- Synchronous and metachronous bilateral breast cancers:
- Appear in 1% to 20% of patients with breast cancer
- Improvements in screening and the increased use of MRI:
- Often diagnose more early-stage synchronous bilateral cancer
- The role of MRI in the preoperative planning:
- Is controversial and may be partly responsible for increasing mastectomy rates in the United States
- MRI may identify additional lesions in both the ipsilateral and contralateral breast in many women diagnosed with unifocal breast cancer:
- Many of these additional lesions are often found to be benign once additional diagnostic imaging is performed and biopsies are completed
- Additional MRI findings should not prompt surgeons to recommend mastectomy:
- Unless they are biopsy-proven to represent additional sites of malignancy not amenable to breast conservation, and/or the patient was inclined toward mastectomy prior to MRI findings
- Retrospective studies evaluating the outcomes of synchronous bilateral breast cancer:
- Are limited by small cohort sizes, differing definitions, and non-matched unilateral patients as controls
- Most retrospective studies show no differences in local recurrence or survival for bilateral breast cancers:
- Making bilateral breast-conserving treatment a safe option for early-stage synchronous cancers
- References
- Heron DE, Komarnicky LT, Hyslop T, Schwartz GF, Mansfield CM. Bilateral breast carcinoma: risk factors and outcomes for patients with synchronous and metachronous disease. Cancer. 2000;88(12):2739-2750.
- Intra M, Rotmensz N, Viale G, et al. Clinicopathologic characteristics of 143 patients with synchronous bilateral invasive breast carcinomas treated in a single institution. Cancer. 2004;101(5):905-912.
Blog
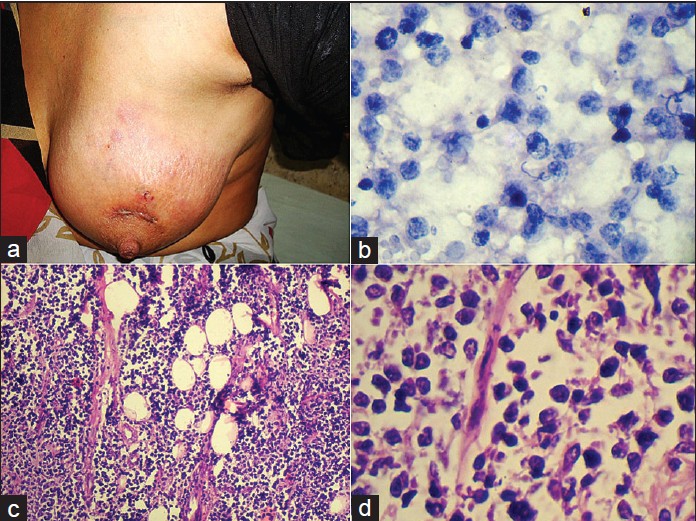
Primary Lymphoma of the Breast
- Current management strategies for primary breast lymphoma are largely based on:
- Results published in small, single-institution series
- Historically, primary breast lymphoma was treated with:
- Modified radical mastectomy with or without adjuvant chemotherapy or radiotherapy:
- Treatment strategies had focused on anthracycline-based chemotherapy with or without consolidative radiotherapy
- Modified radical mastectomy with or without adjuvant chemotherapy or radiotherapy:
- Current treatment guidelines dictate:
- That surgery should be reserved for
- Obtaining adequate tissue for diagnosis, if needed, and:
- Should not be regarded as a therapeutic modality in the treatment of this disease:
- In several series, surgery has been associated with worse outcomes
- Should not be regarded as a therapeutic modality in the treatment of this disease:
- Some histologies may be amenable to localized surgery so understanding the disease pathology is important in decision making
- While axillary nodal status is an important prognosticator:
- There are no definitive guidelines regarding how to stage the axilla:
- In addition to CT scan, axillary ultrasound with percutaneous biopsy is frequently used
- There are no definitive guidelines regarding how to stage the axilla:
- Sentinel lymph node biopsy has not been studied in this malignancy and currently has no role in its workup
- Obtaining adequate tissue for diagnosis, if needed, and:
- That surgery should be reserved for
- References
- Aviles A, Delgado S, Nambo MJ, Neri N, Murillo E, Cleto S. Primary breast lymphoma: results of a controlled clinical trial. Oncology. 2005;69(3):256-260.
- Aviv A, Tadmor T, Polliack A. Primary diffuse large B-cell lymphoma of the breast: looking at pathogenesis, clinical issues and therapeutic options. Ann Oncol. 2013;24(9):2236-2244.
- el-Ghazawy IM, Singletary SE. Surgical management of primary lymphoma of the breast. Ann Surg. 1991;214(6):724-726.
- Jennings WC, Baker RS, Murray SS, et al. Primary breast lymphoma: the role of mastectomy and the importance of lymph node status. Ann Surg. 2007;245(5):784-789.
#Arrangoiz #BreastSurgeon #CancerSurgeon #BreastCancer #BreastLymphoma #PrimaryLymphomaoftheBreast #CASO #Miami #CenterforAdvancedSurgicalOncology
Metaplastic Carcinoma of the Breast
- Metaplastic carcinoma of the breast:
- Tends to present in patients age 60 years and older
- Is rare in young or premenopausal women
- Compared to IDC:
- It has been shown to present in a higher proportion of African Americans and Hispanics
- Tends to present in patients age 60 years and older
- Metaplastic breast cancer (MBC):
- Is more likely to be high grade but axillary node negative at presentation
- The mean tumor size:
- Is about 4 cm
- Patients with this diagnosis are also more likely to receive chemotherapy and undergo mastectomy
- Recurrence tends to be locoregional or pulmonary:
- And is associated with a high mortality rate
- Future directions may include immunotherapies:
- As MBC has a unique histology, demonstrating increased PDL-1:
- Which may make it a good candidate for targeted therapy:
- More research is needed on this unique tumor phenotype
- Which may make it a good candidate for targeted therapy:
- As MBC has a unique histology, demonstrating increased PDL-1:
- References
- Pezzi CM, Patel-Parekh L, Cole K, Frank J, Klimberg VS, Bland K. Characteristics and treatment of metaplastic breast cancer: analysis of 892 cases from the National Cancer Data Base. Ann Surg Oncol. 2006;14(1):166-173.
