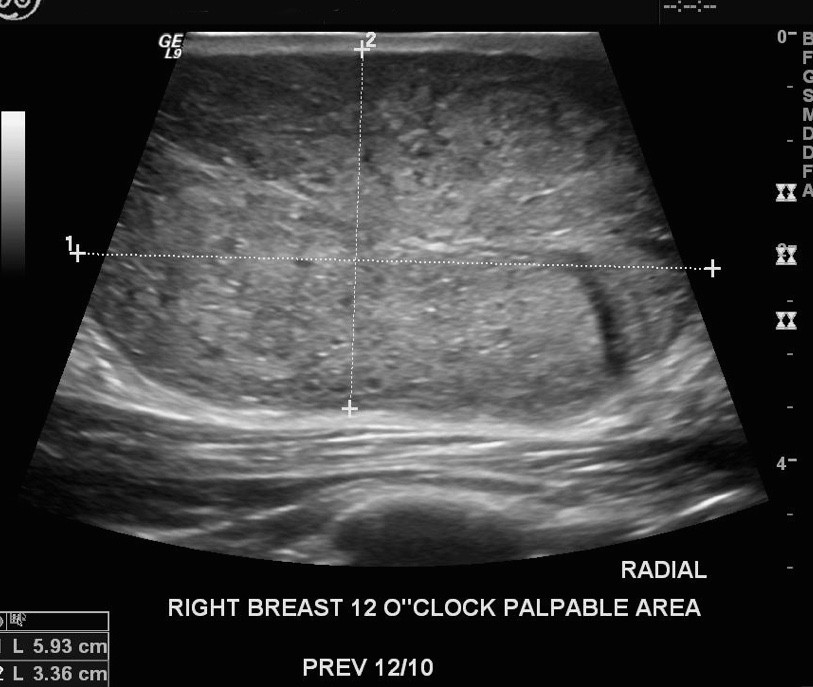
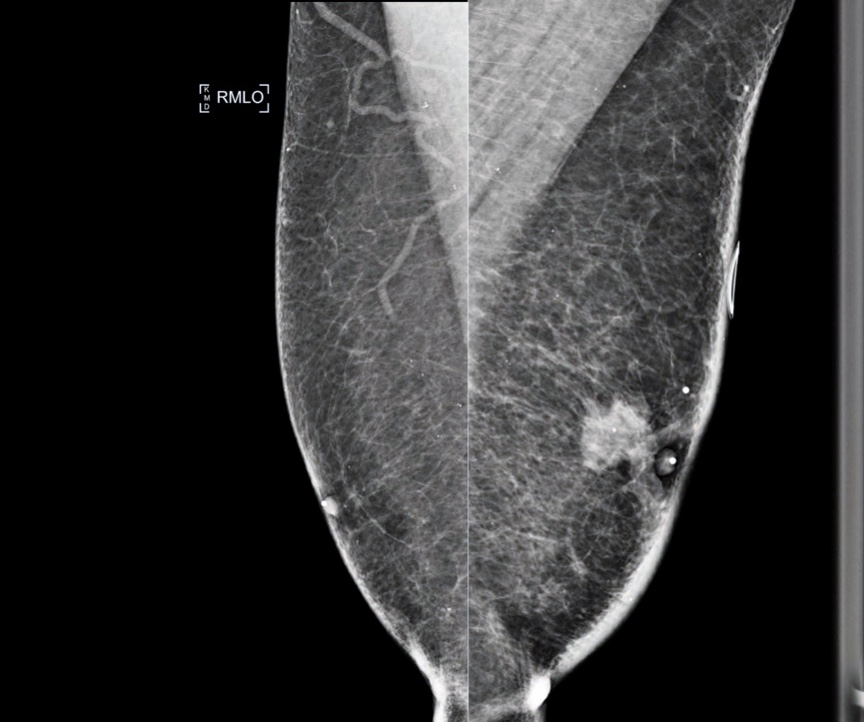
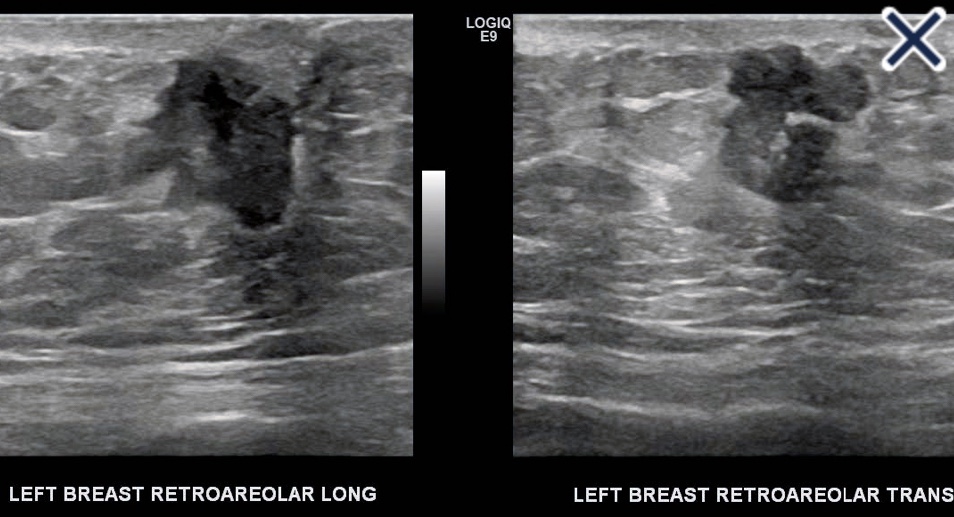
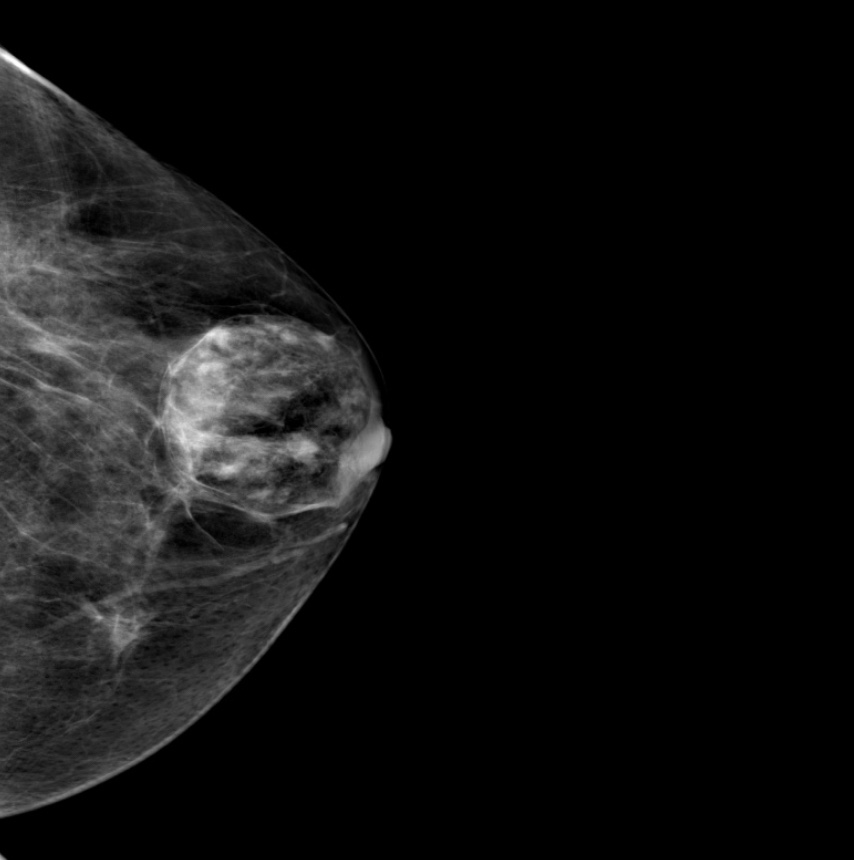
Palpable right subareolar massUltrasound from 6-month follow-upUltrasound from 6-month follow-up
The rapid growth of this lesion:
Suggests that it is a phyllodes tumor:
Although a giant fibroadenoma is another possibility
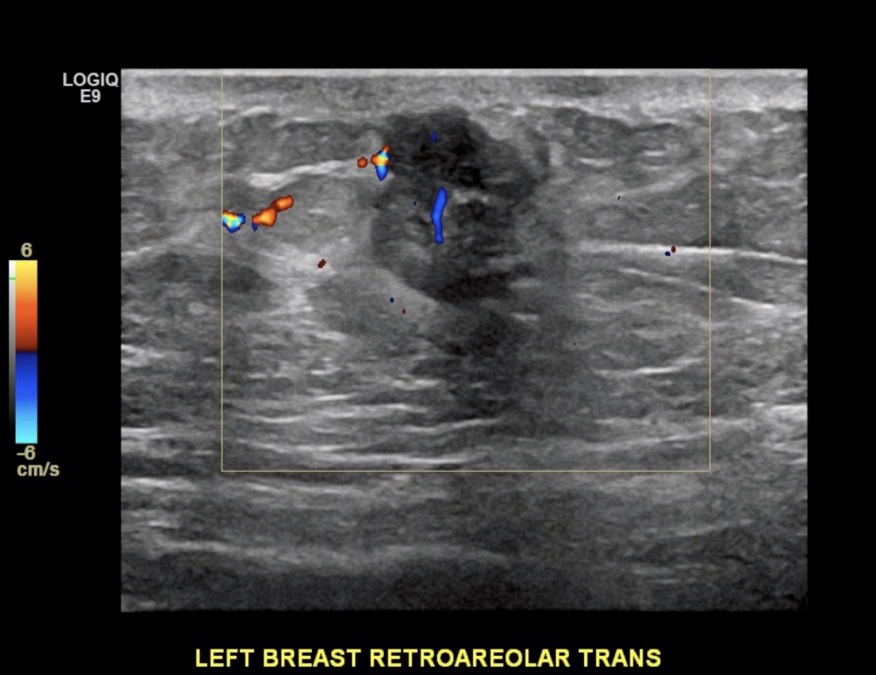
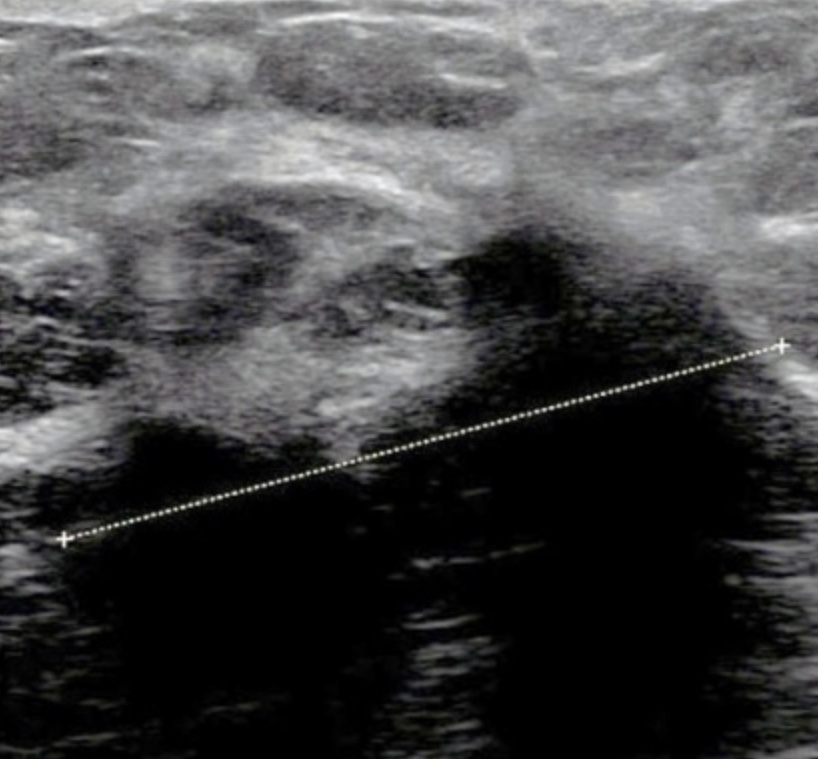
The most recent ultrasound image shows:
An isoechoic, heterogeneous mass that contains cystic, fluid filled spaces, and is vascular on Doppler examination
In most cases, benign phyllodes tumors:
Have margins that are well-circumscribed, and a thin, echogenic capsule is demonstrable
The doubling time for a:
Benign phyllodes tumor:
Is about four months
Malignant phyllodes tumor:
Is a little over a month
Rapidly growing phyllodes tumors:
Whether benign or malignant:
Often cause prominent veins on the skin:
From the developing vascularity
Phyllodes tumors are more common in women of Mexican descent:
Latin American women with phyllodes tumors tend to be diagnosed at an earlier age than other women
A malignant phyllodes tumor:
Would in all likelihood have a less distinct border than the lesion shown above
A core needle biopsy:
Cannot reliably distinguish phyllodes tumors from fibroadenomas:
It is therefore not sufficient for a definitive diagnosis
The correct management is excision:
With or without a pre-operative core biopsy:
With care to completely excise the tumor
Phyllodes tumors can also be difficult to distinguish from giant juvenile fibroadenomas:
But they should also be treated by surgical excision
The rapid growth of this lesion suggests a phyllodes tumor, not a fibroadenoma
References:
Guillot E, Couturaud B, Reyal F, Curnier A, Ravinet J, Lae M, et al. Management of phyllodes breast tumors. Breast J. 2011;17(2):129-137.
Plaza MJ, Swintelski C, Yaziji H, Torres-Salichs M, Esserman LE. Phyllodes tumor: review of key imaging characteristics. Breast Dis. 2015;35(2):79-86.
Rajan PB, Cranor ML, Rosen PP. Cystosarcoma phyllodes in adolescent girls and young women: a study of 45 patients. Am J Surg Pathol. 1998;22(1):64-69.
Sosin M, Pulcrano M, Feldman ED, Patel KM, Nahabedian MY, Weissler JM, et al. Giant juvenile fibroadenoma: a systematic review with diagnostic and treatment recommendations. Gland Surg. 2015;4(4):312-321.
Stavros AT. Atypical, high-risk, premalignant, and locally aggressive lesions. In: Stavros AT. Breast Ultrasound. Philadelphia, PA: Lippincott Williams & Wilkins; 2004:689-711.
The sonographic image for this patient shows a fairly round, well-circumscribed, microlobulated lesion with posterior enhancement
The most reliable sonographic feature of medullary carcinoma is:
Enhanced through transmission:
This results from the highly cellular lesion with a paucity of desmoplastic fibrous tissue, in addition to areas of cystic necrosis and hemorrhage
Medullary carcinomas:
Are classically well-circumscribed:
Though most of them have some area of angularity
High-grade, colloid (mucinous), and papillary carcinomas:
Typically have a sonographic appearance similar to medullary carcinoma:
The lesion in Image:
Is irregular, has spiculated margins, and shows posterior shadowing:
All of these features are commonly seen in fat necrosis, scar, and low-grade invasive cancers
Hematoma is unlikely to have enhanced through transmission
References:
Harvey JA. Unusual breast cancers: useful clues to expanding the differential diagnosis. Radiology. 2007;242(3):683-694.
