeted axillary dissection (TAD)
SENTINA – why was FNR a concern?
Complex 4-arm RCT showed higher FNRs when SLNB was performed after NAC in initially node-positive patients, especially when only 1 to 2 SLNs were retrieved:
Driving optimization:
Dual mapping, ≥ 3 SLNs and TAD
SN-FNAC (JCO 2015) – can SLNB be accurate post-NAC in cN+?
With mandatory IHC, ID rate 87.6% and FNR 8.4%:
When ≥ 2 SLNs were removed – evidence that optimized technique can make SLNB acceptable after NAC in prior cN+
GANEA-2 (2019) – safety signal?
Prospective multicenter study supported feasibility and safety of post-NAC SLNB with low axillary failure when using optimized protocols; informs modern post-NAC algorithms
What is TAD and why do it?
Targeted axillary dissection combines SLNB + removal of the pre-treatment clipped node:
To slash FNR vs SLNB alone and better mirror basin response – core idea from MD Anderson implementation work
RISAS / TAD accuracy – what’s the FNR
Multicenter diagnostic study of radioactive iodine seed localization (RISAS):
FNR 3.5%, NPV 92.8% – strong diagnostic performance for restaging after NAC
MARI protocol – how is it different?
Marking the positive node with a seed pre-NAC and excising it post-NAC; with PET-CT integration:
MARI can avoid ALND in ~80% of cN+ while keeping 3-yr axillary recurrence-free interval ~98%
TAD outcomes – can we safely omit ALND in responders?
Cohorts show low 3-yr axillary recurrence with TAD alone in good responders (and no survival decrement vs TAD + ALND in selected patients):
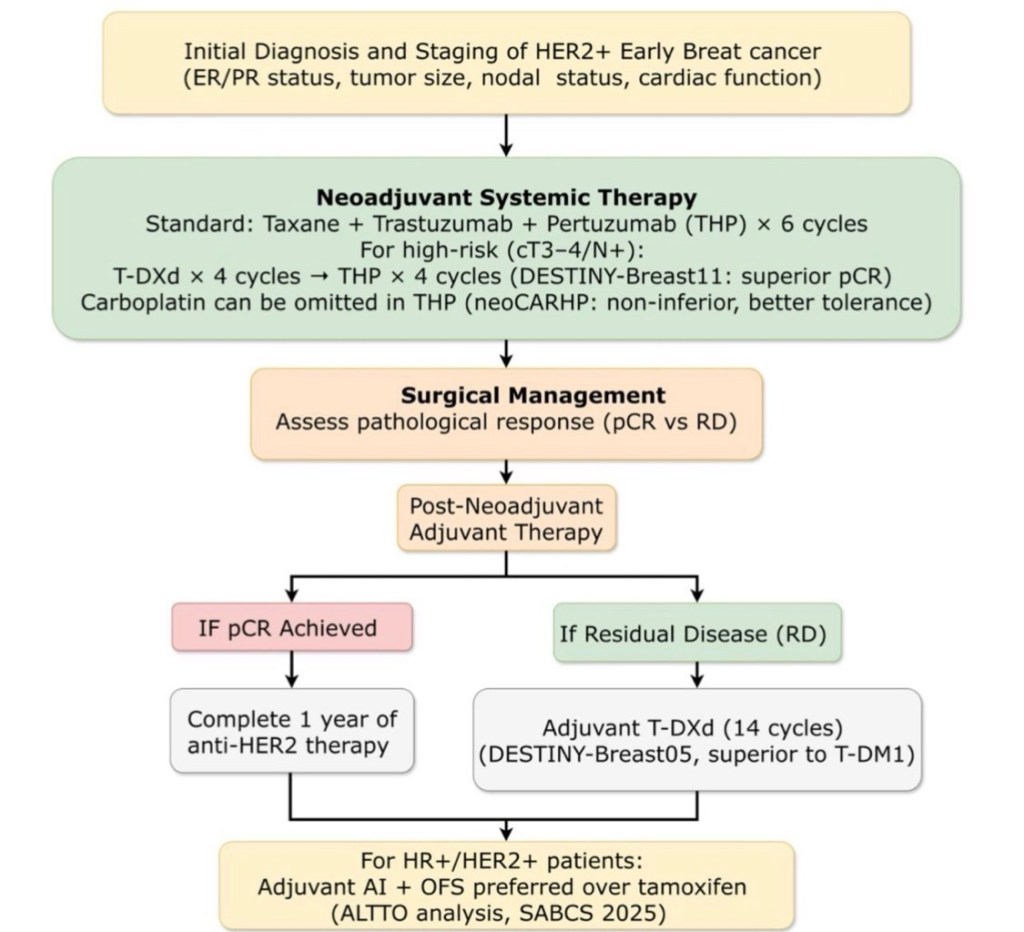
The treatment landscape for HER2-positive early breast cancer (EBC) is evolving rapidly — and trastuzumab deruxtecan (T-DXd) is emerging as a potential new standard in both the neoadjuvant and adjuvant settings.