- Schwartz T, Mogal H, Papageorgiou C, Veerapong J, Hsueh EC. Metaplastic breast cancer: histologic characteristics, prognostic factors and systemic treatment strategies. Exp Hematol Oncol. 2013;(1)2:31.
- Haque W, Teh BS. Current practice and future directions for metaplastic breast cancer. Ann Surg Oncol. 2018;25(Suppl 3):630-631.

#Arrangoiz #BreastSurgeon #BreastCancer #MetaplasticBreastCancer #SurgicalOncology #CancerSurgeon #Miami #CASO #CenterforAdvancedSurgicalOncology
Radioactive Iodine Therapy Pre-Therapy Diet
👉Prior to RAI, a low iodine diet (< 50 mcg/day) is recommended for 2 weeks prior to treatment to increase the efficacy.
#Arrangoiz #ThyroidSurgeon #CASO #CenterforAdvancedSurgicalOncology #ThyroidLobectomy #ThyroidCancer #ThyroidNodules #HeadandNeckSurgeon #EndocrineSurgery
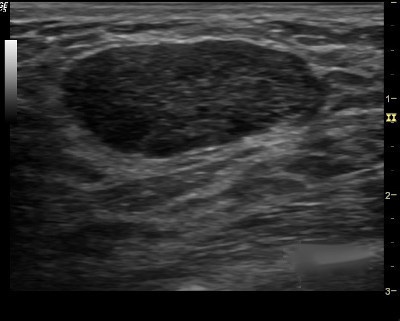
Evaluation of a Breast Nodule by Ultrasound
- You first evaluate the lesion for any of the 10 malignant signs:
- Shadowing
- Hypoechoic echotexture
- Spiculation
- Angular margins
- Thick echogenic capsule
- Taller than wider
- Microlobulation
- Duct extension
- Branching pattern
- Calcifications
2. Finding none, you move on to the second step in the evaluation process and specifically look for one of the three strictly defined benign signs, and if any of them is found, the lesion can be considered BI-RADS 3.
3. The three benign findings defined by Stavros are:
- A purely hyperechoic lesion with no hypoechoic area larger than a normal duct or lobule.
- Elliptical, wider than tall, well-circumscribed and thin echogenic capsule.
- Gently lobulated, wider than tall, well-circumscribed and thin echogenic capsule.
– Combining the elliptical or gently lobulated shapes with the presence of a complete, thin echogenic capsule is necessary because many circumscribed carcinomas and most ductal carcinoma in situ are encompassed in a thin, echogenic capsule.

👉Rodrigo Arrangoiz MS, MD, FACS cirujano oncology y cirujano de mamá de Center for Advanced Surgical Oncology:
-
Es experto en el manejo del cáncer de mama.

👉Es miembro de la American Society of Breast Surgeons:
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016


#Arrangoiz
#Surgeon
#Cirujano
#SurgicalOncologist
#CirujanoOncologo
#BreastSurgeon
#CirujanodeMama
#CancerSurgeon
#CirujanodeCancer
Thyroid Supplementation after Thyroid Surgery
👉After removal of the entire thyroid for cancer, patients require lifelong thyroid hormone replacement with levothyroxine starting immediately.
👉TSH levels are checked in approximately 6 to 8 weeks to titrate the dose.
#Arrangoiz #ThyroidSurgeon #CASO #CenterforAdvancedSurgicalOncology #ThyroidLobectomy #ThyroidCancer #ThyroidNodules #HeadandNeckSurgeon #EndocrineSurgery
Hormone Replacement after Thyroid Lobectomy
👉Most patients do not require lifelong hormone replacement after removal of half of the thyroid, however 30% to 50% of patients will.
#Arrangoiz #ThyroidSurgeon #CASO #CenterforAdvancedSurgicalOncology #ThyroidLobectomy #ThyroidCancer #ThyroidNodules #HeadandNeckSurgeon #EndocrineSurgery
Occult Primary Breast Cancer
- Three important conclusions are agreed upon regarding this clinical entity:
- Prognosis of occult primary breast cancer is the same or slightly better than women with classic stage IIA disease (T0, N1, M0)
- An exhaustive workup for the non-breast primary is usually not fruitful
- Treatment of the breast in some manner decreases the risk of local failure over time
- Occult primary breast cancer was first recognized by William Halsted:
- Who described three patients presenting with axillary tumors that were eventually found to represent breast cancer
- In modern series:
- Occult breast cancer accounts for 0.1% to 0.8% of all newly diagnosed breast cancers:
- The incidence has not decreased with improvements in breast imaging
- Differential diagnosis:
- In general:
- Palpable axillary nodes are more often related to benign rather than malignant disorders:
- However, when cancer is identified:
- The most common tumor causing axillary lymphadenopathy is:
- Breast cancer
- The most common tumor causing axillary lymphadenopathy is:
- However, when cancer is identified:
- Palpable axillary nodes are more often related to benign rather than malignant disorders:
- In several series:
- The incidence of breast cancer in mixed populations of men and women with metastatic axillary adenopathy:
- Is 50% or higher:
- The vast majority are women:
- Although occult primary breast cancer has been reported in men:
- It is very rare
- Although occult primary breast cancer has been reported in men:
- The vast majority are women:
- Is 50% or higher:
- The incidence of breast cancer in mixed populations of men and women with metastatic axillary adenopathy:
- Other neoplasms that may present with axillary nodal involvement are:
- Lymphomas
- Melanomas
- Sarcomas
- Thyroid cancers
- Skin cancers
- Lung cancers
- Less often:
- Uterine, ovarian, sweat gland, or gastric cancers
- In approximately 30% of cases:
- The primary site is never identified
- In general:
- Initial Diagnostic Workup:
- Biopsy:
- The first step in the diagnostic workup of a patient with unexplained axillary adenopathy is:
- A biopsy
- Besides standard light microscopic examination of hematoxylin and eosin-stained sections:
- Other techniques such as:
- Immunohistochemistry and sometimes electron microscopy can help to narrow the differential diagnosis
