My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
Thyroid nodules can occur in anyone, but certain factors make them more likely.
👥 Common Risk Factors
Age: Nodules become more common as we get older Female sex: Women develop thyroid nodules 3–4 times more often than men Iodine imbalance: Both deficiency and excess can play a role Family history: Thyroid nodules or thyroid cancer in first-degree relatives Autoimmune thyroid disease: Hashimoto’s thyroiditis increases nodule prevalence
☢️ Higher-Risk Situations
Radiation exposure to the head and neck, especially during childhood Prior radiation therapy for acne, tonsils, or cancer (historical treatments) Certain genetic syndromes (rare, but important)
🧠 Important clarification
Having risk factors does not mean a thyroid nodule is cancer.
➡️ Even in higher-risk individuals, most nodules are benign.
🔍 What matters most?
Risk factors help guide how closely we evaluate, but ultrasound findings ultimately determine:
Cancer risk Need for biopsy Follow-up strategy
📌 Key point for patients:
A thyroid nodule should never be ignored — but it should also never cause unnecessary fear. Proper, evidence-based evaluation is the answer.
Haugen BR et al. ATA Guidelines for Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid Guth S et al. Very high prevalence of thyroid nodules. Thyroid Gharib H et al. Evaluation and Management of Thyroid Nodules. Endocrine Practice
Most thyroid nodules cause no symptoms at all and are found incidentally on imaging or routine exams.
🔹 Common scenario: You feel well — the nodule is discovered on ultrasound
🔹 Important fact: Lack of symptoms does NOT mean the nodule is dangerous (or benign)
👀 When can symptoms occur?
Symptoms are more likely when nodules are large or strategically located:
A visible or palpable lump in the neck Difficulty swallowing or a sensation of food “getting stuck” Hoarseness or voice changes (uncommon, but important) Neck pressure or fullness, especially when lying flat Rarely, shortness of breath
⚠️ Hormone-related symptoms (less common)
A small percentage of nodules produce excess thyroid hormone (“hot” nodules), which may cause:
Palpitations Weight loss Heat intolerance Tremors or anxiety
🚨 When should you seek evaluation?
You should be evaluated if you notice:
✔️ A new or growing neck lump
✔️ Persistent hoarseness
✔️ Difficulty swallowing or breathing
✔️ A personal history of radiation exposure or family history of thyroid cancer
🔍 Bottom line:
Symptoms alone cannot determine whether a nodule is benign or malignant.
➡️ High-resolution ultrasound is essential for proper evaluation.
Don’t rely on symptoms — rely on proper imaging and expert evaluation.
📚 References
Haugen BR et al. ATA Guidelines for Thyroid Nodules. Thyroid Gharib H et al. Evaluation and Management of Thyroid Nodules. Endocrine Practice Durante C et al. JAMA
Thyroid nodules are very common in the general population.
🔹 With modern high-resolution ultrasound, thyroid nodules are detected in up to 50–60% of adults
🔹 More than 90% are benign
🔹 Most people have no symptoms and feel completely well
👉 The key is not panic — it’s proper evaluation.
🔍 How should thyroid nodules be evaluated?
The most important first step is a high-resolution thyroid ultrasound, which allows us to:
Accurately measure and characterize nodules Assess features associated with cancer risk Use validated risk-stratification systems (ATA / TI-RADS) Decide whether a biopsy is actually necessary
🧪 A key fact for patients
Only 5–10% of thyroid nodules are cancer.
When thyroid cancer is detected early, cure rates are excellent.
Having it evaluated correctly by an experienced team makes all the difference.
📚 References
Haugen BR et al. ATA Guidelines for Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid Durante C et al. Long-term surveillance of benign thyroid nodules. JAMA Gharib H et al. Fine-needle aspiration biopsy of thyroid nodules. Endocrine Practice
– Thyroid nodules are very common in the general population. With modern high-resolution ultrasound, nodules can be detected in up to 50% to 60% of adults.