🔹 Neoadjuvant Setting
DESTINY-Breast11
T-DXd followed by THP (docetaxel + trastuzumab + pertuzumab) demonstrated:
Significantly higher pathologic complete response (pCR) rates compared with standard anthracycline-based regimens A chemotherapy-sparing strategy with reduced anthracycline exposure Favorable tolerability profile consistent with prior T-DXd data
📊 Early reports show pCR rates approaching ~65–70%, exceeding historical benchmarks for standard neoadjuvant regimens (typically ~55–60%).
Clinical Implication:
We may be entering an era of antibody–drug conjugate (ADC)-based neoadjuvant intensification, potentially redefining the backbone of HER2-directed therapy.
Reference:
Hurvitz SA et al. DESTINY-Breast11. Presented at ESMO 2024 / SABCS 2024 (late-breaking data).
🔹 Adjuvant Setting
DESTINY-Breast05
For patients with residual invasive disease after neoadjuvant therapy, T-DXd demonstrated:
53% reduction in risk of invasive disease–free survival (iDFS) events compared with T-DM1 Superior invasive disease–free survival Manageable toxicity, with ILD rates consistent with prior experience
This builds upon the paradigm established by KATHERINE, where T-DM1 replaced trastuzumab in patients with residual disease.
Now, T-DXd appears poised to replace T-DM1 in this high-risk population.
Reference:
DESTINY-Breast05. Presented at ASCO 2025.
von Minckwitz G et al. KATHERINE trial. NEJM. 2019;380:617–628.
🔬 Why This Matters
We are witnessing:
A shift from monoclonal antibodies → ADC-based escalation Earlier deployment of highly potent HER2-directed agents Refinement of risk-adapted therapy based on response
If adopted into guidelines (NCCN, ASCO, ESMO), this could:
Redefine the management of residual disease Potentially reduce recurrence risk further in high-risk HER2+ EBC Change neoadjuvant sequencing strategies
⚠️ Considerations
ILD/pneumonitis risk requires vigilance Cost-effectiveness and long-term survival data pending Optimal sequencing with pertuzumab still being clarified
📌 Bottom Line
T-DXd is no longer just a metastatic drug.
It is rapidly reshaping the curative-intent HER2+ early breast cancer algorithm.