- Other techniques such as:
- The first step in the diagnostic workup of a patient with unexplained axillary adenopathy is:
- Immunohistochemistry:
- The pathologic examination of a biopsy specimen for an isolated axillary lymph node metastatic adenocarcinoma or poorly differentiated carcinoma in a woman should include immunohistochemical staining for the following markers:
- Carcinoembryonic antigen (CEA)
- Cytokeratins 7 and 20
- Estrogen receptor (ER) and progesterone receptor (PR)
- Gross cystic disease fluid protein-15:
- GCDFP-15:
- Is identified by staining with the monoclonal antibody BRST2
- GCDFP-15:
- Mammaglobin
- Thyroid transcription factor (TTF-1)
- CA125
- Men:
- Should have routine staining for prostate cancer markers as well
- While none of these markers is sufficiently sensitive or specific to be used alone, certain patterns of expression favor the diagnosis of an occult breast cancer:
- Positive staining for:
- CEA, CK7, ER/PR, mammaglobin, CA125, and BRST2
- Negative staining for:
- CK20 and TTF-1
- Positive staining for:
- CEA is a sensitive marker for:
- Adenocarcinomas of the breast, lung, and gastrointestinal tract:
- But does not help to distinguish among these sites of origin
- Adenocarcinomas of the breast, lung, and gastrointestinal tract:
- On the other hand, differential expression of cytokeratins (CKs) can assist in this differentiation:
- CK20 is a low molecular weight cytokeratin:
- That is normally expressed in the gastrointestinal epithelium, urothelium, and in Merkel cells
- CK7 is expressed by tumors of the:
- Lung, ovary, endometrium, and breast:
- Not in the lower gastrointestinal tract
- Lung, ovary, endometrium, and breast:
- The pattern of CK20 and CK7 may be particularly helpful in suggesting a primary site:
- The presence of CK7 and absence of CK20:
- Favors a diagnosis of breast cancer
- The presence of CK7 and absence of CK20:
- TTF-1:
- Is rarely positive in breast cancers:
- While it is positive in 70% to 80% of non-squamous cancers arising in the lung
- Is rarely positive in breast cancers:
- CA-125:
- Is commonly positive in ovarian carcinomas:
- But is positive in about 10% of breast cancers
- Is commonly positive in ovarian carcinomas:
- ER/PR:
- Its presence in an axillary node, particularly in conjunction with other compatible IHC findings:
- Lends support to a diagnosis of an occult breast primary
- Although positive staining for ER and/or PR supports a possible diagnosis of breast cancer:
- These markers are nonspecific and they may also be expressed in:
- Ovarian, uterine, lung, stomach, thyroid, and hepatobiliary cancers:
- However:
- ER/PR staining of an axillary node is compelling evidence of a primary breast cancer
- However:
- Ovarian, uterine, lung, stomach, thyroid, and hepatobiliary cancers:
- These markers are nonspecific and they may also be expressed in:
- Its presence in an axillary node, particularly in conjunction with other compatible IHC findings:
- CK20 is a low molecular weight cytokeratin:
- Other breast cancer-specific IHC stains are:;
- BRST2 (for GCDFP) and mammaglobin:
- BRST2 is positive in 65% to 80% of cases:
- Is relatively specific for breast cancer:
- Rarely, it is positive in:
- Skin adnexal tumors, endometrial cancers, and salivary gland tumors
- Rarely, it is positive in:
- Is relatively specific for breast cancer:
- BRST2 is positive in 65% to 80% of cases:
- While mammaglobin is more sensitive, it is less specific for breast cancer:
- Gynecologic, lung, urothelial, thyroid, colon and hepatobiliary tumors may stain positive:
- Both stains are thus typically used together
- Gynecologic, lung, urothelial, thyroid, colon and hepatobiliary tumors may stain positive:
- BRST2 (for GCDFP) and mammaglobin:
- HER2 immunostaining:
- Is not generally useful for the differential diagnosis of a carcinoma arising in the axillary nodes as it lacks specificity:
- Furthermore, only 18% to 20% of breast cancers overexpress this protein:
- However, assay for HER2 overexpression by IHC or fluorescent in situ hybridization (FISH) is a routine component of the evaluation of all breast cancers:
- As it permits the identification of those women who are most likely to respond to treatments targeting HER2 (eg, the therapeutic monoclonal antibody trastuzumab)
- However, assay for HER2 overexpression by IHC or fluorescent in situ hybridization (FISH) is a routine component of the evaluation of all breast cancers:
- Furthermore, only 18% to 20% of breast cancers overexpress this protein:
- Is not generally useful for the differential diagnosis of a carcinoma arising in the axillary nodes as it lacks specificity:
- The pathologic examination of a biopsy specimen for an isolated axillary lymph node metastatic adenocarcinoma or poorly differentiated carcinoma in a woman should include immunohistochemical staining for the following markers:
- Biopsy:
- Modified radical mastectomy has been the traditional surgical treatment for many years
- Previously, the primary breast cancer was found in the mastectomy specimen:
- 40% to 80% of the time, but with the advent of much better mammography and ultrasound along with breast MRI, this rate is much lower now
- However, what was true then and still holds today:
- Is that no treatment to the breast itself results in an unacceptably high local recurrence rate