👉 The good news: more than 90% of thyroid nodules are benign.
🔍 What is the best way to evaluate a thyroid nodule?
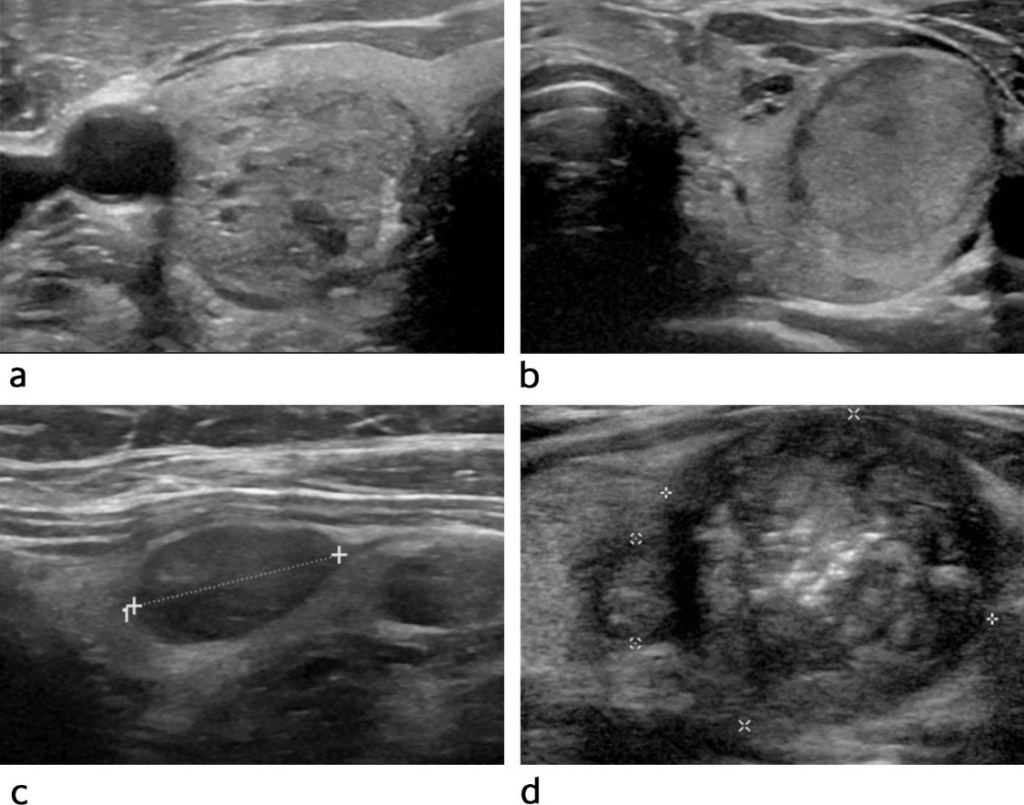
The first and most important test is a high-resolution thyroid ultrasound. It allows us to:
Accurately characterize the nodule (size, margins, echogenicity, calcifications) Stratify cancer risk using validated systems (such as ATA or TI-RADS) Determine whether a biopsy is necessary
🧪 When is a biopsy needed?
If the ultrasound shows suspicious features, a ultrasound-guided fine-needle aspiration biopsy (FNAB) is recommended.
✔️ This is a safe, minimally invasive, outpatient procedure that provides highly accurate information to determine whether a nodule is benign or malignant, helping avoid unnecessary surgery.
📊 Key facts (evidence-based)
Thyroid nodules are found in up to 60% of adults on ultrasound Only 5% to 10% of nodules are malignant Ultrasound-guided FNAB has high diagnostic accuracy and a very low complication rate
🏥 Experience you can trust
👨⚕️ Dr. Rodrigo Arrangoiz
Surgical Oncologist | Thyroid, Head & Neck, and Breast Surgery
📌 Take-home message: Early detection and proper evaluation of thyroid nodules make a real difference—protecting patients from unnecessary treatments while identifying cancer early when it is most curable.
