The true prevalence of iatrogenic injury to the EBSLN during thyroid surgery remains difficult to quantify, largely due to underdiagnosis and variability in clinical presentation.
– The pathophysiology and anatomical risk stratification of EBSLN injury were elegantly described by Cernea et al. in 1992 [1]. In this landmark study, the variant in which the nerve crosses the superior thyroid pedicle below the plane of the upper pole apex—classified as Cernea type 2B—was identified as carrying a high risk of injury.
– Although this configuration was initially reported in approximately 14% of cadaveric dissections by the University of São Paulo group [1], later clinical series by Gianlorenzo Dionigi et al. demonstrated that this “high-risk” anatomy may be present in up to 54% of patients with large or bulky goiters [2], significantly increasing surgical complexity.
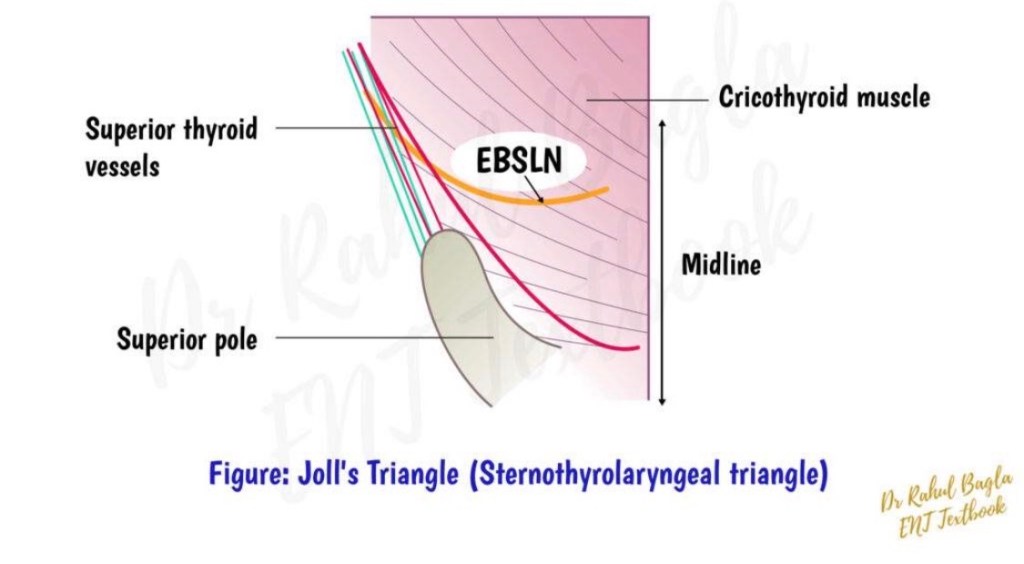
– First popularized by Mossman and DeWeese (1968), Joll’s sterno-thyro-laryngeal triangle remains a valuable anatomical landmark for identifying the EBSLN during superior pole dissection [3].
– In 1986, Michael Friedman provided a detailed description of the surgical approach to the upper thyroid pole that many of us continue to employ in complex cases, particularly when exposure of the EBSLN is critical [4].
– At the supero-external angle of the intermuscular pocket, created to identify the insertion of the sternothyroid muscle on the oblique line of the thyroid cartilage, surgeons frequently encounter a small arterial vessel. While its injury usually causes only minor (though often annoying) bleeding, it serves as an important anatomical landmark.
– These vessels supply the upper portion of the sternohyoid muscle, above the level of the cricoid cartilage.
– According to Wang et al. [5], in approximately 75% of cases, this vessel represents a terminal branch of a common trunk with the cricothyroid artery, originating from the superior thyroid artery. Before bifurcation, this trunk also gives rise to small nourishing branches to the thyrohyoid and omohyoid muscles.
– The so-called “sternohyoid nutrient vessel” is anatomically unique in 56% of cases [5]. After emerging superficially, it enters the (virtual) intermuscular space between the posterior surface of the sternohyoid and the anterior surface of the sternothyroid muscle, following one of two patterns:
✅ coursing along (“hugging”) the lateral border of the sternothyroid muscle, or ✅ directly piercing the most cranial fibers of the sternothyroid muscle.
– Awareness of this vascular anatomy can facilitate safe superior pole dissection, improve EBSLN identification, and ultimately reduce the risk of voice-related complications following thyroid surgery.
References
Cernea CR, et al. Identification of the external branch of the superior laryngeal nerve during thyroidectomy. Am J Surg. 1992. Dionigi G, et al. Surgical anatomy of the external branch of the superior laryngeal nerve. Gland Surg. Mossman HW, DeWeese MS. The surgical anatomy of the larynx. 1968. Friedman M. Surgical management of the superior thyroid pole. Otolaryngol Clin North Am. 1986. Wang C, et al. Vascular supply of the infrahyoid muscles and its surgical relevance. Surg Radiol Anat.