- An alternative to a modified radical mastectomy:
- Is complete ALND followed by whole-breast irradiation
- Axillary dissection:
- Provides local control while also fine tuning staging
- Theoretically the whole-breast radiation:
- Should control any subclinical disease in the breast not detected on imaging
- Primary radiation to the breast, axilla, and supraclavicular area without any surgery of the breast or axilla:
- Results in higher local and regional recurrence compared to surgery and radiation combined
- Axillary node dissection and whole-breast irradiation:
- Has been found to have equivalent survival as a modified radical mastectomy
- A recent meta-analysis of seven studies and more than 240 patients with occult primary breast cancers (0.3% to 0.8% of all breast cancers):
- Found 39% were treated with ALND and radiation while 47% had modified radical mastectomy and 15% had ALND alone
- With a mean follow-up of 5 years:
- The study found no difference in local regional recurrence (12.7% vs 9.8%), distant metastasis (7.2% vs 12.7%), or mortality (9.5% vs 17.9%) between ALND and radiation vs modified radical mastectomy (all p>0.16)
- ALND with radiation was superior to ALND alone in terms of local regional recurrence (12.7% vs 34.3%, p < 0.01) and trended towards improved survival but this was not statistically significant (P=0.09)
- References:
- Barton SR, Smith IE, Kirby AM, Ashley S, Walsh G, Parton M. The role of ipsilateral breast radiotherapy in management of occult primary breast cancer presenting as axillary lymphadenopathy. Eur J Cancer. 2011;47:2099-2106. PMID: 21658935. http://www.ncbi.nlm.nih.gov/pubmed/21658935
- Dockery MB, Gray HK, Pierce EH. Surgical significance of isolated axillary adenopathy. Ann Surg. 1957;145:104-107. http://www.ncbi.nlm.nih.gov/pubmed/13395289
- Macedo FI, Eid JJ, Flynn J, Jacobs MJ, Mittal VK. Optimal surgical management for occult breast carcinoma: a meta-analysis. Ann Surg Oncol. 2016;23:1838-1844. https://www.ncbi.nlm.nih.gov/pubmed/26832884
- Rueth NM, Black DM, Limmer AR, et al. Breast conservation in the setting of contemporary multimodality treatment provides excellent outcomes for patients with occult primary breast cancer. Ann Surg Oncol. 2015;22:90-95. [epub ahead of print]. http://www.ncbi.nlm.nih.gov/pubmed/25249256
- Walker GV, Smith GL, Perkins GH, et al. Population-based analysis of occult primary breast cancer with axillary lymph node metastasis. Cancer. 2010;116:4000-4006. PMID: 20564117. http://www.ncbi.nlm.nih.gov/pubmed/20564117
- Woo SM, Son BH, Lee JW, et al. Survival outcomes of different treatment methods for the ipsilateral breast of occult breast cancer patients with axillary lymph node metastasis: a single center experience. J Breast Cancer. 2013;16:410-416. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3893343/

Stewart-Treves Syndrome
- Stewart-Treves syndrome:
- Is a rare complication of longstanding lymphedema
- It is a deadly cutaneous angiosarcoma
- Most commonly, this tumor is a result of lymphedema induced by radical mastectomy to treat breast cancer:
- Unfortunately, although the breast cancer may be cured with such radical surgery:
- This second primary cancer may be responsible for the patient’s worsening course.
- Unfortunately, although the breast cancer may be cured with such radical surgery:
- The term Stewart-Treves syndrome is broadly applied to an angiosarcoma that arises in a chronically lymphedematous region due to any cause, including:
- Congenital lymphedema and other causes of secondary lymphedema unassociated with mastectomy
- As reported by Durr et al in 2004, this lymphangiosarcoma occurs as a rare complication:
- Lymphangiosarcoma is a misnomer because this malignancy seems to arise from blood vessels instead of lymphatic vessels:
- A more appropriate name is hemangiosarcoma
- Lymphangiosarcoma is a misnomer because this malignancy seems to arise from blood vessels instead of lymphatic vessels:
- In 1906, Lowenstein first described angiosarcoma:
- In a patient’s arm that had been affected by severe posttraumatic lymphedema for 5 years
- In 1948, Stewart and Treves reported this rare secondary malignancy in six cases of angiosarcoma in postmastectomy lymphedema:
- They recognized that an edematous arm after radical mastectomy for breast cancer may suggest recurrent breast cancer:
- But that long-standing chronic edema without recurrent cancer may occasionally produce “a heretofore unrecognized and unreported sequel … long after the malignant breast neoplasm has apparently been arrested … a new specific tumor”
- Stewart and Treves suggested that these angiosarcomas were probably not observed previously because they were mistaken for recurrent, inoperable, cutaneous manifestations of breast cancer
- They recognized that an edematous arm after radical mastectomy for breast cancer may suggest recurrent breast cancer:
- Clinical suspicion should be high:
- As this syndrome is easily misdiagnosed and treatment is advertently delayed
- Pathophysiology:
- The pathogenic mechanism by which lymphedema may induce angiosarcoma has been the subject of controversy
- Stewart and Treves found a high incidence of third malignancies in patients with postmastectomy angiosarcoma:
- Thus, they speculated that a systemic carcinogenic factor was the main causative factor in the pathogenesis of lymphangiosarcomas.