📚 References
Haugen BR et al. 2015 ATA Guidelines for Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. Russ G et al. European Thyroid Association Guidelines for Ultrasound Malignancy Risk Stratification (EU-TI-RADS). Eur J Endocrinol. Gharib H et al. Fine-Needle Aspiration Biopsy of Thyroid Nodules. Endocrine Practice. Durante C et al. Long-term Surveillance of Benign Thyroid Nodules. JAMA.
Gives rise to the superior laryngeal nerve (SLN) and recurrent laryngeal nerve (RLN) in the neck
After descending toward the larynx:
The SLN divides into:
The internal laryngeal nerve (ILN)
External laryngeal nerve (ELN)
The RLN innervates all of the intrinsic muscles of the larynx:
Except the cricothyroid muscle:
This muscle, tenses the vocal cords and adducts the vocal cords:
Is innervated by the ELN
The other branch of the SLN, the ILN:
Provides sensory innervation to the laryngeal mucosa
There are many exceptions to the normal innervation of the laryngeal muscles:
Which can influence the interpretation of laryngoscopy results or voice changes after thyroid surgery
A neural anastomosis:
That provides additional motor innervation to the muscles of the larynx normally innervated by the injured nerve:
Can contribute to an incorrect interpretation of injury during laryngoscopy or stroboscopy
According to recent clinical studies:
Electrical stimulation of the RLN can cause contraction of the cricothyroid muscle:
This suggests that extra-laryngeal branches and or other communications of the RLN:
Can sometimes contribute to innervation of this muscle
The laryngeal nerves:
Can form a great variety of anastomoses:
These various connections among the ILN, ELN, and RLN have been investigated by many anatomists over the centuries
Claudius Galen:
Was the first to describe the communication between the ILN and RLN
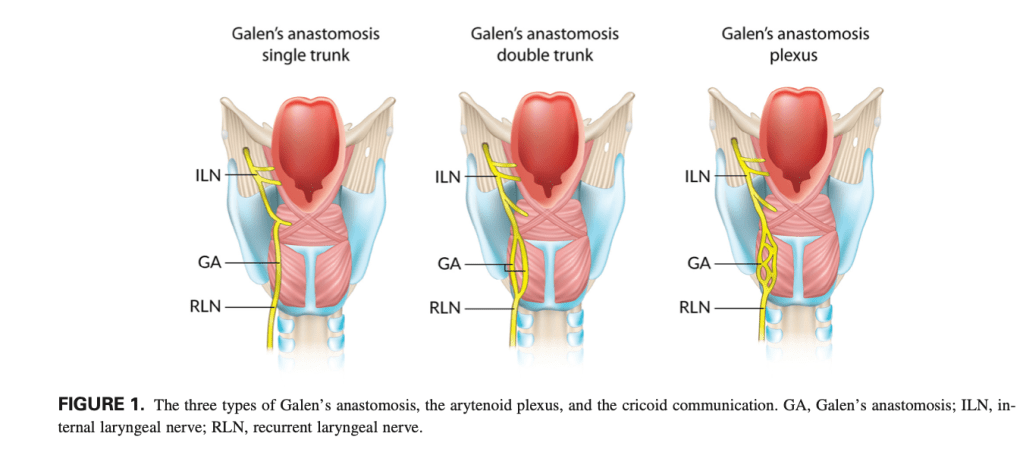
Currently, Galen’s anastomosis:
Is most commonly defined as:
The direct communication between the posterior branches of the ILN and the RLN
It can occur as:
A single trunk
A double trunk
A plexus
Besides Galen’s anastomosis, other communications have been observed and described as follows:
The arytenoid plexus:
Which links the anterior branch of the RLN with the arytenoid branch of the ILN
The arytenoid plexus and the cricoid communication. AP, arytenoid plexus; CA, cricoid communication; ILN, internal laryngeal nerve; RLN, recurrent laryngeal nerve (a, anterior; p, posterior).