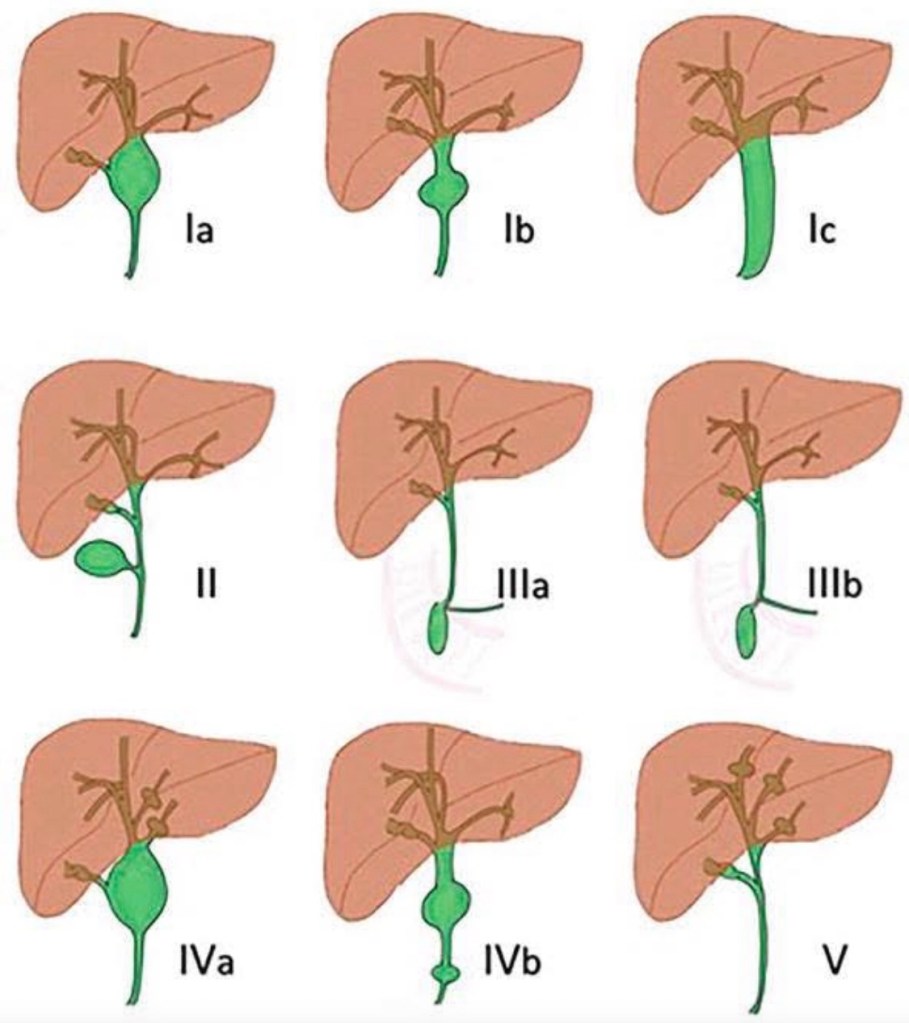
Choledochal cysts are congenital cystic dilatations of the biliary tree. They are associated with an abnormal pancreaticobiliary junction and carry a significant lifetime risk of malignancy (especially cholangiocarcinoma).
Classification (Todani Classification)
The most widely used system is the Todani classification, which divides choledochal cysts into five main types:
Type I – Extrahepatic bile duct dilatation (most common, 50–80%) • Ia – Diffuse cystic dilatation of CBD • Ib – Focal segmental dilatation • Ic – Fusiform dilatation of CBD
Management: → Complete excision of extrahepatic bile duct + Roux-en-Y hepaticojejunostomy
Type II – True diverticulum of CBD • Saccular outpouching from extrahepatic bile duct
Management: → Diverticulectomy ± primary closure of CBD
Type III – Choledochocele • Intraduodenal dilatation of distal CBD (within ampulla)
Type IV – Multiple cysts • IVa – Both intrahepatic and extrahepatic involvement • IVb – Multiple extrahepatic cysts only
Management: → Excision of extrahepatic bile duct + Roux-en-Y hepaticojejunostomy → Liver resection if localized intrahepatic disease → Liver transplant if diffuse severe intrahepatic disease
Type V – Caroli Disease • Multiple intrahepatic cystic dilatations only
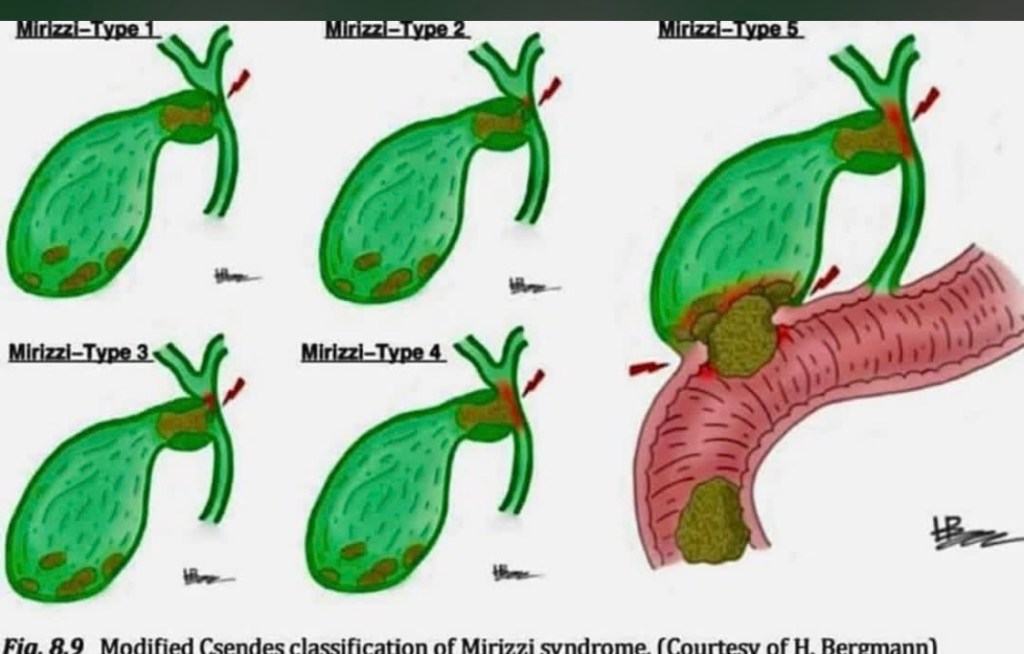
Mirizzi Syndrome: The rare but challenging complication where an impacted gallstone in the cystic duct or Hartmann’s pouch causes external compression or fistulization into the common bile duct. The modified Csendes classification grades severity from Type 1 (external