Meyer JE, Amin E, Lindfors KK, Lipman JC, Stomper PC, Genest D. Medullary carcinoma of the breast: mammographic and US appearance. Radiology. 1989;170(1 Pt 1):79-82.
Stavros AT. Malignant solid breast nodules: specific types. In: Stavros AT. Breast Ultrasound. Philadelphia, PA: Lippincott Williams & Wilkins; 2004:297-688.
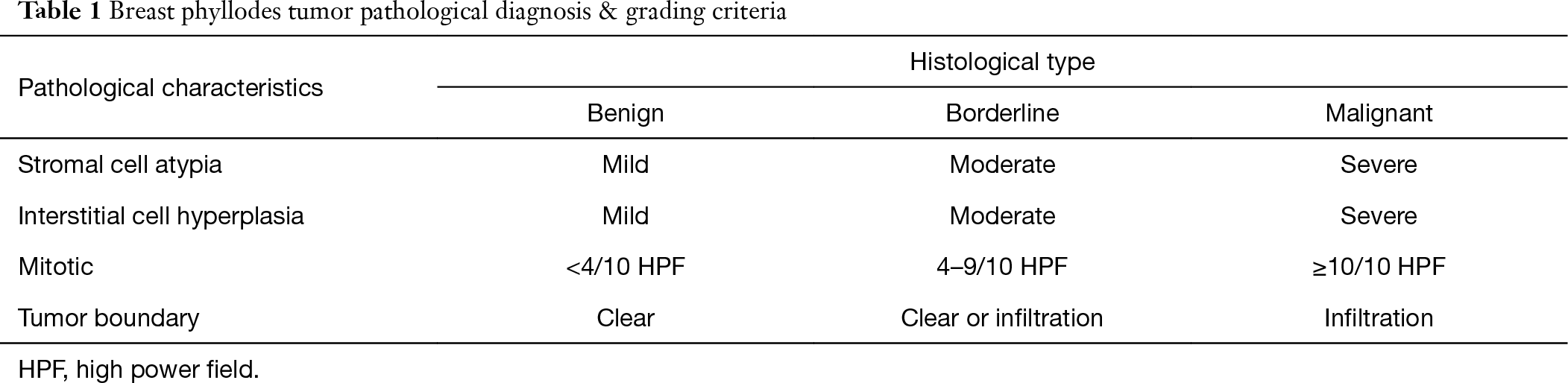
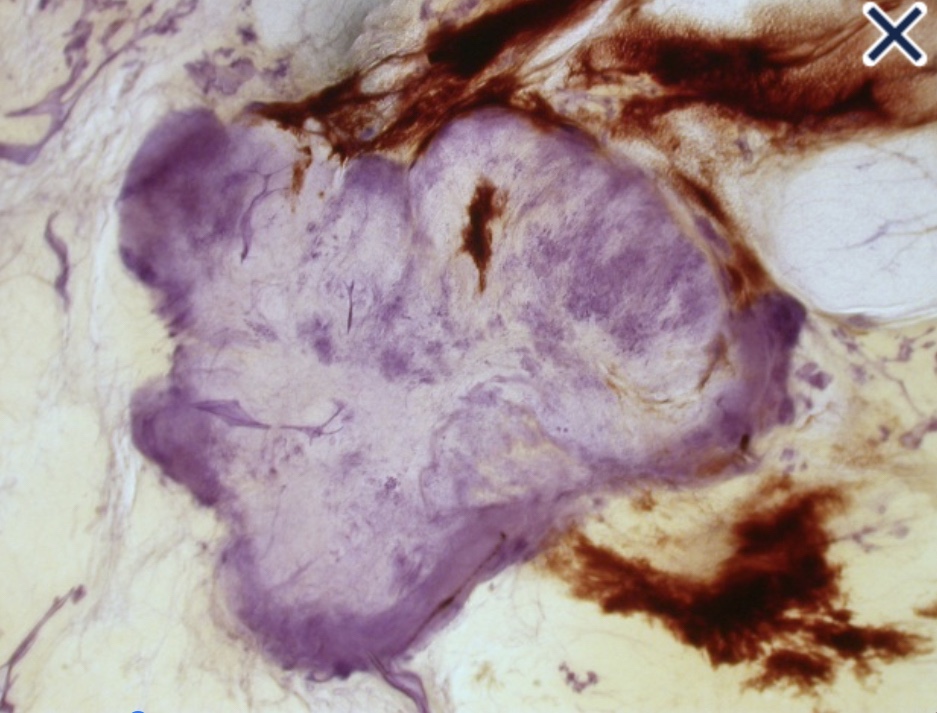
Phyllodes tumors:Are true fibroepithelial neoplasms:With both epithelial and stromal components
They represent less than 1% of all breast tumors:Most commonly occurring in women in their 50sThey are rapidly growing tumors:But are usually well-defined / circumscribed:Often appear as distinct masses:Indistinguishable from fibroadenomas on mammography and ultrasound
The World Health Organization has divided phyllodes tumors into three categories: BenignBorderline
Malignant
The majority of phyllodes tumors are benign:With local recurrence rates of 15% to 20% depending on adequacy of excision
Grading is usually based on multiple criteria in the stromal component:Nuclear pleomorphismMitotic rate
Stromal overgrowth
Cellularity
Tumor margins
The distinction between cellular fibroadenomas and phyllodes tumors:Can be difficult
The definition of “optimal” margin varies for various types of phyllodes tumors:Historically, margins of 2 cm to 3 cm have been recommended:But current recommendations are considerably less:With the only “absolute” being that the margin is tumor-free
Malignant transformation:Is a rare occurrence
Metastases can occur:In a small number of malignant phyllodes tumors and an even smaller number of borderline phyllodes tumors
Radiotherapy may be of benefit for local control of malignant phyllodes tumors
Differences in grading of phyllodes tumors among pathologists can be substantial
REFERENCES
Barth RJ Jr, Wells WA, Mitchell SE, et al. A prospective, multi-institutional study of adjuvant radiotherapy after resection of malignant phyllodes tumors. Ann Surg Oncol. 2009;16:2288-2294.