- In 1979, Schreiber and others postulated the concept of local immunodeficiency in the presence of lymphedema:
- This theory is supported by experimental evidence:
- In 1960, Stark and associates demonstrated that homograft skin transplanted to lymphedematous arms survive much longer than those transplanted to healthy arms:
- Therefore, lymphedema may cause some degree of local immunodeficiency and lead to oncogenesis
- In 1960, Stark and associates demonstrated that homograft skin transplanted to lymphedematous arms survive much longer than those transplanted to healthy arms:
- This theory is supported by experimental evidence:
- The possibility that radiation therapy has an important role in the induction of lymphangiosarcoma is also postulated:
- Sternby et al reported that in their study:
- The patient with the shortest interval between radical mastectomy and the onset of the tumor (8 months) received both preoperative radiation therapy of the breast and involved axillary lymph nodes followed by fractionated radiation
- Others suggest that irradiation is not an essential factor in the pathogenesis of this tumor
- Finally, irradiation may be an indirect cause of lymphangiosarcomas because it may cause axillary node sclerosis and thereby accelerate and aggravate the edema
- Sternby et al reported that in their study:
- Clinical data from Swedish women with previous breast cancer who developed angiosarcomas / lymphangiosarcomas on the thoracic wall / upper extremity between 1958 and 2008:
- Showed 31 angiosarcomas developed at a median age of 71 years
- The 14 women treated for breast cancer with radical mastectomy and radiotherapy from 1949 to 1988 developed angiosarcomas in edematous arms after a median 11 years
- Whereas 17 females treated by segmental resection, antihormonal treatment, and radiotherapy from 1980 to 2005 developed angiosarcomas in the irradiated field on the thoracic wall after a median 7.3 years
- Epidemiology:
- Frequency:
- Currently, approximately 400 cases of Stewart-Treves syndrome are reported in the world literature
- In 1962, Schirger calculated that the incidence of this disease is 0.45% in patients who survive at least 5 years after radical mastectomy
- Another analysis calculated it as occurring in 0.03% of patients surviving 10 or more years after radical mastectomy:
- As a result of the increase in conservative treatment for breast carcinoma and improvement of operative and radiation therapy techniques:
- The prevalence of Stewart-Treves syndrome has decreased
- As a result of the increase in conservative treatment for breast carcinoma and improvement of operative and radiation therapy techniques:
- Race:
- No racial predominance exists for Stewart-Treves syndrome
- Gender:
- Most patients with Stewart-Treves syndrome are women with a history of breast cancer that has been treated with radical mastectomy:
- Which causes chronic lymphedema
- Most patients with Stewart-Treves syndrome are women with a history of breast cancer that has been treated with radical mastectomy:
- Age:
- Stewart-Treves syndrome usually occurs in middle-aged or elderly women, a few years or many years after mastectomy:
- In 1981, Sordillo and associates reported a peak incidence in persons aged 65 to 70 years
- In 1972, Woodward et al described a series of 23 patients in a review of 163 cases of Stewart-Treves syndrome from the literature:
- They recorded an average patient age of 68.8 years at the onset of lymphangiosarcoma:
- The youngest patient was aged 44 years and the oldest, 84 years
- They recorded an average patient age of 68.8 years at the onset of lymphangiosarcoma:
- Frequency:
- Once diagnosed:
- Surgical excision is the treatment of choice, sometimes requiring forequarter amputation
- Early amputation or wide local excision provides the best chance of long-term survival in patients with Stewart-Treves syndrome
- Some authorities favor radical ablative surgery with an early diagnosis, in order to confer a reasonable prognosis with this rare but aggressive disease
- A nihilistic approach is undesirable
- The most common approach in patients with lymphangiosarcoma is amputation of the limb or forequarter rather than wide local surgical excision
- Even in cases with early surgical treatment, the prognosis is disappointing, with a high rate of local recurrence and metastasis
- Metastatic disease should exclude surgical treatment unless surgery is useful for symptomatic improvement
- Chemotherapy may have some role:
- However its benefit is unclear
- Chemotherapy and irradiation continue to be evaluated as adjuvants to surgery for the treatment of Stewart-Treves syndrome:
- Currently, these treatment options offer little benefit
- Multiple studies have shown the 5-year survival to be very poor:
- At less than 10%
- The mean survival is 20 months
- Multimodal therapy including:
- Hyperthermic isolated limb perfusion with tumor necrosis factor-alpha and melphalan, combined with radical resection of the affected skin and subcutaneous tissue including the fascia, with large safety margins, may provide enhanced survival
- In 2000, Grobmyer and associates found no statistical significant difference in the survival rates of patients treated with chemotherapy compared with those treated with irradiation:
- Although long-term survivors after either radiation therapy or systemic chemotherapy have been reported:
- The overall results have been discouraging
- Although long-term survivors after either radiation therapy or systemic chemotherapy have been reported:
- A questionable response to weekly paclitaxel has been described:
- As a result of these findings, these treatment options are reserved for patients with inoperable, advanced disease or those who refuse surgery
- Intra-arterial mitoxantrone / paclitaxel was used for angiosarcoma of the lower limb associated with chronic lymphedema (Stewart-Treves syndrome) in a patient with cervical cancer
- In 1994, Furue et al demonstrated that immunotherapy may be beneficial as palliative treatment for pleural effusions caused by metastatic angiosarcoma:
- Expression of VEGF-C makes this angiosarcoma a good potential candidate for targeted antilymphangiogenic therapy
- Stewart-Treves syndrome occurring in the abdominal wall was successfully treated with eribulin mesylate:
- A structurally modified analog of halichondrin B, originally isolated from the marine sponge Halichondria okadai

- References
- Cui L, Zhang J, Zhang X, et al. Angiosarcoma (Stewart-Treves syndrome) in postmastectomy patients: report of 10 cases and review of literature. Int J Clin Exp Pathol. 2015;8(9):11108-11115.
- Penel N, Bui BN, Bay JO, et al. Phase II trial of weekly paclitaxel for unresectable angiosarcoma: the ANGIOTAX Study. J Clin Oncol. 2008;26(32):5269-5274.
- Stewart FW, Treves N. Lymphangiosarcoma in postmastectomy lymphedema: A report of six cases in elephantiasis chirurgica. Cancer. 1948. 1:64-81.
- Hallel-Halevy D, Yerushalmi J, Grunwald MH, Avinoach I, Halevy S. Stewart-Treves syndrome in a patient with elephantiasis. J Am Acad Dermatol. 1999 Aug. 41(2 Pt 2):349-50.
- Offori TW, Platt CC, Stephens M, Hopkinson GB. Angiosarcoma in congenital hereditary lymphoedema (Milroy’s disease)–diagnostic beacons and a review of the literature. Clin Exp Dermatol. 1993 Mar. 18(2):174-7.