The cricoid communication:
Which connects branches originating bilaterally from the RLNs with the superior branch from the deep portion of the arytenoid plexus
The thyroarythenoid communication:
Which is formed by the ascending branch of the RLN and the descending branch from the anterior branch of the ILN
The thyroarytenoid communication and the communication between the external laryngeal nerve (ELN) and the recurrent laryngeal nerve (RLN). CN, communicating nerve; ILN, internal laryngeal nerve; TAC, thyroarytenoid communication
The communication between the ELN and RLN:
Human communicating nerve
The communication between the ILN and ELN
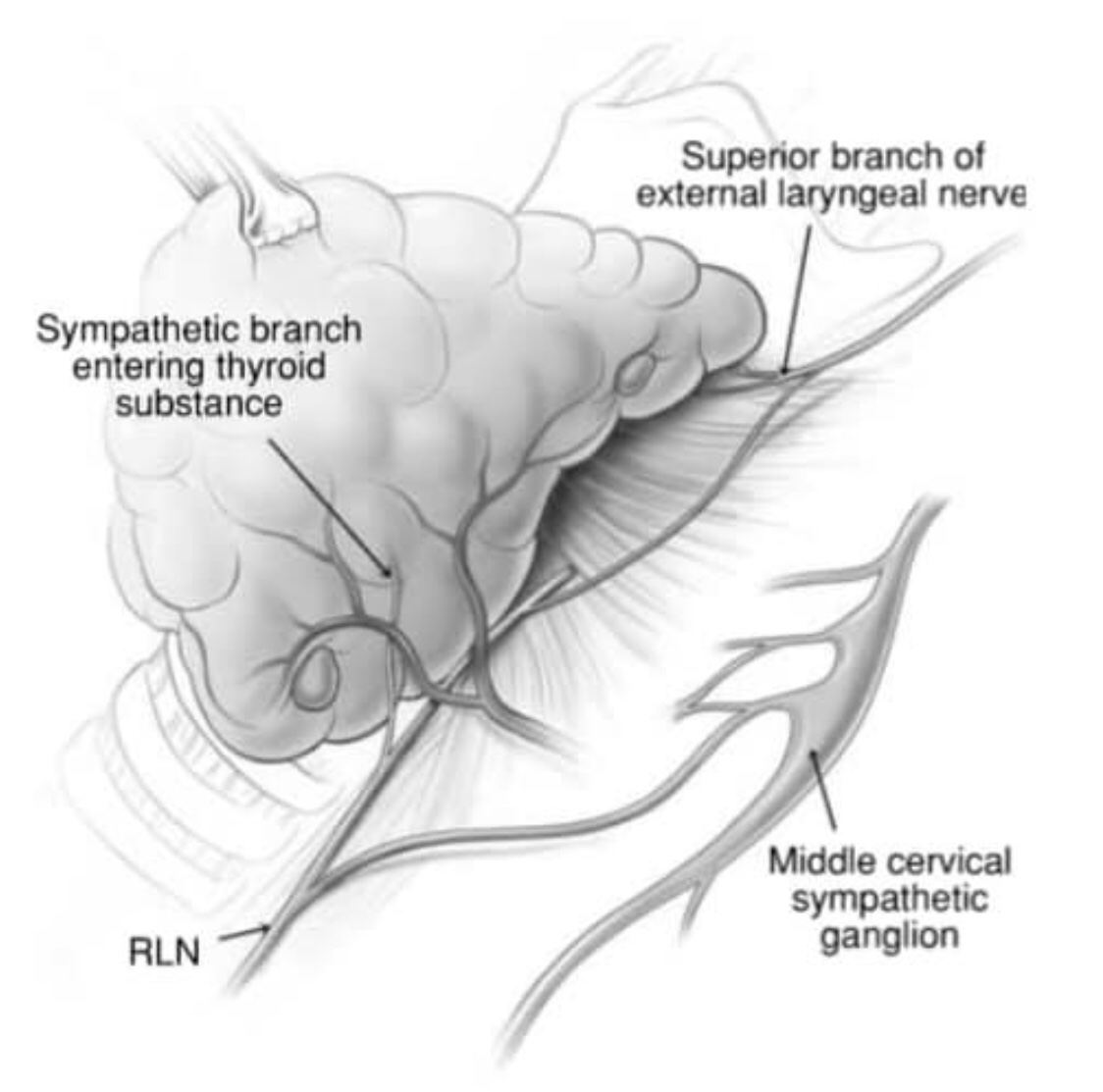
The communication between the RLN and the sympathetic trunk
Communications between the internal laryngeal nerve (ILN) and the external laryngeal nerve (ELN) and between the recurrent laryngeal nerve (RLN) and the sympathetic trunk. SLN, superior laryngeal nerve; TF, thyroid foramen.