Lawton TJ, Acs G, Argani P, et al. Interobserver variability by pathologists in the distinction between cellular fibroadenomas and phyllodes tumors. Int J Surg Pathol. 2014;22:695-698.
O’Malley F, Pinder S, Mulligan A, eds.. Fibroepithelial lesions, including fibroadenoma and phyllodes tumors. In: Breast pathology: a volume in the series: foundations in diagnostic pathology, 2nd ed. Philadelphia, PA: Elsevier Saunders; 2011:121-138.
Sinn H, Kreipe H. A brief overview of the WHO classification of breast tumors, 4th edition, focusing on issues and updates from the 3rd edition. Breast Care (Basel). 2013;8:149-154.
Spitaleri G, Toesca A, Botteri E, et al. Breast phyllodes tumor: a review of literature and a single center retrospective series analysis. Crit Rev Oncol Hematol. 2013;88 :427-436.
👉Member of the American Society of Breast Surgeons:
Phyllodes tumors are classified into three groups:
Benign
Borderline
Malignant
Borderline and malignant phyllodes tumors:
Have a higher incidence of local recurrence:
Therefore, historically management was:
A mastectomy without nodal assessment
Recently, more patients are undergoing lumpectomy for this lesion
Researchers believe that local recurrence rates:
Are similar for borderline and malignant phyllodes tumors:
Historically:
1 cm margins have been recommended for malignant and borderline phyllodes tumors:
And continue to be recommended in the current 2023 NCCN guidelines
The guidelines however note that while narrow margins are associated with an increased risk for local recurrence:
They are not an absolute indication for mastectomy
Newer data may suggest a smaller margin is adequate:
Spanheimer et al:
Identified local recurrences in 16% of 71 patients with borderline or malignant phyllodes tumors undergoing:
Breast-conserving surgery
Some of these patients had a positive or close (< 1 mm) margin
When the subset of patients with a margin > 1 mm was considered:
The local recurrence rate was 12%
In addition, radiation may play a role in decreasing the risk of local recurrence:
In a prospective, multi-institutional study, 46 patients (30 with malignant phyllodes tumors and 16 with borderline phyllodes tumors) underwent margin-negative resections followed by radiation therapy:
Eight of these patients had margins < 2 mm
After 10 years of observation for all patients:
None had developed a local recurrence
In another study using data from the National Cancer Database, Gnerlich et al:
Showed that adjuvant radiation therapy decreased the risk of local recurrence after resection of phyllodes tumors by:
More than half (hazard ratio [HR] 0.43, 95% confidence interval [CI] 0.19–0.95).4
References
Tan, BY, Acs, G, Apple, SK, et al. Phyllodes tumor of the breast: a consensus review. Histopathology. 2016;68(1):5-21.
Spanheimer P, Murray M, Zabor E, et al. Long term outcomes after surgical treatment of malignant/borderline phyllodes tumors of the breast. Ann Surg Oncol. 2019;26(7):2136-2143.
Barth R, Wells W, Mitchell S, Cole B. A prospective, multi-institutional study of adjuvant radiation therapy after resection of malignant phyllodes tumors. Ann Surg Oncol. 2009;16(8):2288-2294.