- Farhat MM, Le Guern A, Peugniez C, Dabouz F, Quinchon JF, Modiano P. [Angiosarcoma in primary lymphoedema: A rare complication]. Ann Dermatol Venereol. 2018 Apr. 145 (4):266-269.
- Schreiber H, Barry FM, Russell WC, Macon WL 4th, Ponsky JL, Pories WJ. Stewart-Treves syndrome. A lethal complication of postmastectomy lymphedema and regional immune deficiency. Arch Surg. 1979 Jan. 114(1):82-5.
- Stark RB, Dwyer EM, De Forest M. Effect of surgical ablation of regional lymph nodes on survival of homografts. Ann NY Acad Sci. 1960. 87:140-148.
- Cabral ANF, Rocha RH, Amaral ACVD, Medeiros KB, Nogueira PSE, Diniz LM. Cutaneous angiosarcoma: report of three different and typical cases admitted in a unique dermatology clinic. An Bras Dermatol. 2017 Mar-Apr. 92 (2):235-238.
- Sternby NH, Gynning I, Hogeman KE. Postmastectomy angiosarcoma. Acta Chir Scand. 1961. 121:420-432.
- Styring E, Fernebro J, Jonsson PE, et al. Changing clinical presentation of angiosarcomas after breast cancer: from late tumors in edematous arms to earlier tumors on the thoracic wall. Breast Cancer Res Treat. 2010 Jan 20.
- Stanczyk M, Gewartowska M, Swierkowski M, Grala B, Maruszynski M. Stewart-Treves syndrome angiosarcoma expresses phenotypes of both blood and lymphatic capillaries. Chin Med J (Engl). 2013 Jan. 126(2):231-7.
- Schirger A. Postoperative lymphedema: etiologic and diagnostic factors. Med Clin North Am. 1962 Jul. 46:1045-50.
- Wierzbicka-Hainaut E, Guillet G. [Stewart-Treves syndrome (angiosarcoma on lyphoedema): A rare complication of lymphoedema]. Presse Med. 2010 Dec. 39(12):1305-8.
#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOncologist #BreastCancer #Angiosarcoma #StewartTrevesSyndrome #CASO #Miami #CenterforAdvancedSurgicalOncologist
Bilateral Salpingo‐Oophorectomy
- Risk‐reducing bilateral salpingo‐oophorectomy (RRBSO) – or the removal of fallopian tubes and ovaries:
- Is the advised surgical prophylaxis for hereditary breast and ovarian cancer (HBOC) mutation carriers
- Other preventive and cancer screening measures available for these women:
Bilateral Salpingo‐Oophorectomy
- Risk‐reducing bilateral salpingo‐oophorectomy (RRBSO) – or the removal of fallopian tubes and ovaries:
- Is the advised surgical prophylaxis for hereditary breast and ovarian cancer (HBOC) mutation carriers
- Other preventive and cancer screening measures available for these women:
- Such as serial CA125 levels and pelvic ultrasounds:
- Have not been shown to reduce cancer mortality in this high‐risk population
- Such as serial CA125 levels and pelvic ultrasounds:
- RRBSO has been associated with significantly improved cancer‐specific mortality:
- For ovarian, fallopian tube, peritoneal and breast cancers, as well as improved all‐cause mortality in BRCA carriers
- In a multicenter, prospective study of 2482 women with a known BRCA1 or BRCA2 mutation:
- Women treated with RRBSO had a:
- Decreased ovarian cancer risk (1% vs 6%)
- Decreased breast cancer risk (2% vs 6%)
- Improved all‐cause mortality (3% vs 10%)
- Women treated with RRBSO had a:
- Retrospective data supports the relative risk of gynecologic cancer:
- After RRBSO to be 0.04 (95% CI, 0.01‐0.16)
- In that study, only 2 of 253 women who underwent RRBSO were later diagnosed with peritoneal carcinoma:
- 58 women out of 292 matched controls received a diagnosis of the ovarian, fallopian tube, or peritoneal cancer after a mean follow up of 8.8 years
- In a prospective study which controlled for history of prophylactic mastectomy:
- The hazard ratio for the diagnosis of breast cancer or gynecologic cancer in a patient with BRCA after RRBSO was 0.25 (95% CI, 0.08‐0.74)
- As more recent data have supported that many ovarian cancers may originate within the fallopian tube:
- There are currently ongoing studies exploring whether bilateral salpingectomy alone is an effective risk‐reducing procedure
- Generally, BRCA‐positive women elect to defer RRBSO:
- Until they complete their childbearing
- Age‐related risk, however, differs between BRCA1 and BRCA2 carriers:
- BRCA1 carriers are at an elevated lifetime risk for ovarian cancer compared to BRCA2 carriers and are also more likely to develop it earlier in life:
- Specifically, women with BRCA1 mutations have an:
- Average age at ovarian cancer diagnosis of 50 years
- A significantly increased ovarian cancer risk starting at 35 years:
- Which continues to increase with age
- Specifically, women with BRCA1 mutations have an:
- Women with BRCA2 mutations:
- Have an average age of ovarian cancer diagnosis of 60 years
- A significantly increased ovarian cancer risk starting at 50 years:
- Which then plateaus at a 14% risk
- Therefore, BRCA2 carriers may elect to defer RRBSO to a later age compared with BRCA1 carriers:
- However, if they choose to do so, they must be counseled that they may not receive the benefit of decreased breast cancer risk after RRBSO