compression only) through Type 5 (cholecystobiliary fistula with gallstone ileus). Type 1 shows simple compression without fistula formation. Type 2 involves erosion affecting less than one-third of the bile duct circumference. Type 3 extends to involve one-third to two-thirds of the duct. Type 4 shows complete destruction of the bile duct wall. Type 5 adds the complication of cholecystoenteric fistula with gallstone ileus. Recognition is critical during cholecystectomy as misidentification can lead to bile duct injury. Higher types require bile duct reconstruction
New 5-Year Evidence Supporting Radiofrequency Ablation (RFA) in Early-Stage Breast Cancer
I’m pleased to share results from the RAFAELO Phase 3 multicenter trial — published online in Annals of Surgical Oncology (Feb 18, 2026) — assessing radiofrequency ablation (RFA) as a minimally invasive alternative to partial mastectomy in early-stage breast cancer.
• Population: 370 women with solitary Tis–T1 (≤1.5 cm), N0M0 breast carcinomas.
• Intervention: Percutaneous RFA followed by whole-breast radiation (45–60 Gy).
• Primary Endpoint: 5-year ipsilateral breast tumor recurrence-free survival (IBTRFS).
📈 Key Findings
✔ At 5 years, IBTRFS was 98.6% (90% CI 97.1–99.3%), exceeding the pre-specified noninferiority margin of 90%.
✔ Only 2 ipsilateral recurrences were observed at 5 years.
✔ Grade ≥3 skin ulceration was rare (1/370 patients), underscoring a favorable safety profile.
✔ These results suggest that RFA with adjuvant radiation may be comparable to partial mastectomy in appropriately selected early-stage patients.