Gnerlich J, Williams R, Yao K, Jaskowiak N, Kulkarni S. Utilization of radiotherapy for malignant phyllodes tumors: analysis of the National Cancer Database 1998–2009. Ann Surg Oncol. 2014;21(4):1222-1230
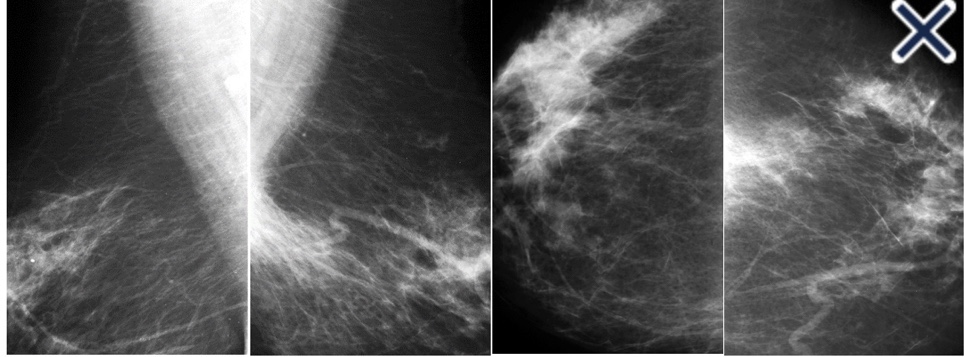
The mammogram shows a spiculated mass with extensive edema:
As evidenced by skin thickening and increased trabecular markings in the breast (Images)
Ultrasound shows a heterogeneous, irregular, hypoechoic mass with some angular and spiculated margins (Image):
Internal vascularity is demonstrated on Doppler examination (Image)
Gynecomastia:
Does not cause erythema, skin thickening, and breast edema:
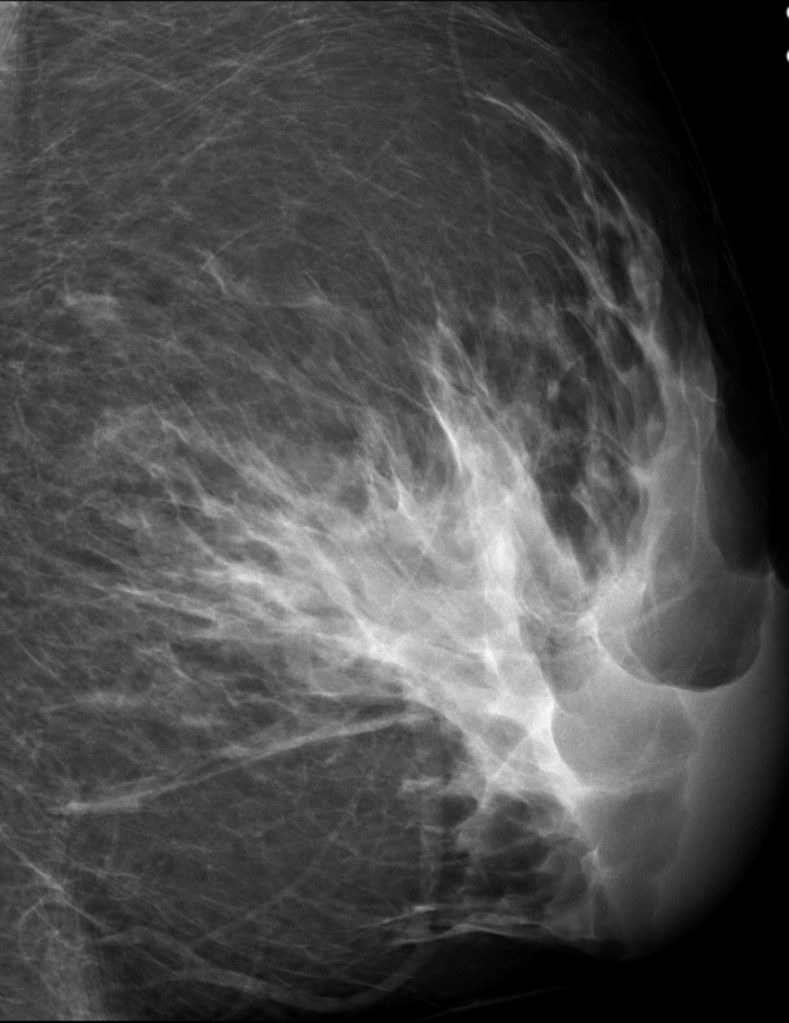
The mammogram would usually show a triangular shaped density radiating from the nipple into the breast tissue (Image)
Classic mammographic image of gynecomastia
The sides of the mammographic triangle in gynecomastia are:
Usually straight or concave (Image) as opposed to convex in breast cancer
The sonographic appearance of gynecomastia depends on the phase of development:
It can appear quite hypoechoic and have angular margin
Paget’s disease of the breast is rare, but it does occur in males:
It would present with a nipple rash and would not be expected to have secondary infection
There are usually no mammographic or sonographic features unless there is an underlying invasive carcinoma
References
Abeywardhana DY, Nascimento VC, Dissanayake D, Taylor D, Metcalf C, Saunders C, et al. Review of ultrasound appearance in inflammatory breast cancer: a pictorial essay. J Med Imaging Radiat Oncol. 2016;60(1):83-87.
Stavros AT. Evaluation of the male breast. In: Stavros AT. Breast Ultrasound. Philadelphia, PA: Lippincott Williams & Wilkins; 2004:712-741.
Khalkhali I, Cho J. Male breast cancer imaging. Breast J. 2015;21(3):217-218.
Ottini L, Palli D, Rizzo S, Ferico M, Bazan V, Russo A. Male breast cancer. Crit Rev Oncol Hematol. 2010;73(2):141-155.