- BRCA1 carriers are at an elevated lifetime risk for ovarian cancer compared to BRCA2 carriers and are also more likely to develop it earlier in life:
- Nevertheless, the society of Gynecologic Oncology (SGO):
- Continues to recommend that BRCA1 and BRCA2 mutation carriers:
- Undergo RRBSO after completing childbearing or by age 35 to 40 years
- Continues to recommend that BRCA1 and BRCA2 mutation carriers:
- Thorough preoperative counseling is critical in helping patients decide whether to proceed with RRBSO:
- RRBSO is generally performed laparoscopically and is a low‐risk procedure:
- The reported complication rate (both major and minor) of RRBSO:
- Has been quoted as 4% but is even lower at high volume institutions
- The reported complication rate (both major and minor) of RRBSO:
- In addition, patients must be advised that there is a 4% to 8% risk of discovering an occult malignancyeither at the time of RRBSO or on final pathology
- Preoperative serum CA125 should be obtained and patients should undergo a pelvic ultrasound
- Patients should be consented for ovarian cancer staging surgery in case visible disease is seen and counseled that an occult malignancy may be detected on final pathology, thus requiring additional surgery
- Women should also be counseled that at the time of RRBSO they will undergo surgical menopause and may begin to experience hot flashes, mood changes, vaginal dryness, dyspareunia, decreased libido, osteoporosis, cardiovascular disease, and possible impaired cognitive function:
- Although surgical menopause before age 45:
- Has been associated with increased overall mortality in the general population, this risk must be balanced with the substantially decreased all‐cause mortality after risk‐reducing surgery for the high‐risk HBOC population
- Nonhormonal agents should be used as a first‐line therapy for these symptoms:
- But hormonal replacement therapy (HRT) is also likely safe on the basis of a recent study of almost 900 postoophorectomy BRCA1 mutation carriers:
- In that prospective longitudinal study, investigators found that HRT use was not associated with an increased risk of breast cancer (HR 0.97, 95% CI, 0.62‐1.52, P = .89)
- However, when analyzing only women who used HRT:
- The incidence of breast cancer was lower with estrogen‐only HRTcompared with combination estrogen and progesterone (12% vs 22%, log‐rank P = .04)
- Estrogen‐only HRT is only recommended for women who have undergone a hysterectomy, as without progesterone support, it significantly increases the risk for endometrial cancer in the general population
- A recent meta‐analysis including three trials with 1100 patients also demonstrated there was not a significantly higher breast cancer risk associated with HRT after RRBSO in BRCA1 and BRCA2 mutation carriers (HR 0.98, 95% CI, 0.63‐1.52)
- Nevertheless, the relationship between HRT and individual all‐cancer risk is complex and imperfectly understood at this time
- The results of long‐term, prospective studies are necessary to draw more definitive conclusions in this high‐risk population
- But hormonal replacement therapy (HRT) is also likely safe on the basis of a recent study of almost 900 postoophorectomy BRCA1 mutation carriers:
- Although surgical menopause before age 45:
- RRBSO is generally performed laparoscopically and is a low‐risk procedure:
- References:
- Domchek SM, Friebel TM, Singer CF, et al. Association of risk‐ reducing surgery in BRCA1 or BRCA2 mutation carriers with cancer risk and mortality. JAMA. 2010;304(9):967‐975.
- Rebbeck TR, Lynch HT, Neuhausen SL, et al. Prophylactic oophor- ectomy in carriers of BRCA1 or BRCA2 mutations. N Engl J Med. 2002;346(21):1616‐1622.
- Kauff ND, Satagopan JM, Robson ME, et al. Risk‐reducing salpingo‐ oophorectomy in women with a BRCA1 or BRCA2 mutation. N Engl J Med. 2002;346(21):1609‐1615.
- Antoniou A, Pharoah PDP, Narod S, et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case Series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet. 2003;72(5):1117‐1130.
- Manchanda R, Abdelraheim, Johnson M, et al. Outcome of risk‐ reducing salpingo‐oophorectomy in BRCA carriers and women of unknown mutation status. BJOG. 2011;118(7):814‐824.
- Rocca WA, Grossardt BR, de Andrade M, Malkasian GD, Melton LJ. Survival patterns after oophorectomy in premenopausal women: a population‐based cohort study. Lancet Oncol. 2006;7(10):821‐828.
- Kotsopoulos J, Gronwald J, Karlan BY, et al. Hormone replacement therapy after oophorectomy and breast cancer risk among BRCA1 mutation carriers. JAMA Oncology. 2018;4(8):1059.
- Marchetti C, De Felice F, Boccia S, et al. Hormone replacement therapy after prophylactic risk‐reducing salpingo‐oophorectomy and breast cancer risk in BRCA1 and BRCA2 mutation carriers: a meta‐ analysis. Crit Rev Oncol Hematol. 2018;132:111‐115.
