– The goals of treatment of cancer of the oral cavity are:
Cure of the cancer
Preservation or restoration of:
Speech, mastication, swallowing, and external appearance
Minimization of the sequelae of treatment such as:
Dental decay, osteonecrosis of the mandible, and trismus
Awareness of the risk of subsequent primary tumors and their management
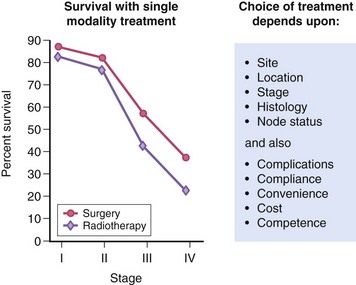
– Surgery and radiotherapy can be used as a single modality or in combination for the treatment of cancer of the oral cavity
– Treatment Approaches:
In general, early-stage (stage I or II) head and neck tumors:
May be treated using a single modality (surgery or radiotherapy):
Whereas advanced disease (stage III or IV) frequently benefits from multimodality therapy
The best therapeutic approach for the primary tumor depends on the anatomic site
Most neck disease can be treated equally well with surgery or radiation:
Thus the modality chosen to treat the neck is based on which modality is selected for the primary
When the primary tumor is treated with irradiation:
The regional lymphatics “at-risk” are incorporated into the treatment fields
Neck dissections should remain standardized (ie, complete anatomic dissections, as opposed to “berry picking” or random biopsy) in these settings to avoid incomplete surgery
Rodrigo ArrangoizSinai Medical Center in Miami, Florida:
He is first author on some publications on oral cavity cancer:
Oral Tongue Cancer: Literature Review and Current Management
Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon and is a member of the Braman Comprehensive Cancer at Mount Sinai Medical Center in Miami, Florida.
He is first author on some publications on oral cavity cancer:
Oral Tongue Cancer: Literature Review and Current Management
This nerve is a cutaneous branch of the intercostal nerves:
Most commonly the second intercostal nerve:
Which gives off a lateral cutaneous nerve:
Which continues as the intercostobrachial nerve
The intercostal nerves arise from the anterior rami of the thoracic spinal nerves
The intercostobrachial nerve pierces the serratus anterior:
Crosses the axilla to the medial side of the upper arm
The intercostobrachial nerve is commonly in the surgical field during axillary lymph node dissections:
It may be severed during surgery, or subject to traction or postsurgical inflammation:
Thus leading to intercostobrachial neuralgia
The larger intercostal nerves:
Can be preserved with meticulous dissection
Neuropathic symptoms:
May be limited to numbness or tingling:
But may also include a burning sensation
Techniques such as a regional nerve block have been described to alleviate symptoms in severe cases:
In a study of 200 patients who underwent axillary dissection:
76% had symptoms of intercostobrachial neuralgia postoperatively
Of these patients, 82% reported improvement or resolution of these symptoms within 1 year:
Reflecting the richness of the sensory nerve supply to the axilla and upper arm
The thoracodorsal nerve:
Is a branch of the posterior cord of the brachial plexus:
Supplies motor function to the latissimus dorsi
If injured:
Patients experience weakness with arm abduction, lateral flexion, and difficulty with activities such as climbing, swimming, and using the arms to pull the body up
The medial cord of the brachial plexus:
Gives rise to the medial pectoral nerve:
Which innervates both the pectoralis minor muscle and the pectoralis major muscle
The medial pectoral nerve typically pierces the pectoralis minor muscle:
But may wrap around the lateral aspect of the pectoralis minor before traveling on to innervate the distal pectoralis major muscle
The lateral cord of the brachial plexus:
Gives rise to the lateral pectoral nerve:
Which innervates the pectoralis major muscle
This nerve travels along the medial border of the pectoralis minor muscle, and then along the undersurface of the pectoralis major muscle along with the pectoral branch of the thoracoacromial artery to supply the proximal pectoralis major muscle
The medial pectoral nerve bundle:
Is often encountered during axillary dissection as it is located lateral to the lateral pectoral nerve
If either of these nerves is injured:
Pectoralis muscle atrophy can occur:
Which can present as a late complication of surgery:
With weakness of shoulder adduction, interior rotation, and flexion
The long thoracic nerve:
Typically arises from anterior rami of the cervical spinal nerve roots C5 to C7:
It courses along the chest wall and supplies the serratus anterior muscle
Injury to this nerve causes a winged scapula
References
Sclafani LM, Baron RH. Sentinel lymph node biopsy and axillary dissection: added morbidity of the arm, shoulder and chest wall after mastectomy and reconstruction. Cancer J. 2008;14(4):216-222.