Despite progress in the development of new techniques:
Such as intra-operative nerve monitoring:
Which help to reduce the risk of iatrogenic injuries during thyroid surgeries and other procedures conducted in close proximity to the laryngeal nerves:
The laryngeal muscles are often paralyzed postoperatively due to iatrogenic injury to the laryngeal nerves
In view of the complexity and variability of the anatomy in this region:
Detailed anatomical knowledge is crucial if surgery is to be both successful and safe, and to reduce the risk of nerve injury
Observing an intra-laryngeal anastomosis during laryngeal surgery or an extra-laryngeal communication between laryngeal nerves during thyroid surgery:
Can lead to confusion, misidentification, and an increased risk of iatrogenic injury
A thorough understanding of the complex anastomoses between the laryngeal nerves is crucial in patients with laryngeal muscle paralysis
Paralyzed laryngeal muscles can be spontaneously reinnervated from an anastomosis between laryngeal nerves
Additionally, in cases in which surgical reinnervation is required, some of the nerves that form anastomoses can be used as grafts to restore damaged nerve connections
On the other hand, variations in the normal anatomy of the laryngeal nerves can disrupt selective surgical laryngeal reinnervation:
A procedure based on the assumption that each laryngeal muscle is supplied by only one nerve branch originating from the RLN
Anastomoses among laryngeal nerves can result in exceptions to this rule
Such anastomoses have been widely described in the literature:
However, there is still no consensus about their prevalence and functionality
The significant heterogeneity among studies reporting data on anastomoses between the laryngeal nerves is noteworthy:
For example, the reported prevalence of the most common communication, Galen’ s anastomosis:
Ranges from 25% to 100%
Prevalence of Galen’s anastomosis:
A total of 14 studies (n = 890 hemilarynges) presented data on the prevalence of Galen’s anastomosis
The overall pooled prevalence rate:
Was 76.7% (95% confidence interval [CI]: 59.0– 90.0)
Subgroup analysis revealed no significant difference in the prevalence of Galen’s anastomosis between the right and left sides
Subgroup analyses by gender (males vs females) and geographical origin, and the sensitivity analysis, also revealed no significant differences:
However, although the difference was not significant:
The prevalence of the anastomosis was highest in Europeans (88.2%) and lowest in North Americans (44.8%)
Analysis of the different types of Galen’s anastomosis (two studies, n = 261 anastomoses):
Showed a significant difference in the prevalence between single versus double trunk and plexus formation
But no significant difference between double trunk and plexus formation
The most common type of Galen’s anastomosis was a single trunk:
With a pooled prevalence rate 92.3% (95% CI: 84.1–97.5)
This was followed by the double trunk anastomosis type:
With a pooled prevalence of 4.2% (95% CI: 0.5– 10.7)
The plexus formation type with a pooled prevalence of 3.5% (95% CI: 0.2–9.5) (I2: 70.4%, 95% CI: 0–93.3; Co- chran’s Q, P value = 0.066