- Such as serial CA125 levels and pelvic ultrasounds:
- Have not been shown to reduce cancer mortality in this high‐risk population
- RRBSO has been associated with significantly improved cancer‐specific mortality:
- For ovarian, fallopian tube, peritoneal and breast cancers, as well as improved all‐cause mortality in BRCA carriers
- In a multicenter, prospective study of 2482 women with a known BRCA1 or BRCA2 mutation:
- Women treated with RRBSO had a:
- Decreased ovarian cancer risk (1% vs 6%)
- Decreased breast cancer risk (2% vs 6%)
- Improved all‐cause mortality (3% vs 10%)
- Women treated with RRBSO had a:
- Retrospective data supports the relative risk of gynecologic cancer:
- After RRBSO to be 0.04 (95% CI, 0.01‐0.16)
- In that study, only 2 of 253 women who underwent RRBSO were later diagnosed with peritoneal carcinoma:
- 58 women out of 292 matched controls received a diagnosis of the ovarian, fallopian tube, or peritoneal cancer after a mean follow up of 8.8 years
- In a prospective study which controlled for history of prophylactic mastectomy:
- The hazard ratio for the diagnosis of breast cancer or gynecologic cancer in a patient with BRCA after RRBSO was 0.25 (95% CI, 0.08‐0.74)
- As more recent data have supported that many ovarian cancers may originate within the fallopian tube:
- There are currently ongoing studies exploring whether bilateral salpingectomy alone is an effective risk‐reducing procedure
- Generally, BRCA‐positive women elect to defer RRBSO:
- Until they complete their childbearing
- Age‐related risk, however, differs between BRCA1 and BRCA2 carriers:
- BRCA1 carriers are at an elevated lifetime risk for ovarian cancer compared to BRCA2 carriers and are also more likely to develop it earlier in life:
- Specifically, women with BRCA1 mutations have an:
- Average age at ovarian cancer diagnosis of 50 years
- A significantly increased ovarian cancer risk starting at 35 years:
- Which continues to increase with age
- Specifically, women with BRCA1 mutations have an:
- Women with BRCA2 mutations:
- Have an average age of ovarian cancer diagnosis of 60 years
- A significantly increased ovarian cancer risk starting at 50 years:
- Which then plateaus at a 14% risk
- Therefore, BRCA2 carriers may elect to defer RRBSO to a later age compared with BRCA1 carriers:
- However, if they choose to do so, they must be counseled that they may not receive the benefit of decreased breast cancer risk after RRBSO
- BRCA1 carriers are at an elevated lifetime risk for ovarian cancer compared to BRCA2 carriers and are also more likely to develop it earlier in life:
- Nevertheless, the society of Gynecologic Oncology (SGO):
- Continues to recommend that BRCA1 and BRCA2 mutation carriers:
- Undergo RRBSO after completing childbearing or by age 35 to 40 years
- Continues to recommend that BRCA1 and BRCA2 mutation carriers:
- Thorough preoperative counseling is critical in helping patients decide whether to proceed with RRBSO:
- RRBSO is generally performed laparoscopically and is a low‐risk procedure:
- The reported complication rate (both major and minor) of RRBSO:
- Has been quoted as 4% but is even lower at high volume institutions
- The reported complication rate (both major and minor) of RRBSO:
- In addition, patients must be advised that there is a 4% to 8% risk of discovering an occult malignancyeither at the time of RRBSO or on final pathology
- Preoperative serum CA125 should be obtained and patients should undergo a pelvic ultrasound
- Patients should be consented for ovarian cancer staging surgery in case visible disease is seen and counseled that an occult malignancy may be detected on final pathology, thus requiring additional surgery
- Women should also be counseled that at the time of RRBSO they will undergo surgical menopause and may begin to experience hot flashes, mood changes, vaginal dryness, dyspareunia, decreased libido, osteoporosis, cardiovascular disease, and possible impaired cognitive function:
- Although surgical menopause before age 45:
- Has been associated with increased overall mortality in the general population, this risk must be balanced with the substantially decreased all‐cause mortality after risk‐reducing surgery for the high‐risk HBOC population
- Nonhormonal agents should be used as a first‐line therapy for these symptoms:
- But hormonal replacement therapy (HRT) is also likely safe on the basis of a recent study of almost 900 postoophorectomy BRCA1 mutation carriers:
- In that prospective longitudinal study, investigators found that HRT use was not associated with an increased risk of breast cancer (HR 0.97, 95% CI, 0.62‐1.52, P = .89)
- However, when analyzing only women who used HRT:
- The incidence of breast cancer was lower with estrogen‐only HRTcompared with combination estrogen and progesterone (12% vs 22%, log‐rank P = .04)
- Estrogen‐only HRT is only recommended for women who have undergone a hysterectomy, as without progesterone support, it significantly increases the risk for endometrial cancer in the general population
- A recent meta‐analysis including three trials with 1100 patients also demonstrated there was not a significantly higher breast cancer risk associated with HRT after RRBSO in BRCA1 and BRCA2 mutation carriers (HR 0.98, 95% CI, 0.63‐1.52)
- Nevertheless, the relationship between HRT and individual all‐cancer risk is complex and imperfectly understood at this time
- The results of long‐term, prospective studies are necessary to draw more definitive conclusions in this high‐risk population
- But hormonal replacement therapy (HRT) is also likely safe on the basis of a recent study of almost 900 postoophorectomy BRCA1 mutation carriers:
- Although surgical menopause before age 45:
- RRBSO is generally performed laparoscopically and is a low‐risk procedure:
- References:
- Domchek SM, Friebel TM, Singer CF, et al. Association of risk‐ reducing surgery in BRCA1 or BRCA2 mutation carriers with cancer risk and mortality. JAMA. 2010;304(9):967‐975.
- Rebbeck TR, Lynch HT, Neuhausen SL, et al. Prophylactic oophor- ectomy in carriers of BRCA1 or BRCA2 mutations. N Engl J Med. 2002;346(21):1616‐1622.
- Kauff ND, Satagopan JM, Robson ME, et al. Risk‐reducing salpingo‐ oophorectomy in women with a BRCA1 or BRCA2 mutation. N Engl J Med. 2002;346(21):1609‐1615.
- Antoniou A, Pharoah PDP, Narod S, et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case Series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet. 2003;72(5):1117‐1130.
- Manchanda R, Abdelraheim, Johnson M, et al. Outcome of risk‐ reducing salpingo‐oophorectomy in BRCA carriers and women of unknown mutation status. BJOG. 2011;118(7):814‐824.
- Rocca WA, Grossardt BR, de Andrade M, Malkasian GD, Melton LJ. Survival patterns after oophorectomy in premenopausal women: a population‐based cohort study. Lancet Oncol. 2006;7(10):821‐828.
- Kotsopoulos J, Gronwald J, Karlan BY, et al. Hormone replacement therapy after oophorectomy and breast cancer risk among BRCA1 mutation carriers. JAMA Oncology. 2018;4(8):1059.
- Marchetti C, De Felice F, Boccia S, et al. Hormone replacement therapy after prophylactic risk‐reducing salpingo‐oophorectomy and breast cancer risk in BRCA1 and BRCA2 mutation carriers: a meta‐ analysis. Crit Rev Oncol Hematol. 2018;132:111‐115.
#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOncologist #Miami #CASO #CenterforAdvancedSurgicalOncology #RiskReducingSurgery #RRBSO #RiskReducingBilateralSalpinooforectomy