Wisotzky EM, Saini V, Kao C. Ultrasound-guided intercostobrachial nerve block for intercostobrachial neuralgia in breast cancer patients: a case series. Prev Med Rep, 2016;8(3):273-277.
Roses DF, Brooks AD, Harris MN, Shapiro RL, Mitnick J. Complications of level I and II axillary dissection in the treatment of carcinoma of the breast. Ann Sur. 1999;230(2):194-201.
Porzionato A, Macchi V, Stecco C, Loukas M, Tubbs RS, De Caro R. Surgical anatomy of the pectoral nerves and the pectoral musculature. Clin Anat. 2012;25(5):559-575.
This nerve is a cutaneous branch of the intercostal nerves:
Most commonly the second intercostal nerve:
Which gives off a lateral cutaneous nerve:
Which continues as the intercostobrachial nerve
The intercostal nerves arise from:
The anterior rami of the thoracic spinal nerves
The intercostobrachial nerve pierces the serratus anterior:
Crosses the axilla to the medial side of the upper arm
The intercostobrachial nerve is commonly in the surgical field during axillary lymph node dissections and may be severed during surgery, or subject to traction or postsurgical inflammation:
Thus leading to intercostobrachial neuralgia
The larger intercostal nerves:
Can be preserved with meticulous dissection
Neuropathic symptoms:
May be limited to numbness or tingling:
But may also include a burning sensation
Techniques such as a regional nerve block:
Have been described to alleviate symptoms in severe cases
In a study of 200 patients who underwent axillary dissection:
76% had symptoms of intercostobrachial neuralgia postoperatively
Of these patients, 82% reported improvement or resolution of these symptoms within 1 year:
Reflecting the richness of the sensory nerve supply to the axilla and upper arm
The thoracodorsal nerve:
Is a branch of the posterior cord of the brachial plexus:
It supplies motor function to the latissimus dorsi
If injured, patients experience weakness with arm abduction, lateral flexion, and difficulty with activities such as climbing, swimming, and using the arms to pull the body up
The medial cord of the brachial plexus:
Gives rise to the medial pectoral nerve:
Which innervates both the pectoralis minor muscle and the pectoralis major muscle
The medial pectoral nerve typically pierces the pectoralis minor muscle:
But may wrap around the lateral aspect of the pectoralis minor before traveling on to innervate the distal pectoralis major muscle
The lateral cord of the brachial plexus:
Gives rise to the lateral pectoral nerve:
Which innervates the pectoralis major muscle
This nerve travels along the medial border of the pectoralis minor muscle:
Then along the undersurface of the pectoralis major muscle along with the pectoral branch of the thoracoacromial artery to supply the proximal pectoralis major muscle
The medial pectoral nerve bundle:
Is often encountered during axillary dissection as it is located lateral to the lateral pectoral nerve
If either of these nerves is injured:
Pectoralis muscle atrophy can occur:
Which can present as a late complication of surgery, with weakness of shoulder adduction, interior rotation, and flexion
The long thoracic nerve:
Typically arises from anterior rami of the cervical spinal nerve roots C5 to C7
It courses along the chest wall and supplies the serratus anterior muscle
Injury to this nerve causes a winged scapula
References:
Sclafani LM, Baron RH. Sentinel lymph node biopsy and axillary dissection: added morbidity of the arm, shoulder and chest wall after mastectomy and reconstruction. Cancer J. 2008;14(4):216-222.
Wisotzky EM, Saini V, Kao C. Ultrasound-guided intercostobrachial nerve block for intercostobrachial neuralgia in breast cancer patients: a case series. Prev Med Rep, 2016;8(3):273-277.
Roses DF, Brooks AD, Harris MN, Shapiro RL, Mitnick J. Complications of level I and II axillary dissection in the treatment of carcinoma of the breast. Ann Sur. 1999;230(2):194-201.
Porzionato A, Macchi V, Stecco C, Loukas M, Tubbs RS, De Caro R. Surgical anatomy of the pectoral nerves and the pectoral musculature. Clin Anat. 2012;25(5):559-575.
It is a surgical sub-specialty that deals mainly with benign and malignant tumors of the head and neck region, including:
The scalp, facial region, eyes, ears, nose, nasal fossae, paranasal sinuses, oral cavity, pharynx (nasopharynx, oropharynx, hypopharynx), larynx (supraglotic larynx, glottis larynx, subglotic larynx), thyroid gland, parathyroid gland, salivary glands (parotid glands, submandibular glands, sublingual glands, minor salivary glands), soft tissues of the neck, skin of the head and neck region.