🏷 Clinical Significance
This large prospective trial provides the most robust long-term evidence to date that RFA — a less invasive approach — may be a viable local-control strategy in small, node-negative breast cancers. These findings reinforce ongoing interest in expanding treatment options that balance oncologic safety with patient-centred care (e.g., cosmesis, procedural morbidity).
Optional Add-Ons for Engagement
🔹 Thanks to the RAFAELO Study Group and contributing centers for advancing patient-centred oncology.
🔹 Looking forward to longer follow-up, quality-of-life data, and comparative trials against standard surgery
Conference Overview Held March 12–15, 2025 in Vienna with >3,100 global participants. Focused on early breast cancer (BC): evidence, controversies, consensus, and breakthroughs. Included lectures, debates, poster sessions, and the renowned St. Gallen Consensus Session. Hansjoerg Senn Memorial Lecture was introduced to honor a major contributor to BC care.
🔬 Systemic Therapy & Novel Agents Goal of early BC therapy is to improve overall survival (OS) through better systemic and local treatment. Surrogate endpoints (e.g., pathological complete response) are crucial for accelerating drug development. New endocrine therapies (SERDs) are being evaluated, with emphasis on QoL and resistance mechanisms. Anti-HER2 advances from metastatic setting are being translated to early BC, including adaptive trial designs. Antibody-drug conjugates (ADCs) hold potential in early BC; ongoing trials are evaluating various indications.
🧬 Liquid Biopsy & Biomarkers ctDNA and liquid biopsy show promise for minimal residual disease (MRD) detection and relapse risk stratification. Tumor-informed assays have higher sensitivity than tumor-agnostic panels. Circulating tumor cells (CTCs) are prognostic but less sensitive; CHIP mutations may confound results. Multiple trials are exploring ctDNA as a tool for guiding post-treatment strategies.
HER2+ Breast Cancer Trastuzumab remains a foundational therapy after 20 years. Duration of trastuzumab (6 vs. 12 months) continues to be debated; 12 months remains standard. Improved HER2 testing and classification helps tailor therapies, especially in HER2-low disease. De-escalation strategies (e.g., PET-adapted) are under study for selected patients. Residual disease post-neoadjuvant therapy moves toward T-DM1 or other combinations; new trials are ongoing.
Tailoring Treatment & De-Escalation Omitting radiotherapy (RT) or endocrine therapy (ET) in very low-risk patients is under investigation. Minimally invasive alternatives (e.g., cryoablation) are being evaluated to reduce surgical burden. Older patients need individualized decision making rather than age-based exclusion from therapy. Tools like ESMO Magnitude of Clinical Benefit Scale can help weigh benefits vs toxicity.
Surgery & Local Management Breast-conserving surgery (BCS) remains preferred when feasible; mastectomy does not guarantee survival benefit. Radiotherapy tailoring (partial, hypofractionation) reduces toxicity while maintaining control. Post-neoadjuvant surgery focuses on resection of residual disease; MRI radiomics and biopsies aid prediction. Reconstruction decisions must be individualized, involving patient preferences and RT considerations.
ER+ Disease Nuances Optimizing adjuvant therapy (ET, CDK4/6 inhibitors, genomic assays) depends on recurrence risk and biomarkers. Chemotherapy benefit varies by genomic risk scores and age—particularly in premenopausal women. Extended ET decisions benefit from clinical, genomic, and novel biomarkers like ctDNA. Invasive lobular carcinoma (ILC) and ER-low tumors need refined imaging and therapeutic stratification.
Artificial Intelligence (AI) Integration AI has potential to enhance: Biomarker discovery and response prediction Treatment planning and radiation delivery Target identification and clinical decision support Collaboration between AI developers and clinicians is essential for clinical implementation.
Imaging & Staging Updates PET-CT may be useful in higher-stage early BC; routine use in stage I remains limited. Breast MRI improves staging but increases interventions without clear outcome benefit; selective use recommended. Follow-up imaging remains guided by existing evidence; future strategies might integrate new technologies and ctDNA.
