- BRCA 1 and BRCA 2 are genes:
- That produce tumor suppressor proteins:
- Which help repair damaged DNA
- They are the most common gene alterations seen in the hereditary breast cancer population
- They are associated with an increased risk of breast cancer estimated to be:
- 55% to 70% for BRCA 1 carriers by age 70
- 45% to 70% in BRCA 2 carriers by age 70
- While both BRCA 1 and BRCA 2 mutations are associated with an increased risk of breast cancer:
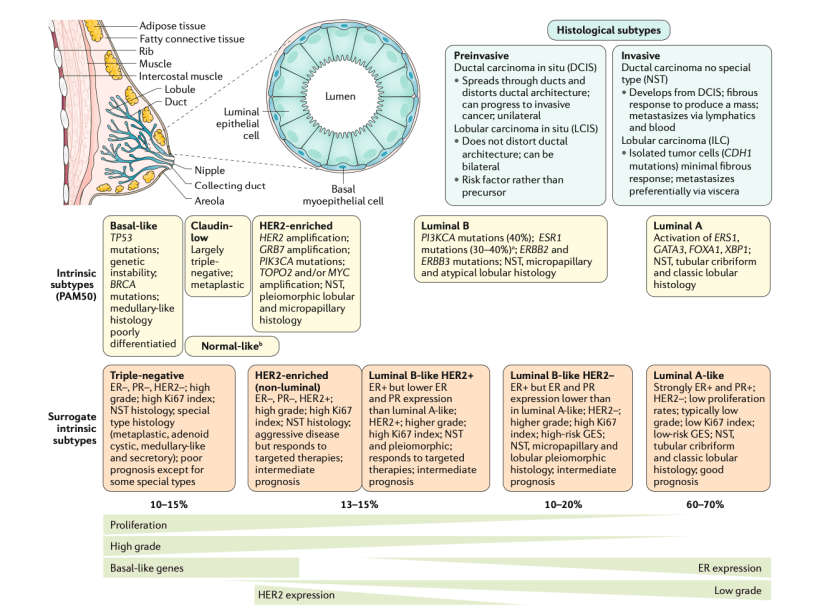
- BRCA 1 breast cancers more commonly occur in:
- Younger
- Premenopausal women
- Are more likely to be triple negative
- BRCA 1 breast cancers more commonly occur in:
- BRCA 1 is associated with a higher risk of ovarian cancer compared to BRCA 2:
- With a lifetime risk of 40% to 45% in BRCA 1 carriers compared to 15% to 20% in BRCA 2 carriers
- BRCA 2 breast cancers more closely resemble the sporadic breast cancer pattern:
- With a predominance of hormone receptor positive cancers in women greater than 50 years
- That produce tumor suppressor proteins:
- CHEK 2 and PALB 2 are moderate penetrance genes:
- That are less common than BRCA mutations
- Similar to BRCA 2 deleterious mutations:
- CHEK 2 and PALB 2 mutations are associated with:
- Hormone receptor positive postmenopausal breast cancer
- CHEK 2 and PALB 2 mutations are associated with:
- Imaging surveillance for BRCA mutation carriers begins at:
- Age 25 with annual breast MRI with contrast, with addition of mammography after age 30
- Although use of screening ultrasound is evolving in women with dense breast tissue:
- Its use in BRCA carriers has not been defined
- Surveillance strategies have significantly improved early detection but do not prevent breast cancer
- Bilateral salpingo-oophorectomy:
- Has been shown to provide approximately 50% relative reduction in breast cancer risk:
- But ultimately prophylactic mastectomy provides the greatest reduction
- Has been shown to provide approximately 50% relative reduction in breast cancer risk:
- The optimal timing of surgery depends on multiple factors, including:
- The patient’s desire for future breastfeeding
- Ages of family members at diagnosis
- Several retrospective series and meta-analyses of four prospective studies:
- Have supported prophylactic mastectomy in BRCA mutation carriers
- While the data demonstrate a 93% relative risk reduction in breast cancers:
- They do not demonstrate a survival benefit in this population
- Recent non-randomized studies have evaluated use of nipple-sparing mastectomy (NSM) and demonstrated its feasibility and safety in patients with BRCA mutation:
- Jakub et al. reported data from 548 risk-reducing NSMs in 346 patients treated at 9 institutions
- This study included both women opting for prophylactic mastectomies concurrent with treatment for a contralateral breast cancer, and women undergoing bilateral prophylactic mastectomies for risk reduction
- With median and mean follow up of 34 and 56 months, respectively:
- No ipsilateral breast cancers occurred after prophylactic NSM
- Breast cancer did not develop in any patients undergoing bilateral risk-reducing NSMs
- References
- Heemskerk-Gerritsen BA, Menke-Pluijmers MB, Jager A, et al. Substantial breast cancer risk reduction and potential survival benefit after bilateral mastectomy when compared with surveillance in healthy BRCA1 and BRCA2 mutation carriers: a prospective analysis. Ann Oncol. 2013;24(8):2029-2035.
- Genetic/familial high-risk assessment: breast and ovarian. National Comprehensive Cancer Network. Version 2.2019. https://www.nccn.org/professionals/physician_gls/pdf/genetics_screening.pdf. Accessed September 16, 2018.
- De Felice F, Marchetti C, Musella A, et al. Bilateral risk-reduction mastectomy in BRCA1 and BRCA2 mutation carriers: a meta-analysis. Ann Surg Oncol. 2015;22(9):2876-2880.
- Ludwig KK, Neuner J, Butler A. Risk reduction and survival benefit of prophylactic surgery in BRCA mutation carriers: a systematic review. Am J Surg. 2016;212(4):660-669
- Jakub JW, Peled AW, Gray RJ. Oncologic Safety of Prophylactic Nipple-Sparing Mastectomy in a Population With BRCA Mutations: A Multi-institutional Study. JAMA Surg. 2018;153:123-129.
- Loi M, Desideri I, Olmetto E, Francolini G, Greto D, Bonomo P, et al. BRCA mutation in breast cancer patients: Prognostic impact and implications on clinical management. Breast J. 2018;24(6):1019-1023.
- Peshkin BN, Isaacs, C et al. Overview of hereditary breast and ovarian cancer syndromes. UpToDate website. Updated February 10, 2020. https://www.uptodate.com/contents/genetic-testing-and-management-of-individuals-at-risk-of-hereditary-breast-and-ovarian-cancer-syndromes. Accessed February 15, 2020.
- Economopoulou P, Dimitriadis G, Psyrri A. Beyond BRCA: new hereditary breast cancer susceptibility genes. Cancer Treat Rev. 2015;41(1):1-8.
#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOncologist #BreastCancer #BRCA #CASO #CenterforAdvancedSurgicalOncology #Miami