The head and neck surgeon’s work area:
Does not cover tumors or diseases of the brain and other areas of the central nervous system or those of the cervical spine:
This is the neurosurgeon field
Among the diagnostic procedures performed by the head and neck surgeon, are the following:
Nasopharyngolaryngoscopy:
Performed to examine, evaluate and, possibly perform a biopsy, of oral cavity, pharyngeal and laryngeal lesions
The surgeries most commonly performed by the head and neck surgeon are:
Total or near total thyroidectomies
Hemithryoidectomies (lobectomies)
Comprehensive neck dissections
Selective neck dissections
Maxillectomies:
Total maxillectomy
Subtotal maxillectomy
Infrastructure maxillectomy
Suprastructure maxillectomy
Medial maxillectomy
Mandibulectomy:
Segmental
Marginal
Tracheostomy
Salivary gland surgeries:
Parotid gland operations:
Limited superficial parotidectomy with identification and preservation of the facial nerve
Superficial parotidectomy with identification and preservation of the facial nerve
Near total parotidectomy with identification and preservation of the facial nerve
Total parotidectomy
Submandibular gland resection
Sublingual gland resection
Resection of tumors of the oral cavity:
Glossectomy
Resection of the floor of the mouth tumors
Resection of tumors of the pharynx
Resection of tumors of the larynx
Split-thickness skin grafts
Full-thickness skin grafts
Sentinel lymph node mapping and sentinel lymph node biopsy
Resection of malignant skin tumors (BCC, SCC, melanoma) of the head and neck region
The training of the head and neck surgeon includes mastering the following subjects:
Surgical Anatomy
History and Basic Principles of Head and Neck Surgery
Epidemiology, Etiology, and Pathology of Head and Neck Diseases
Diagnostic Radiology of the Head and Neck Region
Tumors of the Scalp, Skin and Melanoma
Eyelids and Orbit
Nasal Cavity and Paranasal Sinuses
Skull Base and Temporal Bone
Lips and Oral Cavity
Pharynx and Esophagus
Larynx and Trachea
Cervical Lymph Nodes
Thyroid and Parathyroid Glands
Salivary Glands
Neurogenic Tumors and Paragangliomas
Soft Tissue Tumors
Bone Tumors and Odontogenic Lesions
Reconstructive Surgery
Oncologic Dentistry and Maxillofacial Prosthetics
Principles of Radiation Oncology
Principles of Chemotherapy
Molecular Oncology, Genomics and Immunology
Nutrition
Biostatistic
My name is Rodrigo Arrangoiz I am a board-certified surgical oncologist who sub-specializes in breast cancer and head and neck cancer. I earned his medical degree at the Anahuac University Medical School in Mexico City, Mexico and graduated Suma Cum Laude. I completed his internship and residency in general surgery at Michigan State University, where he was named chief resident during his fifth year of residency. I also completed a complex surgical oncology, head and neck fellowship at the Fox Chase Cancer Center in Philadelphia and at the same time he undertook a master’s in science (Clinical Research for Health Care Professionals) at Drexel University in Philadelphia. I participated in a two-year global online fellowship in head and neck surgery and oncology through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center.
I have participated in multiple courses and academic congresses as a lecturer and guest professor and has also participated in several publications on topics related to his specialty that include oral cavity cancer, hyperparathyroidism, thyroid cancer, breast cancer, endocrine tumors, squamous cell carcinoma of the head and neck, and more. I am board certified by the American Board of Surgery, the Mexican Board of General Surgery and the Mexican Board of Oncology.
I am a member of various medical associations such as the American College of Surgeons, American Thyroid Association, American Head and Neck Society, American Medical Association, American Society of Clinical Oncology, Association of Academic Surgeons, Society of Surgical Oncology, among others.
What You Need to Know About Head and Neck Cancer Treatments That Provide Life-Saving Results
By Dr. Rodrigo Arrangoiz, MS, MD, FACS, FSSO – Surgical Oncologist, Mount Sinai Medical Center
From the way we speak and eat to how we breathe and express emotions, the head and neck region plays a vital role in daily life. Unfortunately, this complex area is also susceptible to a variety of cancers that can dramatically affect a person’s health and quality of life. That’s why understanding head and neck cancers—their risk factors, symptoms, and treatment options—is critical for early detection and successful outcomes.
As a surgical oncologist specializing in head and neck and breast cancers at Mount Sinai Medical Center, I’ve seen firsthand how early diagnosis and expert care can be lifesaving. During Head and Neck Cancer Awareness Month, I want to share what patients and families should know.