Prevalence of a communication between the ELN and RLN
A total of eight studies (n = 639 hemilarynges) provided data on the prevalence of the communication between the ELN and RLN
The overall meta-analysis revealed that this communication was present in:
21.3% of hemilarynges (95% CI: 3.8–46.0)
A subgroup analysis showed no significant difference between left and right sides
Although the difference was not statistically significant:
The pooled prevalence rate calculated for the North American subgroup (32.0%) was twice that for the European subgroup (14.4%)
Prevalence of the arytenoid plexus:
Five studies (n = 478 hemilarynges) included data on the prevalence of the arytenoid plexus:
The pooled prevalence rate was 79.7% (95% CI: 41.1–100)
In the European subgroup:
The arytenoid plexus was observed in 96.9% of hemilarynges (95% CI: 83.6–100)
Subgroup analysis revealed no significant difference with respect to side
Prevalence of the cricoid communication:
Two studies (n = 120 hemilarynges) reported prevalence data for the cricoid communication:
The pooled prevalence rate was 19.7% (95% CI: 0–100)
There was no significant difference in sub- group analysis based on side
Prevalence of the thyroarytenoid communication:
A total of three studies (n = 430 hemilarynges) presented data on the prevalence of the thyroarytenoid communication:
The overall pooled prevalence was 6.3% (95% CI: 0.4–16.9)
In subgroup analysis, there was no significant difference in pooled prevalence between the right and left sides:
The calculated pooled rate for the left side (15.9%) was almost twice that for the right side (8.8%)
Communication between the ILN and ELN:
A total of two studies (n = 280 hemilarynges) reported data on a communication between the ILN and ELN
The pooled prevalence estimate of this communication in hemilarynges was 8.8% (95% CI: 0–35.3; I2 97.0%, 95% CI: 92.2–98.8; Cochran’s Q, P value <0.001)
In 1984 Göran Åkerström, on the basis of 503 necropsies, analysed the location of the parathyroid glands:
Together with the work of Gilmour (n=478) and Wang (n=160), they form the foundations of our current knowledge on the subject
Dr. Juan M. Rangone modified the diagrams from Åkerström’s original publication to come up with the percentages of location of the “normodescended” parathyroid glands:
A. Percentages of the different locations of the superior parathyroid glands:
80% corresponds to the midglandular variant
12% to the cricopharyngeal variant
Usually located 1 cm higher than the crossing of the recurrent laryngeal nerve and the inferior thyroid artery
B. Percentages of the different locations of the inferior parathyroid glands:
Roughly 90% are located at the level, or no more than 1 cm below the inferior pole of the thyroid gland
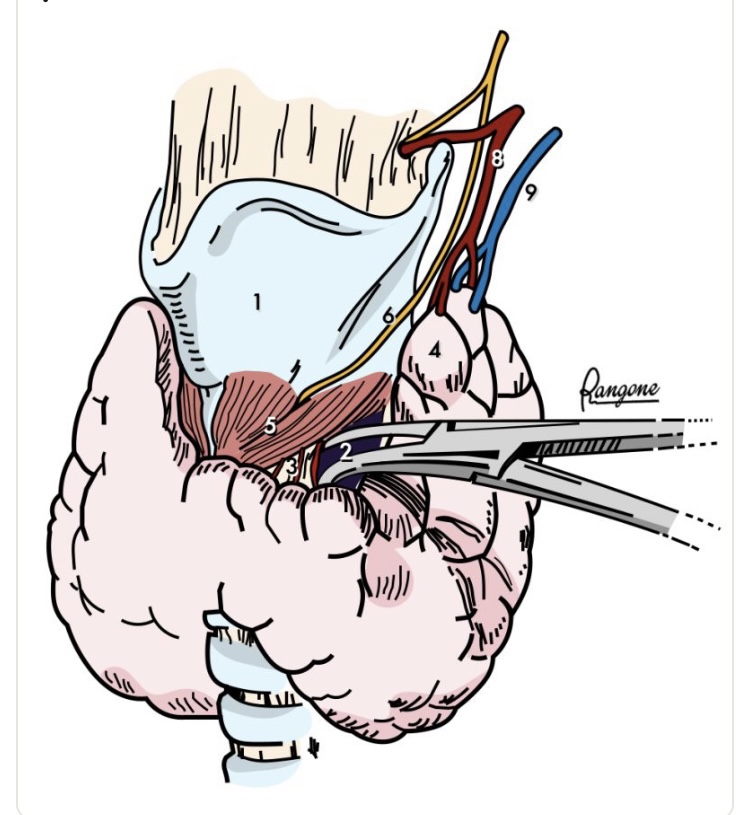
The lower and lateral retraction of the upper thyroid pole:
Reveals a diamond-shaped avascular space
The area is limited:
Medially:
By the lamina of the thyroid cartilage (superiorly) and cricoid cartilage (inferiorly):
Both covered by the cricothyroid muscle
Inferolaterally:
The space is circumscribed by the medial border of the upper thyroid pole and the upper border of the thyroid isthmus