Hereditary BC & Prevention Germline mutations (BRCA1/2, PALB2, ATM, CHEK2) justify altered management and intensive screening. Risk-reducing surgeries lower incidence, though survival benefits require longer follow-up. Non-surgical options (e.g., intensified screening, risk-reducing medications) are important for many carriers.
Axillary Management Sentinel lymph node biopsy (SLNB) remains standard for clinically node-negative patients. Omission of upfront axillary surgery is considered in select scenarios with multidisciplinary input. Trials are evaluating safe approaches to avoid full axillary dissection post-neoadjuvant therapy.
Clinical Trials & Patient-Centered Design High-quality trials require real-world applicability, patient involvement, meaningful endpoints, and QoL measures. Trial design frameworks (e.g., SPIRIT, PRECIS-2) help balance explanatory vs pragmatic objectives.
Special Populations BC during pregnancy requires tailored imaging and therapy planning to optimize maternal and fetal safety. Young patients and those with reproductive concerns need individualized counseling and treatment adaptation.
Paper summary (Eur Arch Otorhinolaryngol, 2026) — “The impact of drains on surgical outcomes in thyroid surgery”
This is a meta-analysis of randomized controlled trials comparing drain vs no drain after adult thyroid surgery (search Jan 1995–Aug 2025). It included 10 RCTs (n=1,078) and assessed haematoma/seroma (primary) plus SSI, return-to-theatre, pain, and length of stay.
Key findings
No significant difference with drains for: Haematoma (p=0.15) Seroma (p=0.64) Return-to-theatre (p=0.22) Drains were associated with worse outcomes: Higher SSI (4.2% vs 0.5%, p=0.01) Longer LOS (≈ +1.2 days, p<0.0001) More pain (MD ≈ +2.2, p=0.001)
Conclusion of the authors: routine drains don’t reduce clinically important collections/bleeding outcomes and should be selective/patient-specific.
Additional high-yield evidence on the same question
Systematic reviews
2017 meta-analysis (14 studies, n=1,927): drains increased infection and length of stay, with no significant differences in haematoma/seroma or RLN palsy/hypoparathyroidism. Cochrane review: highlights the key limitation of drains—they can block with clot and do not replace meticulous haemostasis / re-exploration when bleeding occurs; overall evidence did not support routine use.
Randomized trials (examples)
2013 RCT (Uganda, n=68): no-drain group had shorter LOS and less pain, with no signal that drains prevented important complications. 2023 RCT (lobectomy + central neck dissection, n=104): no routine drain needed; no-drain group had shorter LOS and better comfort metrics.
Evidence-based recommendation (practical)
1) Default position
For uncomplicated thyroidectomy/hemithyroidectomy, the best available RCT/meta-analysis evidence supports NO routine drain because it does not reduce haematoma/seroma and does increase SSI, pain, and LOS.
2) When a drain may be reasonable (selective use)
Consider a drain selectively when you believe a drain will meaningfully manage expected ongoing output or permit monitoring in a high-risk scenario, e.g.:
Extensive dissection / large dead space (e.g., combined procedures, broad flap elevation) Significant intraoperative oozing despite optimization (coagulopathy, difficult hemostasis) Reoperative thyroid surgery Very large goiter/substernal component (case-dependent) Neck dissection / lateral compartment work (many surgeons drain these by default; note: classic drain trials often exclude lateral neck dissections)
(Even in these settings, it’s worth emphasizing: drains don’t “prevent” a dangerous post-thyroidectomy hematoma—rapid recognition and evacuation remain key, and drains may clot off.)
3) What to do instead of routine drains (high-impact steps)
Meticulous hemostasis + Valsalva before closure Layered closure / dead-space minimization Standardized post-op neck checks and early warning protocol (swelling, tightness, voice change, stridor) Clear hematoma pathway (immediate bedside opening vs OR depending on severity/resources)