Most likely result from an overgrowth of a portion of normal breast tissue, or from fibrous and glandular elements becoming incorporated into a lipomatous growth:
Thus, they are sometimes called a “breast within a breast”
They are also variously called:
Adenolipofibroma
Lipofibroadenoma
Adenolipofibroma
Fibroadenolipoma:
Because they contain fibrous, fatty, and epithelial tissues
They may present as palpable masses:
But are more commonly discovered on routine imaging
They are round, oval, or lobulated, and usually are well-circumscribed:
They have a mixture of water density and fatty elements and frequently have either a capsule or the appearance of a capsule resulting from surrounding compressed breast tissue
A mammographically classic hamartoma does not require further imaging:
Short interval follow-up, or biopsy
The presence of a breast hamartoma should prompt further questioning of the patient to be sure there is nothing to suggest she has multiple hamartoma syndrome (Cowden syndrome):
A rare disorder caused by a deleterious mutation in the phosphatase and tensin homolog (PTEN) gene:
Patients with this disorder have an increased head circumference, multiple trichilemmoma skin lesions, intestinal hamartomas, and an increased risk of cancer of the breast, thyroid, endometrium, and kidney
Genetic testing should be done if there is a personal or family history suggestive of the disorder
References
Crothers JG, Butler NF, Fortt RW, Gravelle IH. Fibroadenolipoma of the breast. Br J Radiol. 1985;58(687):191-202.
Daya D, Trus T, D’Souza TJ, Minuk T, Yemen B. Hamartoma of the breast, an underrecognized breast lesion. A clinicopathological and radiographic study of 25 cases. Am J Clin Pathol. 1995;103(6):685-689.
Murat, A, Ozdemir H, Yildirim H, Poyraz AK, Ozercan R. Hamartoma of the breast. Australas Radiol. 2007;51(Spec No.):B37-B39.
Schrager CA, Schneider D, Gruener AC, Tsou HC, Peacocke M. Clinical and pathological features of breast disease in Cowden’s syndrome: an underrecognized syndrome with an increased risk of breast cancer. Hum Pathol. 1998;29(1):47-53.
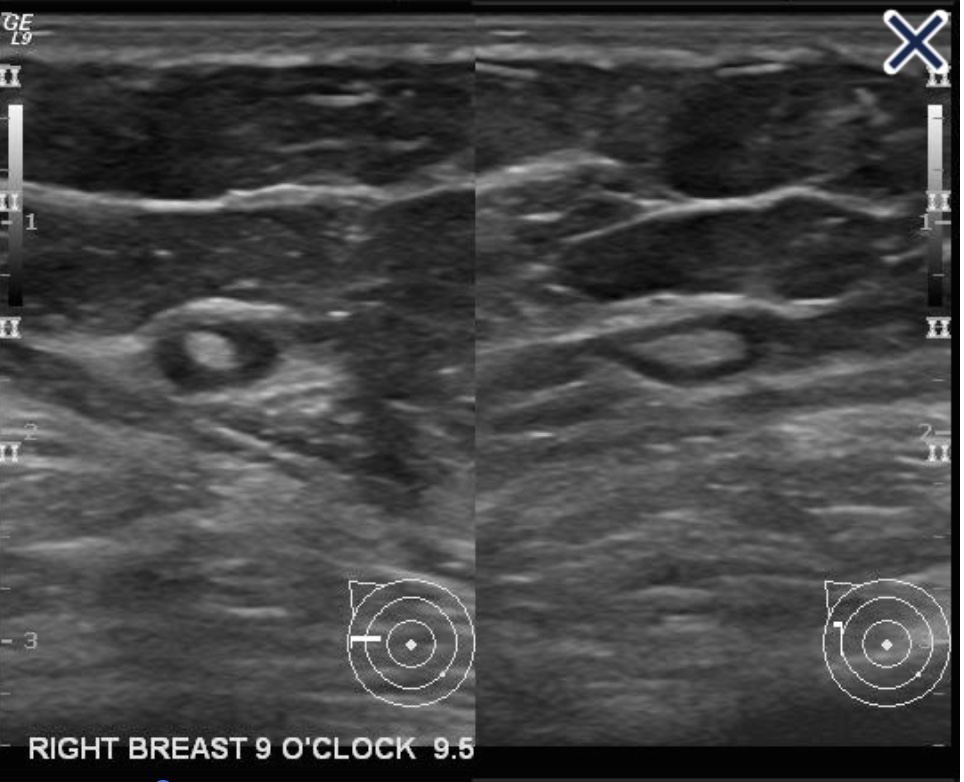
To be regarded as a simple cyst, a mass must meet three criteria:
The margins must be circumscribed:
i.e., a margin “that is well defined or sharp, with an abrupt transition between the lesion and surrounding tissue”
It must be anechoic:
i.e., “without internal echoes”
It must show posterior acoustical enhancement:
i.e., “a column that is more echogenic deep to the mass”
Simple cysts are almost never associated with cancer in the absence of other abnormalities seen on mammogram or ultrasound
There are numerous reflectors in breast tissue:
All of the sound waves that are reflected do not make it back to the transducer:
Many of them bounce back and forth (reverberate) between reflectors in the tissue, and with each reverberation, part of the echoes return to the transducer, are recorded, and part undergo another excursion between the reflectors
Most of these echoes are obscured by all of the other echoes in the tissue, but when an otherwise anechoic window (a cyst) is present:
The reverberation echoes can be seen in the anterior part of the cyst:
In the image shown, a hyperechoic band can be seen within or just above the anterior wall of the cyst, especially on the left side of the image
The acoustic mismatches between this band and the less echogenic tissue superficial to it and the anechoic fluid deep to it, cause echoes that reverberate, creating the artifact in the near field of the cyst
References
D’Orsi CJ, Sickles EA, Mendelson EB, Morris EA. ACR BI-RADS® Atlas: Breast Imaging Reporting and Data System, 5th ed. Reston, VA: American College of Radiology; 2013.
