- The most important histologic feature of the primary tumor:
- That affects selection of treatment and eventual prognosis:
- Is its depth of invasion (DOI)
- That affects selection of treatment and eventual prognosis:
- Thin and superficially invasive lesions:
- Have a lower risk of regional lymph node metastasis
- Are highly curable
- Offer an excellent prognosis
- Thicker lesions that deeply infiltrate the underlying soft tissues:
- Have a significantly increased incidence of regional lymph node metastasis and an adverse impact on prognosis
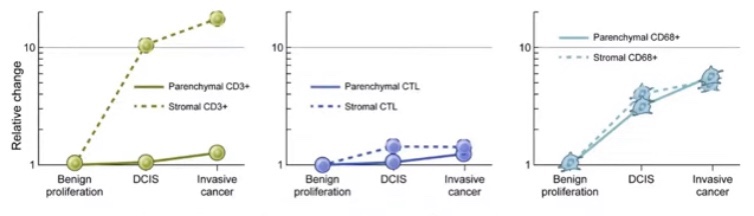
- The risk of lymph node metastasis and survival rates in relation to the DOI of the primary lesion for T1 and T2 squamous carcinomas of the oral tongue and floor of mouth are shown in Figure:
- Although it would be ideal to know the exact DOI of the lesion before surgical intervention, having that information before surgical excision and histopathologic examination of the primary tumor is not possible
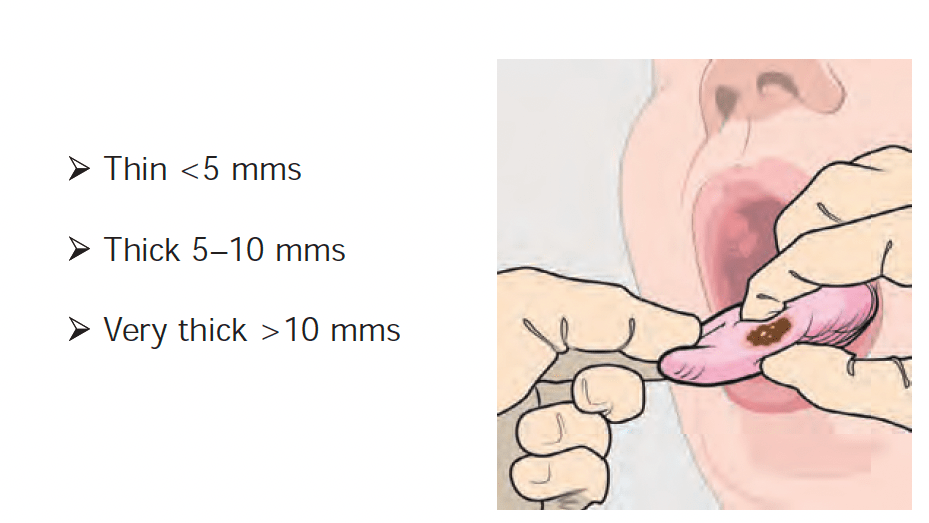
- In general, however, estimate of DOI by assessing thickness of the lesion as appreciated by palpation:
- Is a reasonably good indicator of deeply invasive lesions versus superficial lesions:
- To estimate the extent of soft tissue and / or bone resection for the primary lesion and to decide on the need for elective dissection of the regional lymph nodes at risk in a clinically negative neck
- Is a reasonably good indicator of deeply invasive lesions versus superficial lesions:
- Several retrospective studies have identified DOI of the primary tumor:
- As an important determinant of prognosis:
- Thus DOI is now included in T staging of primary tumors of the oral cavity
- As an important determinant of prognosis:
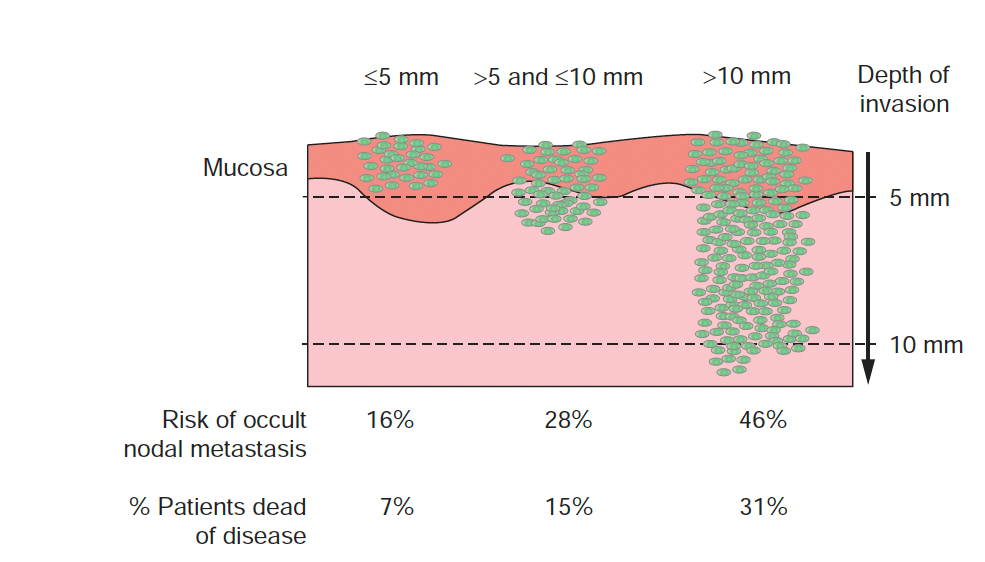
(Memorial Sloan Kettering Cancer Center data, 1985 to 2015).