What Is Head and Neck Cancer?
Head and neck cancer is not a single disease but a group of biologically similar cancers that begin in the squamous cells lining the mucosal surfaces inside the head and neck—such as the mouth, throat, and voice box. Cancers can also arise in the salivary glands, thyroid, sinuses, or skin of the face and scalp.
According to the National Cancer Institute, over 72,000 Americans will be diagnosed with a head and neck cancer in 2025 alone. These cases often involve complex anatomy and require a multidisciplinary approach to treatment.
Risk Factors You Should Know
Several risk factors are strongly linked to head and neck cancers:
Tobacco and alcohol use: These remain the leading causes, especially when combined. Human papillomavirus (HPV): HPV is now the leading cause of oropharyngeal cancers, particularly in younger, non-smoking patients. Sun exposure: Prolonged UV exposure increases the risk of skin cancers in the facial and scalp areas. Poor oral hygiene, poor nutrition, and exposure to certain industrial chemicals also contribute to overall risk.
Know the Signs—And Speak Up
Symptoms can be subtle. If you notice persistent hoarseness, difficulty swallowing, a lump in the neck, or an unusual growth in the mouth or throat, don’t delay—get evaluated by your primary care physician. You may be referred to a head and neck surgical oncologist for further testing.
Early detection makes a difference. Many head and neck cancers are curable when caught in the early stages.
The Role of Surgery in Head and Neck Cancer Treatment
As a surgical oncologist, my role involves diagnosing and surgically treating tumors in the head and neck region—both benign and malignant. Surgery can be curative, especially when paired with other therapies like radiation or chemotherapy.
Common conditions and procedures we manage include:
Thyroid and parathyroid surgery for cancer or overactivity Salivary gland tumor removal (parotid, submandibular) Lymph node dissections in the neck for cancer staging or treatment Mouth and throat tumor resections, sometimes involving the tongue or larynx Skin cancer excisions and facial reconstruction Advanced reconstructive surgery using microvascular techniques when necessary
Each patient receives a personalized plan based on the tumor type, location, stage, and overall health. At Mount Sinai’s Comprehensive Cancer Center, we combine advanced surgical techniques with cutting-edge diagnostics, targeted therapies, and compassionate, team-based care.
Expertise at Mount Sinai Medical Center
Mount Sinai’s Comprehensive Cancer Center is one of South Florida’s leading institutions for head and neck cancer care. We offer:
State-of-the-art imaging and biopsy services A multidisciplinary tumor board to tailor treatment plans Access to clinical trials and the latest medical advancements Reconstructive surgery expertise for functional and cosmetic outcomes Post-treatment rehabilitation, including speech and swallowing therapy
Our goal is to not only treat the cancer but also preserve quality of life—whether that’s helping a patient regain their voice, their smile, or their confidence.
About Dr. Rodrigo Arrangoiz
Dr. Rodrigo Arrangoiz is a board-certified surgical oncologist with specialized fellowship training in complex head and neck surgery and breast surgical oncology. He is a Fellow of the American College of Surgeons (FACS) and the Society of Surgical Oncology (FSSO). He completed his advanced training at some of the most prestigious cancer centers in the U.S. and currently practices at Mount Sinai Medical Center in Miami Beach, where he provides cutting-edge, compassionate cancer care.
To learn more about Mount Sinai’s Comprehensive Cancer Center, visit:
The breast extends from the lateral border of the sternum to the midaxillary line:
In some individuals, into the axilla itself
The adult breast consists of:
Glandular and adipose tissue:
Together with a system of connecting ligaments
1. Nipple:
This is located at the apex of the breast and projects up to 1 cm
Optimizing its positioning is of utmost importance in breast surgery
In the average adult female the nipples lie in the midclavicular line:
19 cm to 21 cm from the sternal notch and 9 cm to 11 cm from the midline:
But their position varies widely according to shape, size and age
2. Areola:
This is a circular area of skin that surrounds the nipple
Its color darkens during pregnancy due to the deposition of melanin
The areolar skin contains Montgomery glands:
Which secrete a protective oily lubricant
3. Glandular tissue:
The glandular tissue is the functional component of the lactating breast and the site of milk production, which is passed to the nipple via a system of ducts:
Each breast, or mammary gland:
Contains 15 to 20 lobes and each lobe is comprised of 20 to 40 terminal ductal lobular units (TDLU):
The TDLU is the functional unit of the breast
The breast mound is roughly hemispherical
The bulk of the glandular tissue is found in the upper outer quadrant:
Which is the commonest site of malignancy.