The “roof” of the area:
Is covered by 2 or 3 “bridging” blood vessels that must be controlled to access the space
The “opening” of this virtual space:
Prior to the ligature of the upper thyroid pedicle:
Is a safety maneuver to protect the external branch of the superior laryngeal nerve
Landmarks:
Thyroid cartilage
Reeve cricothyroid space
Space with “bridging” blood vessels
Upper thyroid pole
Cricothyroid muscle
External branch of the superior larngeal nerve
Superior thyroid artery
Superior thyroid vein
Reference:
Abdullah H, Bliss R, Reeve T, Delbridge L (2000) Recognition of the avascular space medial to the upper pole of the thyroid and its surgical implications. Asian J. Surg. 23: 86–9.
👉The external branch of the superior laryngeal nerve (EBSLN) has been labelled ‘the neglected nerve’ of thyroid surgery.
👉Most surgeons have simply attempted to avoid this nerve on the assumption that so doing will prevent injury; however, it is now recognized that injury is relatively common and associated with the potential for significant impairment, espe- cially for those who use their voices professionally.
👉I was taught to always attempt to identify the nerve and recommend doing so.
👉Recently Aina and Hisham have shown that the nerve can be routinely identified in over 90% of cases, a level that sets a new benchmark for head and neck surgeons / endocrine surgeons.
👉The key to identifying the nerve is to develop the avascular plane between the cricothyroid muscle and the medial border of the upper pole of the thyroid lobe, a manoeuvre facilitated by lateral retraction of the lobe.
👉Awareness of the various positions of the EBSLN according to the Cernea classification is also essential if the nerve is to be both identified and preserved.
👉Type 1 EBSLN are located well clear of the thyroid, more than 1 cm above the upper pole of the lobe passing directly into the cricothyroid muscle.
👉Type 2a nerves pass in the vicinity of the superior thyroid vessels as they enter the gland substance.
👉Type 2b nerves cross over the anterior surface of the thyroid lobe.
👉Awareness of the anatomic variations, such as the nerve of Galen, a direct communication between the RLN and EBSLN, is important in avoiding injury to the nerve.
The true prevalence of iatrogenic injury to the EBSLN during thyroid surgery remains difficult to quantify, largely due to underdiagnosis and variability in clinical presentation.
– The pathophysiology and anatomical risk stratification of EBSLN injury were elegantly described by Cernea et al. in 1992 [1]. In this landmark study, the variant in which the nerve crosses the superior thyroid pedicle below the plane of the upper pole apex—classified as Cernea type 2B—was identified as carrying a high risk of injury.
– Although this configuration was initially reported in approximately 14% of cadaveric dissections by the University of São Paulo group [1], later clinical series by Gianlorenzo Dionigi et al. demonstrated that this “high-risk” anatomy may be present in up to 54% of patients with large or bulky goiters [2], significantly increasing surgical complexity.