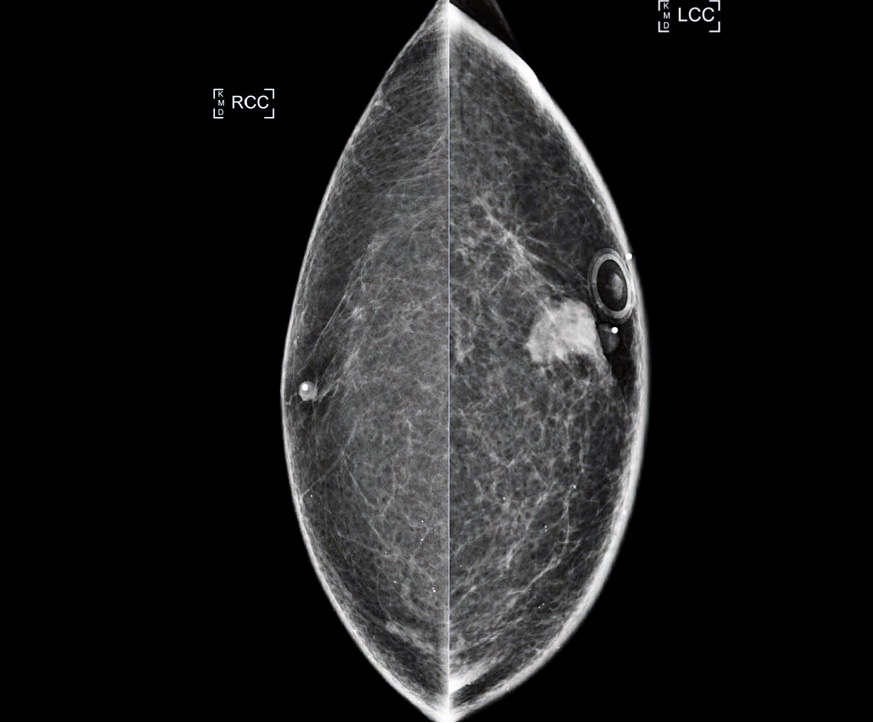
There are two main groups of diffuse breast cancers:
That present as large areas of architectural distortion on the mammogram:
One is neoductgenesis
The other is a diffusely infiltrating carcinoma:
Which makes up approximately
Bilateral diagnostic mammogram images
When the tumor is e-cadherin negative:
It is usually called invasive “lobular” carcinoma
When it is e-cadherin positive:
It is called infiltrating “ductal” carcinoma:
The designation based on e-cadherin staining is arbitrary:
Because the behavior of diffusely invasive carcinoma is the same regardless of the staining
Lacking calcifications and a central tumor mass:
These cancers are notoriously difficult to perceive on mammogram:
Even when they are large and palpable or when they occur in fatty involuted breasts:
However, the associated connective tissue response:
Makes this type of cancer quite visible with ultrasound
Hand-held ultrasound image
In contrast to diffusely infiltrating cancers:
Circular (Image) and spiculated (Image) tumors arising in the terminal ductal lobular units (TDLU):
Have bulging, convex contours protruding into the adipose tissue
Lobulated spherical tumor massMultifocal stellate invasive breast cancer
The solid variety of infiltrating lobular carcinoma:
Most probably arises within the TDLU and has a circular / oval shape on breast imaging
There are two other variants of invasive lobular carcinoma that arise in the TDLUs:
The tubulolobular variant:
Is either a unifocal or multifocal spiculated lesion on the mammogram (Image 5a-b)
The alveolar type of invasive lobular carcinoma:
Is usually mammographically occult, or it can be seen as a subtle, asymmetric density (Image)
Mammogram (a) and large format histology (b) alveolar type invasive lobular carcinoma
The various forms of invasive lobular carcinoma that develop in the TDLUs and present as localized lesions:
Have a significantly better prognosis than the diffusely infiltrating type breast cancer
Complex sclerosing lesions:
Present mammographically as nonpalpable architectural distortion with no central tumor mass and lucent radiating structures, the so called “black star”:
As opposed to cancers originating from the TDLU:
Which have a dense central tumor mass surrounded by radiopaque spiculation, giving the impression of looking at a “white star”
Malignant phyllodes tumors:
Present as large, high density masses:
The borders may be circumscribed or ill defined
Fat necrosis:
Also presents as a hypoechoic, high-density mass
References:
Tot T. Diffuse invasive breast carcinoma of no special type. Virchows Arch. 2016;468(2):199-206.
Tabár L, Dean PB. Teaching Atlas of Mammography. New York, NY: Thieme; 2011.