4. Adipose tissue:
This forms up to 70% of the breast mass:
It is the main determinant of breast size
5. Ligaments:
The structure and shape of the breast is maintained by fascial and ligamentous supports:
As first described by Sir Astley Cooper in 1840
Superficial fascial system:
The breast is enveloped by the superficial and deep laminae of the superficial fascia:
The superficial lamina is separated from the dermis by a thin layer of fatty tissue:
But is often difficult to identify as a separate entity
Suspensory ligaments of Cooper:
These fibrous strands extend through the breast parenchyma between the layers of the superficial and deep (pre-pectoral) fascia:
They help to maintain a non-ptotic breast shape
6. Axillary tail (of Spence):
There is a variable extension along the inferior edge of pectoralis major towards the axilla
This usually lies within the subcutaneous fat but may penetrate the axillary fascia to lie adjacent to the lymph nodes
Occasionally it is a separate entity with ducts that do not drain to the nipple.
7. Retromammary space:
In reality this is not a space but a plane of loose connective tissue lying between the deep lamina of the superficial fascia and the deep pre-pectoral fascia
Chassaignac bursa (also known as the retromammary bursa, submammary serous bursa or occasionally Chassaignac bag):
Is the space behind the breast, lying between the pectoralis fascia posteriorly and deep layer of superficial fascia anteriorly
This is the plane of dissection in which a subglandular pocket can be created for insertion of a prosthesis for breast augmentation
8. Muscle:
The medial two-thirds of the base of the breast lie over the pectoralis major muscle
The lateral one-third lies over serratus anterior and a small portion of the rectus abdominis and external oblique muscles
The muscles are separated from the breast by the deep fascia
9. Rib cage:
Deformities of the ribs, including those that are secondary to a spinal deformity can lead to an apparent asymmetry of breast position and/or shape
Vascular Supply of the breast:
The breast has a rich blood supply:
Which permits safe division and excision of breast tissue:
The viability of the nipple areolar complex is dependent on vessels that pass through the gland:
Which must therefore be preserved
There are three main arterial systems:
Internal Thoracic (Mammary) Artery:
Is responsible for roughly 60% of the vascular supply to the breast
Arising directly from the subclavian artery, the internal thoracic artery passes posterior to the subclavian vein and runs along the edge of the sternum, deep to the costal cartilages
Perforating branches of the internal thoracic artery pass through the 2nd to 6th intercostal spaces to supply the medial half of the breast:
The 2nd and 3rd perforators are the predominant vessels and these are preferred for anastomosis when reconstructing the breast with a free tissue transfer
Lateral Thoracic Artery:
A branch of the second portion of the axillary artery:
Supplies the upper outer quadrant of the breast
The lateral thoracic artery runs along the lower border of the pectoralis minor muscle and curls around the lateral border of pectoralis major to enter the breast
Other branches of the lateral thoracic artery perforate pectoralis major to supply the overlying breast tissue
Posterior Intercostal Arteries:
The lateral branch of the posterior intercostal arteries divides into posterior and anterior branches
The anterior branches from the 3rd to 6th intercostal spaces supply the lateral portion of the breast and the overlying skin through their mammary branches
Other Supply:
The axillary artery also provides other branches to the breast, including the:
Superior thoracic artery:
A branch from the first part of the axillary artery)
The pectoral branch of the thoracoacromial artery and the subscapular artery
The venous drainage of the breast is via two venous systems:
Superficial system:
Which lies within the subdermal venous plexus:
The pattern of drainage is highly variable
Deep system:
The deep venous system parallels the arterial supply:
The medial half of the breast drains via veins that accompany the perforating branches of the internal mammary artery through the intercostal spaces, back to the internal mammary vein
The lateral thoracic veins drain into the axillary vein
The posterior intercostal veins drain into the azygous vein on the right and the hemiazygous vein on the left
Innervation of the breast:
The nerve supply to the breast consists of sensory fibres from the skin and sympathetic efferent fibres to the blood vessels, glandular tissue and smooth muscle cells in the skin and nipple
The sensory nerve supply is derived from cutaneous branches of the intercostal nerves:
Medially:
Anterior branches of the 1st to 6th intercostal nerves
Laterally:
Lateral branches of the 2nd to 6th intercostal nerves
Nipple areola complex:
Supplied by the anterior branch of the 4th intercostal nerve
There is an extensive nerve plexus within the nipple
The skin of the nipple areola complex contains free nerve endings, Meissner’s corpuscles and Merkel disc endings