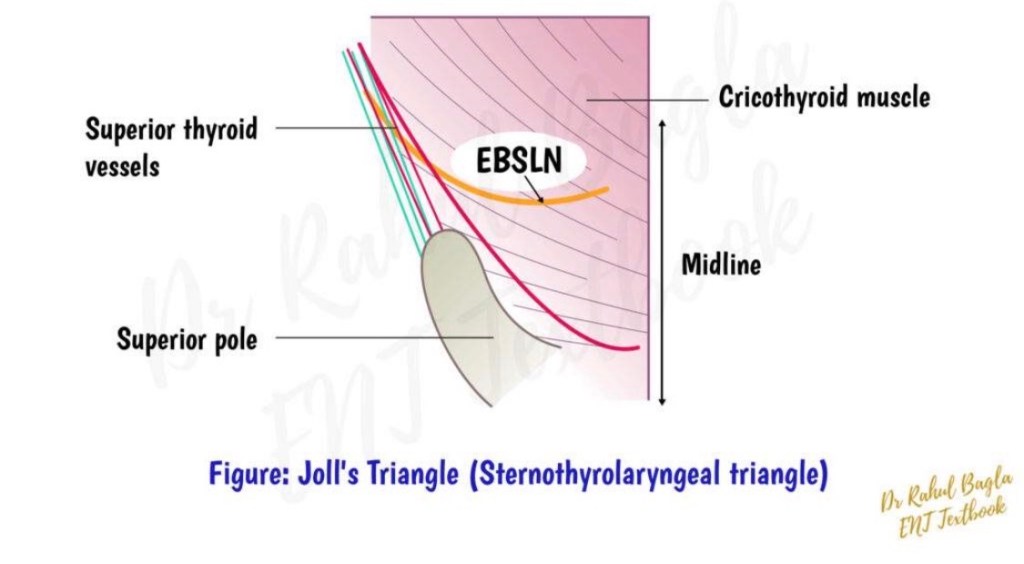
– First popularized by Mossman and DeWeese (1968), Joll’s sterno-thyro-laryngeal triangle remains a valuable anatomical landmark for identifying the EBSLN during superior pole dissection [3].
– In 1986, Michael Friedman provided a detailed description of the surgical approach to the upper thyroid pole that many of us continue to employ in complex cases, particularly when exposure of the EBSLN is critical [4].
– At the supero-external angle of the intermuscular pocket, created to identify the insertion of the sternothyroid muscle on the oblique line of the thyroid cartilage, surgeons frequently encounter a small arterial vessel. While its injury usually causes only minor (though often annoying) bleeding, it serves as an important anatomical landmark.
– These vessels supply the upper portion of the sternohyoid muscle, above the level of the cricoid cartilage.
– According to Wang et al. [5], in approximately 75% of cases, this vessel represents a terminal branch of a common trunk with the cricothyroid artery, originating from the superior thyroid artery. Before bifurcation, this trunk also gives rise to small nourishing branches to the thyrohyoid and omohyoid muscles.
– The so-called “sternohyoid nutrient vessel” is anatomically unique in 56% of cases [5]. After emerging superficially, it enters the (virtual) intermuscular space between the posterior surface of the sternohyoid and the anterior surface of the sternothyroid muscle, following one of two patterns:
✅ coursing along (“hugging”) the lateral border of the sternothyroid muscle, or ✅ directly piercing the most cranial fibers of the sternothyroid muscle.
– Awareness of this vascular anatomy can facilitate safe superior pole dissection, improve EBSLN identification, and ultimately reduce the risk of voice-related complications following thyroid surgery.
References
Cernea CR, et al. Identification of the external branch of the superior laryngeal nerve during thyroidectomy. Am J Surg. 1992. Dionigi G, et al. Surgical anatomy of the external branch of the superior laryngeal nerve. Gland Surg. Mossman HW, DeWeese MS. The surgical anatomy of the larynx. 1968. Friedman M. Surgical management of the superior thyroid pole. Otolaryngol Clin North Am. 1986. Wang C, et al. Vascular supply of the infrahyoid muscles and its surgical relevance. Surg Radiol Anat.